
Antiplatelet Therapy Guided by Platelet Function Testing after Successful Percutaneous Coronary Intervention
DOI:
https://doi.org/10.7775/rac.es.v80.i5.870Keywords:
Angioplasty, Balloon, Coronary, Stents, Platelet Aggregation InhibitorsAbstract
Background
Dual antiplatelet therapy with aspirin and clopidogrel is an essential treatment to prevent ischemic events in patients
undergoing percutaneous coronary intervention (PCI). However, a significant interindividual variability exists in response to clopidogrel treatment, which is responsible for failure in the therapeutic effect and in the development of high residual platelet reactivity (HRPR). Prasugrel could reduce this prothrombotic state.
Objectives
To evaluate: 1) the antiaggregant response in clopidogrel or prasugrel pretreated patients undergoing successful PCI, and 2) the response to prasugrel loading in patients with low residual platelet reactivity on clopidogrel therapy.
Material and Methods
Eighty three patients were prospectively included in the study. They underwent successful PCI under dual anti- platelet therapy: aspirin plus clopidogrel (600 mg loading dose or a maintenance dose of 75 mg for more than 7 days; n=42) or prasugrel (60 mg loading dose or a maintenance dose of 10 mg for more than 7 days; n=41). The selection of thienopyridine was left at the discretion of the treating physician. Patients with high hemorrhagic risk were excluded. Platelet function was tested 12-24 hours after PCI with the VerifyNowTMP2Y12 Assay. High residual platelet reactivity (HRPR) was defined as P2Y12-reaction units (PRU) ≥ 230. In case of HRPR, patients received a loading dose of prasugrel 60 mg and platelet function was reassessed 2 hours later.
Results
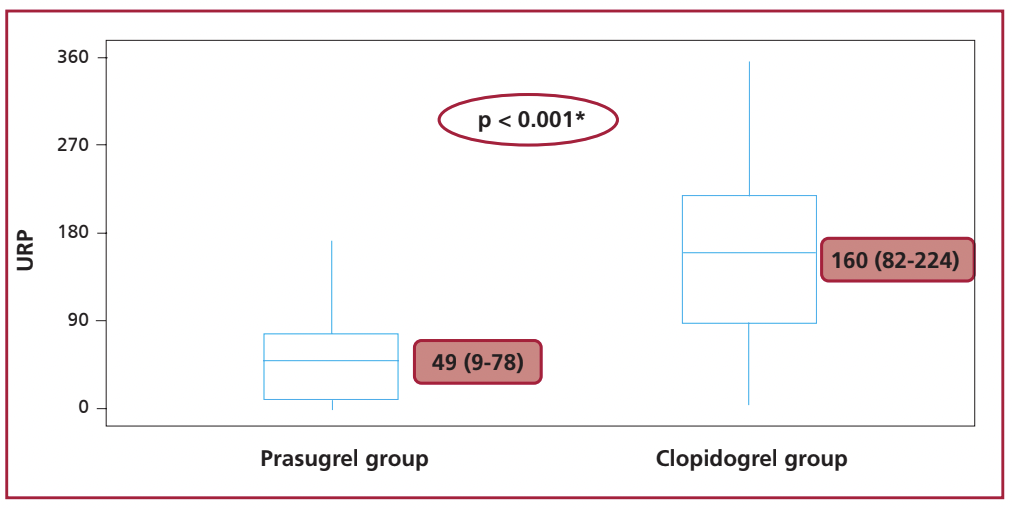
Baseline characteristics did not differ in patients who initially received clopidogrel or prasugrel. At 12-24 hours post PCI, patients treated with prasugrel presented significantly less PRU compared with the clopidogrel cohort (median 49 (9-78) vs. 160 (82-224); p < 0.001). HRPR was observed in 24% of patients in the clopidogrel group and in no patients in the prasugrel cohort (p < 0.001). All patients with HRPR on clopidogrel treatment corrected this value
after the loading dose of prasugrel.
Conclusions
After successful PCI, prasugrel administration achieved greater platelet inhibition compared to clopidogrel. Moreover, in patients with high-on treatment platelet reactivity with clopidogrel, optimal platelet inhibition was accomplished by additional prasugrel administration.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









