
Comparison Between High and Moderate Dosis of Amiodarone Asociated or not with Beta-Blockers in Patients with Arrhythmias During Acute Myocardial Infarction Evolution
pp 191-200
DOI:
https://doi.org/10.7775/rac.v66i2.3507Keywords:
Amiodarona, Betabloqueantes, Arritmias, Infarto agudo de miocardioAbstract
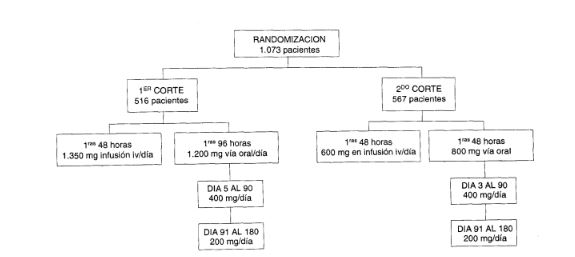
In the GEMICA project, study of the use of amiodarone in the treatment of acute myocardial infarction, two different doses of amiodarone were used. The first 537 patients were given an intravenous dose of 2,700 mg amiodarone or placebo, together with 1,200 mg per Os, over the initial 48hours, and for the following 30 days a dose of 400mg per Os. Keeping to the same time frame, a second group of 536 patients was given an initial intravenous dose of 600 mg amiodarone, together with 800 mg per Os, and 400 mg per Os thereafter.
Objective
To analyse the relation between the incidence of arrhythmia during the first 30 days of acute myocardial infarction evolution and the administration of high doses or moderate doses of amiodarone, either in association with betablockers or without them.
Material and method
The 513 patients treated with amiodarone were divided into 4 groups according to the doses they received:A) high doses of amiodarone with betablockers; B) moderate doses of amiodarone with betablockers; C)high doses without betablockers; D) moderate doses without betablockers. The following variables were analyzed: a) size and location of acute myocardial infarction; b) non fatal arrhythmia; c) sustained ventricular tachycardia; d)ventricular fibrillation; e) asystolia or severe bradycardia;f) atrial fibrillation; g) atrial flutter; h) other supraventricular arrhythmia; i) new conduction disorders; j) use of a transitory pacemaker; k) sudden death. Statistical analysis was based on the chisquared methods and on Student t-test, taking a p value of = 0.05 to be significant.ResultsWe compared the four groups and a higher incidence of new conduction disorders (p = 0.01) and sudden death (p = 0.02) was observed among patients treated with high doses of amiodarone (groups A and C). Compared with group B, group A evidencied a higher incidence of new conduction disorders (p =0.01) and a tendency to increased asystolia and sud-den death (p=0.06). In the comparison of groups C and D, the group with moderate doses of amiodarone without betablockers (group D) revealed a lower incidence of sudden death (p = 0.05) but a higher rate of non fatal arrhythmias (p = 0.05). Finally, comparison of high doses and moderate doses groups, without taking with account the presence or absence of betablockers, showed an increase in new conduction disorders cases (p=0.04; odds ratio 1.89; confidence index 95% 0.97-3.71) and number of sud-den deaths (p= 0.003; odds ratio 14.3; confidence in-dex 95% 1.95-295.8) in the high doses group.
Conclusions
1. The association of amiodarone with betablockers gives better results when moderate doses amiodarone is administered because it has demonstrated no significant incidence of adverse effects and to reduce the severe ventricular arrhythmics events without to increase the mortality during the firs post-acute myocardial infarction 30 days. 2. The incidence of a new conduction disorders and sudden death is lower with moderate doses amiodarone than with high doses. 3. The high doses of amiodarone associated or not to betablockers increase the incidence of new conduction disorders and sudden death. In a post acute myocardial infarction patients with betablockers therapy, moderate doses of amiodarone might be used if arrhythmias are present, despite of to reduce the non-fatal severe ventricular arrhythmias.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








