
Development of a Prediction Model for Mortality in Patients with Positive Serology for Chagas Disease: Argen-CHAG Score
pp. 413-422
DOI:
https://doi.org/10.7775/rac.es.v93.i6.20944Keywords:
Chagas, Mortality, Score, PrognosisAbstract
Background: Infection with Trypanosoma cruzi, the etiological agent of Chagas disease, is endemic in 21 countries in the Americas and affects more than 7 million people. With an annual incidence of 30 000 cases and 12 000 deaths, it remains a critical public health challenge. Despite its impact, prognosis remains difficult to establish, and the predictive tools available are limited and poorly validated. Although Rassi et al. developed a mortality prediction model in Brazil, there are significant differences in cardiac involvement between Brazil and Argentina, so there are no validated models for the Argentine population.
Objectives: This study aimed to evaluate predictors of long-term mortality in the population infected with Trypanosoma cruzi who attend a public hospital in the city of Buenos Aires, and to develop a prognostic score for this population.
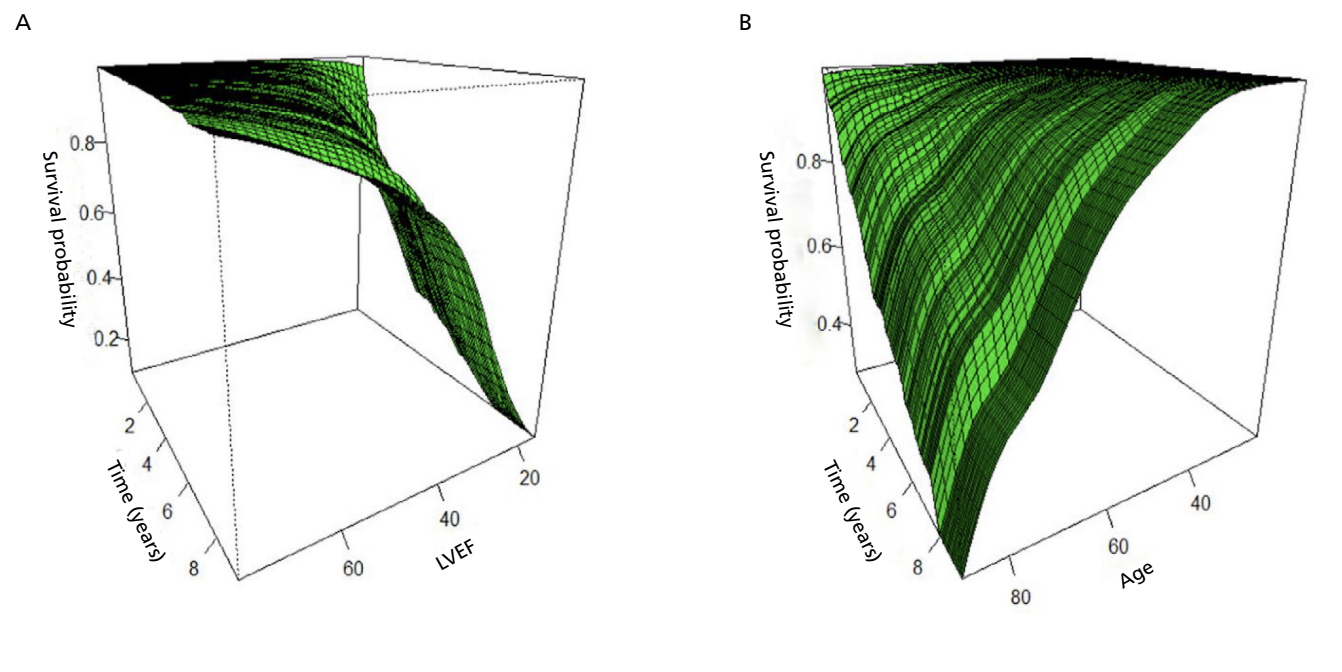
Methods: It included patients aged over 18 years with positive serology for Chagas disease who were evaluated at the Cardiology Division Chagas Program of a public hospital in Buenos Aires. Participants underwent clinical evaluation, ECG, echocardiography, and 24.h Holter monitoring. Follow-up data were obtained by reviewing the Unified Medical Records of the City of Buenos Aires and through telephone interviews with patients or relatives. A derivation group was established assessing prognostic clinical, electrocardiographic and echocardiographic variables related with time to death using a Cox proportional hazards model. Independent predictors of mortality were identified and a score was generated which was subsequently applied to a validation group. The model’s predictive capacity for 5- and 8-year mortality was evaluated using ROC curves.
Results: Among a total of 603 patients, 422 were assigned to the derivation group and 181 to the validation group. During a median follow-up of 6.6 years, 63 deaths in the derivation group and 20 in the validation group were observed. Three independent predictors were found: age, left ventricular ejection fraction (these two variables were rescaled into several categories), and history of implantable cardioverter-defibrillator. Each was assigned a score proportional to the hazard ratio. A risk score was calculated for each patient and divided into three categories: 1) low risk: score 0-4 points, 2) moderate risk: score 5-12 points, and 3) high risk: score ≥ 13 points.
Survival was 12.5% at 6.3 years in the high-risk group, 67% at 8.75 years in the moderate-risk group, and 92% at 8.7 years in the low-risk group. The area under the curve for predicting death was 0.89 and 0.85 at 5 and 8 years, respectively.
Conclusion: The risk score proved highly effective, as it presented high prognostic accuracy based on only three predictors, which are easily accessible in clinical practice. This tool could contribute significantly to risk stratification and decision-making in resource-limited settings, especially in regions where the disease is endemic and existing models do not adequately reflect the local characteristics of the population.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









