
A multicenter study of radioisotope ventriculography with Tc-99m and intravenous dipyridamole at conventional and high doses in patients with chronic coronary artery disease
pp 464-476
DOI:
https://doi.org/10.7775/rac.v60i5.3442Abstract
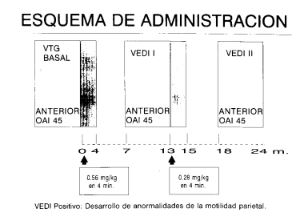
The aims of this study were: 1) assess the sensitivity of radionuclide angiography after dipyridamole; 2) its relationship with exercise parameters; 3) evaluates the sensitivity, specifity, positive and negative predictive values of the development of angina, downslope of ST depression ~ 1.5 mm and the decrease of ejection fraction ~ 5 points during radionuclide angiography after dipyridamole; and 4) observe the mechanisms of ischemia develo ping through the rate pressure product during exercise and radionuclide angiography after dipyridamole. We prospective studied 100 patients with chronic stable coronary artery disease with both exercise radio nuclide angiography and radionuclide angiography after dipyridamole. Patients were included only if they had a new abnormal regional wall motion and decrease or no increase of the ejection fraction at exercise radio- nuclide angiography. After a rest period of one hour dipyridamole 0.56 mg/kg/4 minutes were infunded and images collected, if there were no new wall motion abnormalities, a second radionuclide angiography infusing dipyridamole 0.28 mg/kg/2 minutes was obtained and new images collected again. Criterion of positively for radionuclide angiography after dipyridamole was development of regional wall motion abnormalities. Global sensitivity was 61 % for the first radio- nuclide angiography with dipyridamole (0.56 mg/kg/4 minutes). And 68 % for the second (dipyridamole 0.28 mg/kg/2 minutes). By the analysis of the median we defined patients with "low ischemic response" when they had ischemic exercise radio nuclide angiography at rate pressure product, or mets greater than the median, and ejection fraction or regional wall motion score equal or lower than the median. Patients with these criteria were "Group A" ("low ischemic response"), and conversely "Group B" ("high ischemic response"). Sensitivities (percentage) for rate pressure product, mets, decrease of ejection fraction, and fall of regional wall motion score parameters was: Group A ("low ischemic response): 34, 21, 36 and 49%, for first radio- nuclide angiography with dipyridamole (0.56 mg/kg/4 minutes), and 45, 36, 54 and 59 % for the second (dipyridamole 0.28 mg/kg/2 minutes) respectively. Group B ("high ischemic response"): 96, 90, 83 and 78 % for first the radionuclide angiography with dipyridamole (0.56 mg/kg/4 minutes), and 98, 91, 85 and 80 % for the second (dipyridamole 0.28 mg/kg/2 minutes) respectively. The sensitivity, specifity, positive and negative predictive values were: angina development: 57, 64, 73 and 48 %. Downslope of ST depression ≥ 1.5 mm values was: 41,92,91 and 48%. Considering both together (development of angina and downslope of ST depression ~ 1.5 mm) values were: 49, 100, 100 and 54 %. The decrease of ejection fraction ≥ 5 points during radio nuclide angiography after dipyridamole, had 38, 98, 96 and 48 % respectively. The rate pressure product values for positives first radionuclide angiography with dipyridamole was 8996 ± 2872 and 9404 ± 2270 for the negatives (no significant statistics' differences founded). When positive radionuclide angiography after dipyridamole rate pressure product values were compared with exercise, significant differences were founded in both first radionuclide angiography with dipyridamole (8896 ± 2550 vs 16804 ± 4034) and second radionuclide angiography with dipyridamole (9357 ± 2872 vs 19628 ± 6012) with p value < .0001. We conclude that radionuclide angiography after dipyri- damole asensitivity depended on exercise parameters with sensitivity in Group A while the second radio nuclide angiography after dipyridamole (0.28 mg/kg/2 minutes) only increased sensitivity in Group B, and that the mechanism of dipyridamole producing ischemia is not the increase in oxygen consumption. This test may be useful in patients unable to perform exercise tests.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









