
Fibrinolitics Versus Primary Angioplasty in the Acute Myorcardial Infarction
pp 17-26
DOI:
https://doi.org/10.7775/rac.v64i1.3161Keywords:
Myocardial infarction, Thrombolysis, AngioplastyAbstract
Background Percutaneous transluminal coronary angioplasty has became an alternative to thrombolytics as initial approach in the treatment of acute myocardial infarction. The purpose of this study was to deter-mine if: 1) primary percutaneous transluminal coronary angioplasty was feasible in our media and 2) it could improve the clinical angiographic outcome. Method Patients within 12 hours of an acute myocardial infarction, eligible for thrombolysis were included.Exclusion criteria were cardiogenic shock andLBBB. The primary end points were 50% reduction of ST elevation in the EKG at 120 minutes after randomization and the presence of TIMI 3 flow in the infarct-related artery in the angiogram prior to dis-charge. A composite of in-hospital clinical majors events (death, extension of myocardial infarction, development of heart failure, non fatal stroke, major bleeding and need for urgent revascularization) was a secondary end point. In order to evaluate if the delay in the beginning of percutaneous trans-luminal coronary angioplasty therapy was accept-able, all the intervals were carefully assessed. Results From 10/93 to 3/95, 85 patients were randomized streptokinase 1,500,000 U (41 patients) or primary percutaneous transluminal coronary angioplasty (44 patients). Baseline clinical and infarct location characteristics were similarly distributed in both groups.The mean age was 67 ±12 years, with 70% male gen-der. The time from the onset of symptoms to randomization was 246 ±132 minutes for percutaneous trans-luminal coronary angioplasty and 236 ± 149 for streptokinase (P: NS). From randomization to the beginning of the assigned treatment, the interval was 64± 31 minutes for percutaneous transluminal coronary angioplasty and 19 ±48 for streptokinase (P <0.05). Achievement of the primary end point from the beginning of treatment was significantly shorter for percutaneous transluminal coronary angioplasty compared with streptokinase (29 ± 24 minutes ver-sus 59 ± 38 minutes [P < 0.05]).The angiographic success for percutaneous transluminal coronary angioplasty was 93%. Resolution of ST at 120 minutes was 75% for percutaneous transluminal coronary angioplasty and 51% for streptokinase (P <0.05). In-hospital mortality was 9% for percutaneous transluminal coronary angioplasty and 12% for streptokinase (P: NS). Angiographic follow up was obtained in 90% of the patients.TINE3 flow was found in 94% for percutaneous transluminal coronary angioplasty and 70% for streptokinase (P <0.05). The combined end point of in-hospital clinical majors events was 13.6% for percutaneous trans-luminal coronary angioplasty and 31.7% in streptokinase group (P: NS). Thus event free in-hospital survival was 86% for percutaneous transluminal coronary angioplasty and 68% in streptokinase (P: NS). Conclusions 1) In this study primary percutaneous transluminal coronary angioplasty was feasible and as safe as streptokinase. 2) Percutaneous transluminal coronary angioplasty showed a significantly: a) greater resolution in ST changes and b) greater incidence of TIMI 3 flow at the infarct related artery prior to discharge, than streptoquinase. 3) In-hospital event free survival showed a tendency to be better with percutaneous transluminal coronary angioplasty.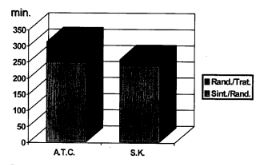
Downloads
Published
2026-03-12
Issue
Section
ORIGINAL ARTICLES
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









