
Ischemic Cardiomyopathy with Poor Ventricular Function: Surgical Options
pp 143-150
DOI:
https://doi.org/10.7775/rac.v65i2.3471Keywords:
Cardiac insufficience, Revascularization, TransplantAbstract
Background
The present study evaluated the early and late results of coronary artery bypass grafting and heart transplantation in patients with ischemic cardiomyopathy and ejection fraction <_25% and investigated the factors that allow to identify which group of patients do not benefit with coronary operation.
Material and method
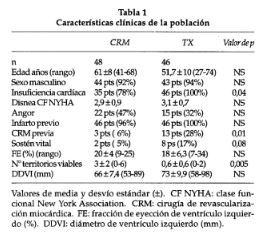
Ninety four patients (87 men and 7 women) with mean age 55.4 ± 20 years were evaluated. Two groups were analyzed: 48 patients (51%) with coronary artery bypass and 46 (49%) with heart trans-plantation. The patients were followed-up for 3years.
Results
The early mortality was similarly in both groups, 10.4% (5 patients) in coronary artery bypass group versus 17% (8 patients) in heart transplantation group. The mean follow-up period was in coronary artery bypass group 24 ± 10 months and in the heart transplantation group 28 ±12 months (p = 0.6). The actuarial survival without early mortality was in the first year 95% versus 89% (p = 0.9) and in the third year 84.8% versus 85% (p =0.9). The New York HeartAssociation functional class improved in the two groups from, 2.9 ± 0.9 to 1.1 ± 0.1 (p = 0.001) in the coronary artery bypass group and 3.1 ± 0.7 to 1.2 =0.2 (p = 0.001) in the heart transplantation group.Left ventricular ejection fraction increased from 20± 4% to 30 ± 7% (p = 0.001) in the coronary artery bypass group and 18 ±6.3% to 58 ±12% (p = 0.0001) in the heart transplantation group. The number of segments with vaibility was associated with the improvement of the ejection fraction. The New York Heart Association functional class was predictive of late mortality in the univariate and multivariate analysis (2.4 ± 0.9 versus 3.5 ± 0.7; p = 0.01, p = 0.03). The ejection fraction 22 ± 6 versus 18 ± 3 (p = 0.04) and left ventricular end-diastolic dimension 63 ±8.9 mm versus 75 ± 8 mm (p = 0.04) was predictive of poor prognosis in the univariate analysis.
Conclusions
There were no differences in early and late mortality between the two groups. Both treatments improved the New York Heart Association functional class and the ejection fraction. Thus, the coronary artery bypass grafting should be considered the first election. A poor New York Heart Association functional class, enlargement of left ventricular end-diastolic dimension and low ejection fraction may predict unsuccessful revascularization.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.








