
Plasma Homocyst(e)ine in Acute Coronary Syndrome
pp 181-189
DOI:
https://doi.org/10.7775/rac.v66i2.3506Keywords:
Síndrome coronario agudo, Homocist(e)ína plasmática, Factores de riesgo cardiovasculares, Diseño caso-controlAbstract
Objective
The aim of this study was to assess whether plasma homocyst(e)ine is a risk factor for acute coronary syndrome.
Design
Case-control study.
Material and method
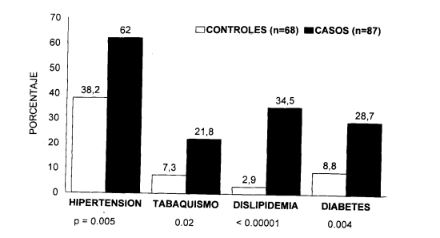
Levels 24-36 hours on set of acute coronary syndrome were compared with the levels in the control safter adjustment for the traditional coronary risk factors. The cases were 53 male and34 female (mean age ± SD 67.45 ± 12.78) hospitalized with either myocardial infarction (n = 24) or unstable angina (n = 63). The patients were matched by sex and age with a group of 68 control subjects (42 male and 26female) clinically free of vascular disease(mean age ± SD 70.02 ± 10.97). We estimated case-control relative risks by quartiles of the plasma homocyst(e)ine levels and tested for linear trends.
Results
Levels of plasma homocyst(e)ine were higher incases than in controls (13.71 ± 7.09 [SDI versus 11.29± 5.23 pmol/1; p = 0.03), after age, cholesterolemia, smoking, hypertension and diabetes were con-trolled for. There was a graded increase in the relative risk of acute coronary syndrome in the second, third, and fourth quartiles of the homocyst(e)ine distribution (relative risk = 1.65, 3.02, 3.26; trend p= 0.005) relative to the first. Of the 87 patients, 15 (17.24%) had homocyst(e)ine levels above the 95th percentile for the controls (20.5μ.cool/1), as com-pared with 4 of the controls (relative risk = 1.49;95% CI: 1.13 to 1.98; p = 0.03).
Conclusions
These findings suggest that hyper homocyst(e)in-emia is a strong and independent risk factor for acute coronary syndrome. Moreover, data suggest that a graded risk for acute coronary syndrome is distributed across the entire distribution of plasma homocyst(e)ine levels.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








