
5-Fluorouracil-Induced Reversible Cardiogenic Shock
pp 253-254
DOI:
https://doi.org/10.7775/rac.es.v89.i3.20225Abstract
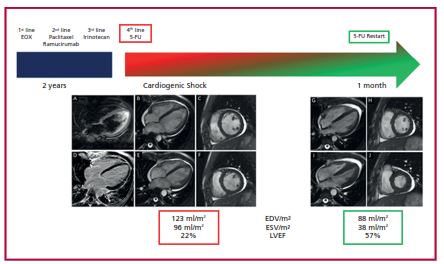
5-Fluorouracil (5-FU) is a fluoropyrimidine (FP) antimetabolite agent used broadly in the treatment of a variety of solid tumors, and is only second to anthracyclines in terms of incidence of cardiotoxicity. Coronary vasospasm is its main cardiotoxic mechanism manifested as precordial pain associated with transient electrocardiographic (ECG) changes, rarely causing myocardial infarction. However, there are other rare manifestations of cardiotoxicity, such as dilated cardiomyopathy, ventricular arrhythmia, and sudden death. We describe a case of cardiogenic shock following 5-FU infusion. This is a 35-year-old patient with a history of stage IV gastric adenocarcinoma. Throughout his specific treatment, the patient completed several chemotherapy regimens: EOX (epirubicin -cumulative dose 324mg/m2-, oxaplatine, and capecitabine) as firstline
therapy; paclitaxel / ramucirumab as second-line therapy, and irinotecan as third-line therapy (Figure 1). During those regimens, the patient had no signs of cardiotoxicity; transthoracic echocardiography (TTE) revealed preserved left ventricular ejection fraction (LVEF) (>55%), with normal global longitudinal strain (<18%, normal range: - 19% ± 2%). Finally, a fourth-line therapy with FOLFOX(5-fluorouracil, oxaplatine and folinic acid) in continuous infusion was started. During the first 5-FU infusion, the patient presented typical precordial pain associated with ECG transient ST-segment elevation, which disappeared once the drug was discontinued. No high-sensitivity troponin T elevation was detected. This event was interpreted as coronary vasospasm. The patient was discharged under diltiazem therapy. Forty-eight hours later, the patient was admitted in the emergency room with a second episode of precordial pain associated with diaphoresis and dizziness. Physical examination showed an awake, hypotensive patient with signs of poor peripheral perfusion. Lab tests on admission revealed acute kidney failure, with increased cardiac biomarkers: high-sensitivity troponin: 20 pg/mL (normal <15 pg/mL), NT-proBNP: 3000 pg/mL (normal 125 pg/mL), and increased blood lactic level: 3 mmol/L. The ECG showed no acute ischemic changes. TTE revealed slightly increased LV diameters, with global hypokinesis and severe LVEF
impairment: 25%. In the Cardiac Intensive Care Unit (CICU), the patient required vasopressors, with clinical improvement in 48 hours. Cardiac magnetic resonance imaging (MRI) confirmed diffuse hypokinesis and severe ventricular dysfunction (LVEF 22%), with no myocardial edema in T2-weighted sequences. Late gadolinium enhancement (LGE) sequences ruled out myocardial fibrosis (Figure 1). The patient made good progress and was discharged 5 days later under beta-blockers and angiotensin-converting enzyme inhibitors. LVEF gradually improved during follow-up in the Cardio-Oncology Unit, reaching full recovery (LVEF: 55%) at 15 days.
