
Recovery from right ventricular dysfunction following revascularization surgery in patients with unstable angina
pp 375-379
DOI:
https://doi.org/10.7775/rac.v60i4.3315Abstract
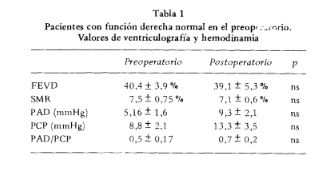
The aim of the study was to investigate the incidence and extent of reversible right ventricular (RV) myocardial disfunction after revascularization surgery (MRS). Methods: 71 consecutive patients with unstable angina and indication of MRS underwent radionuclide ven- triculograms within 24 hours before and 14 days after surgery. Hemodynamic parameters from right side catheterization were obtained before and serially after operation. 38 patients, group A, had abnormal RV function defined as ejection fraction (EF) one SD below minimum normal value. 33 patients, group B, had normal RVEF. Results: there were baseline dif- ferences in number of diseased vessels and LV function between groups. LVEF: group A = 41,7 ± 12 %; group B = 45.3 ± 11 % (p = ns) and wedge pressure (WP): group A = 8.8 ± 2.1 mmHg; group B = 9.7 ± 3 mmHg (p = ns). In group A, preoperative (PE) RVEF was 25.9 :t 6 % and raised to 36 ± 6 % postoperative (PO) (p < 0.01). 83 % entered in normal range. In group B, MRS did not modify RVEF: 40.4 ± 4 % (PE) and 39 ± 5 % (PO). Both groups showed normal RV pressures (P) in PE but group A had early RV hemodynamic disfunction: RAP = 6,5 ± 1.7 mmHg (PE) vs 12.3 ± 3 mmHg (p < 0.05) (PO) and RAP/WP = 0,6 ± 0.15 (PE) vs 1.04 ± 0.3 (PO) (p < 0.05). These results seem to indicate that: 1) low RVEF was not due to LV failure; 2) the group with depressed RVEF had normal pressures in PE; 3) most patients with RV disfunction normalized in the late study although transient hemodynamic abnormalities were seen in PO in this group. The high reversibility of RV disfunction might indicate a better tolerance of this chamber to ischemic insult.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









