
Impact of a Treatment and Intensive Care Program in Heart Failure Management
pp 384-392
DOI:
https://doi.org/10.7775/rac.v69i4.3080Keywords:
Chronic heart failure, Therapy, Non-pharmacological management , PrognosisAbstract
Despite of major advances in the pharmacotherapy of chronic heart failure (CHF), hospitalization and mortality rates remain high, related to low compliance with prescribed therapeutic regimen and sub-optimal use of effective medications.
Objective To evaluate the impact of an intensive care program (ICP) based in prescribed drugs as well as outcome in patients with CHE.
Material and methods Between 02/97-02/00, 157 patients with CHF were prospectively included in an ICP as outpatients. Mean follow-up was 12 months.
Results Sixty-nine percent of the cohort showed an EF < 30% or NYHA functional class III-Iv. Etiology of CHF was coronary artery disease in 54%. Medications used before of after ICP inclusion were ACE-inhibitor/ angiotensin antagonist in 79% and 93% (p < 0.001) before and after ICP inclusion respectively; diurectis 62.4% versus 86.6% (p < 0.001), digoxin 46.5% ver- sus 49.7% (p = ns) and betablockers 29.9% versus 43.9% (p = 0.013). During follow-up, 65 patients (41 %) were hospitalized, 42 patients (27%) had a diagnosis of decompensated heart failure. Mean NYHA class before inclusion in the ICP was 2.4 and decreased to 1.87 during follow-up (p < 0.001). Mortality rate was 9.6% (15 patients) and 24-months cumulative survival was 75%. In multiple logistic regression analysis NYHA functional class during follow-up (p = 0.0005; OR = 4.6; CI 95% = 1,9-10.8) and diabetes (p = 0.019; OR = 4.2; CI 95% = 1.2-14.1) were independent predictors of mortality. Conclusions CHF management in intensive care program showed an increased prescription rate of recommended drugs, with improvement of NYHA class. During follow-up, 1 in a group of 4 patients had to be hospitalized because decompensated CHF and the 2-year survival rate, for this high-risk patients was 75%. Functional class during follow-up and diabetes were independent markers of death.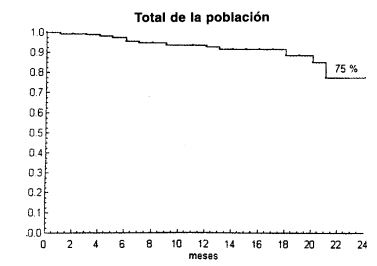
Downloads
Published
2026-03-02
Issue
Section
ORIGINAL ARTICLES
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