This recovery was confirmed by MRI, showing 57% LVEF at 1 month (Figure 1). After LVEF recovery, a multidisciplinary team decided to continue treatment with 5-FU. The 5 pending chemotherapy cycles were completed in the CICU under continuous monitoring, with no further cardiac complications. We have described the case of a young male patient with no cardiovascular history, who presented cardiogenic shock following 5-FU infusion. The most common 5-FU-related adverse events include mucositis, diarrhea, and myelosuppression. Cardiotoxicity is a severe adverse effect causing from electrocardiographic changes in asymptomatic patients to transient angina, myocardial infarction, or even lifethreatening cardiogenic shock. The exact mechanism of cardiotoxicity remains unclear, although several mechanisms from animal models, case reports, and small clinical studies have been proposed. Coronary spasm and acute myocardial ischemia are the best-described adverse effects of fluoropyrimidines, manifested as precordial pain, ischemic ECG changes, and increased biomarkers as high-sensitivity troponin. Two mechanisms have been proposed to explain this phenomenon. Mosseri et al. found that protein kinase C could mediate vasoconstriction, and demonstrated endothelium-independent vasoconstriction with increasing doses of 5-FU in an animal model. (1) In addition, increased concentration of endothelin-1, a potent vasoconstrictor, was detected in patients with 5-FU-induced
cardiotoxicity. (2) Our patient reported 5-FU-induced precordial pain 48 hours before the episode of cardiogenic shock. However, no high-sensitivity troponin elevation was detected, and MRI evidenced no signs of myocardial ischemia, since it showed global hypokinesis with no signs of edema in T2-weighted sequences, and no fibrosis in LGE sequences. Vasospasm was therefore ruled out as the underlying mechanism causing ventricular dysfunction. Direct toxic effect of 5-FU on cardiomyocytes is another proposed mechanism. Alpha-fluoro-beta-alanine (FBAL), a degradation product of 5-FU, plays a key role in this regard. In a case report, Muneoka et al. demonstrated increased concentrations of FBAL in patients with 5-FU-induced cardiotoxicity. No cardiac symptoms occurred after the initiation of the prodrug S-1 administration (an oral fluoropyrimidine that lacks FBAL as a metabolite). (3) Endothelial dysfunction and inadequate oxygen delivery constitute another proposed mechanism. Vascular
dysfunction associated with microthrombi formation is a mechanism that could potentially cause cardiotoxicity. Microthrombiocclusion is usually undetected by coronary arteriography. (4) However, in our patient, we were unable to demonstrate evidence of microvascular obstruction by MRI on LGE sequences. Use of anticoagulation therapy has been suggested to mitigate this adverse effect, but further research is required to standardize their indication. Some authors believe free oxygen radicals could also play a role in cytotoxic endothelial dysfunction. (5) The last mechanism was described by Spasojevic who demonstrated that 5-FU causes changes to the erythrocyte membrane leading to increased blood fluidity and conversion of the erythrocyte from its usual biconcave shape to an echinocyte shape. The resulting membrane changes diminish the erythrocyte ability for oxygen transportation, resulting in myocardial ischemia and injury. (6) In our patient, it was not possible to recognize a single pathophysiological mechanism to explain LV dysfunction, but we believe that it is due to a combination of several factors. There is no standard treatment available for fluoropyrimidine-induced cardiotoxicity. Current consensus indicates 5-FU treatment
discontinuation in case of suspected cardiotoxicity. In case of vasospasm, the patient should be treated symptomatically with antianginal drugs (nitrates or calcium blockers, such as diltiazem), to abort the symptoms and prevent recurrences. LV dysfunction should be initially treatedaccording to international guidelines. In some cases, cardiotoxicity is reversible after drug discontinuation,
as occurred in our patient. A multidisciplinary approach by cardiologists and oncologists is crucial when managing this type of patients and making decisions about whether or not to continue treatment. Repeating treatment with 5-FU after cardiotoxicity implies a high risk of recurrence, between 82% and 100%. Our patient completed the remaining 5-FU cycles under careful monitoring in the CICU. We believe our case is important to emphasize the diverse clinical manifestations, other than vasospasm, of 5-FU-induced cardiotoxicity, to be taken into account when planning strategies for patient monitoring. Myocardial dysfunction and cardiogenic shock may be manifestations of reversible 5-FU-induced cardiotoxicity, and seem to be independent of coronary vasospasm. It is essential to be aware of this adverse effect in these patients’ follow-up.Conflicts of interest
None declared.
(See authors’ conflicts of interest forms on the website/Supplementary material).
Ethical considerations
Not applicable
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








