
Prognostic Value of Right Ventricle-Pulmonary Artery Uncoupling in Cardiac Transthyretin Amyloidosis
pp. 46-54
DOI:
https://doi.org/10.7775/rac.es.v94.i1.20969Keywords:
Cardiac amyloidosis, Right ventricle, TAPSE, Pulmonary systolic pressure, Tissue Doppler, Hospitalization, Heart-PrognosisAbstract
Background: Right ventricular involvement is a common manifestation of transthyretin cardiac amyloidosis (ATTR-CA), especially in advanced stages, and may have significant prognostic implications. Echocardiographic assessment of the right ventricle (RV), however, remains challenging. In this context, the relationship between tricuspid annular plane systolic excursion (TAPSE) and systolic pulmonary artery pressure (SPAP), as well as the relationship between tissue Doppler S wave (S´TDI) and SPAP, have been proposed as markers of RV-pulmonary artery (RV-PA) uncoupling, which could more accurately reflect the functional load on the RV.
Objective: The aim of this study was to analyze the prognostic value of TAPSE/SPAP and S’TDI/SPAP ratios in patients with ATTR-CA, and to compare them with other traditional clinical and echocardiographic predictors regarding the risk of hospitalization for heart failure (HHF).
Methods: A retrospective analysis was performed of patients with confirmed diagnosis of ATTR-CA under outpatient follow up at a cardiomyopathy clinic. Clinical, biochemical, and echocardiographic data were collected at the time of diagnosis, and events of HHF were documented during follow-up. The primary outcome was the first HHF. Univariate and multivariate Cox regression models were applied to identify independent predictors, and Kaplan-Meier analysis were use to evaluate event free survival curves. The optimal cut-off points for continuous variables were defined by Youden's index.
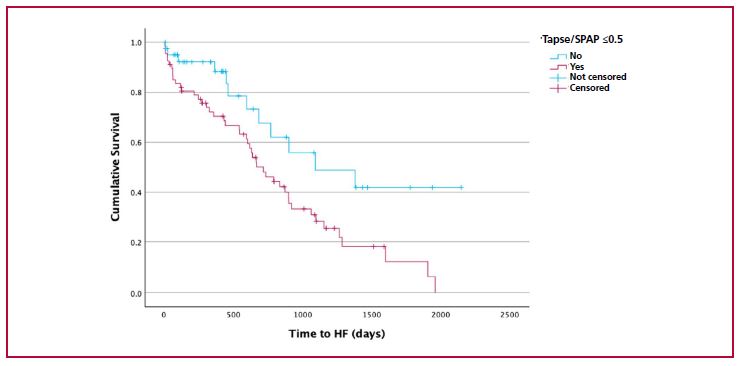
Results: A total of 191 patients (mean age 80 ± 7.9 years, 88.5% men) were included, all with preserved or mildly reduced left ventricular ejection fraction, with a median value of 53% and interquartile range (IQR) 43-61, and echocardiographic evidence of RV dysfunction, with median TAPSE 18 mm (IQR 15–20) and S’TDI 9.5 (IQR 8–10). During a median follow-up of 391 days (IQR 84–704), 32% of patients had at least one HHF. In the univariate analysis, a higher TAPSE/SPAP ratio was associated with lower risk of hospitalization (HR 0.149; p = 0.039), as were higher TAPSE values alone (HR 0.959 p=0.040) and older age (HR 1.066; p=0.010), while SPAP alone was not significant (HR 1.014; p=0.100). In the multivariate analysis, a TAPSE/SPAP ratio ≤ 0.5 (optimal cutoff point with 78% sensitivity, 67% specificity, and area under the ROC curve 0.60) was independently associated with a higher risk of hospitalization (HR 2.05; 95% CI 1.10–4.33; p = 0.025). In contrast, the S’TDI/SPAP ratio showed no independent association (p = 0.843).
Conclusions: In patients with ATTR-CA, RV–PA uncoupling, estimated by a TAPSE/SPAP ratio ≤ 0.5, is associated with an increased risk of HHF, even with preserved ejection fraction. Conversely, the S’TDI/SPAP ratio did not provide prognostic value. Due to its simplicity and availability, the TAPSE/SPAP ratio could be incorporated as a complementary risk stratifica
tion tool in this population
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









