
Analysis of ST segment depression in lead D3 in anterior transmural MI: simplified approach to procedures of precordial ST mapping
pp 163-170
DOI:
https://doi.org/10.7775/rac.v58i4.3367Abstract
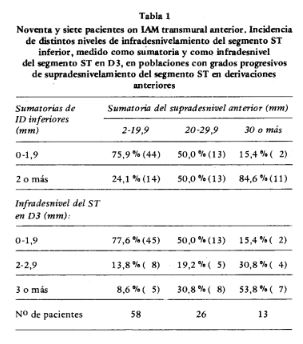
In a previous research work we demonstrated that patients with acute anterior transmural myocardial infarction develop significant ST segment depression at lead D3 in 34.7%, end that such ECG abnormality is related with ST segment elevation at lead aVL, infarcts with greater number of new Q waves and worse clinical evolutions and blocks. In a selected population of 97 patients with a clinical history of such type of infarction we studied the relationships between the clinical behavior of patients during hospitalization and the following electrocardiographical findigns: 1) ST segment elevation levels at the precordial leads, including leads D 1 and a VL (anterior leads); 2) ST segment depression levels at leads D2-D3- aVF (inferior leads); 3) ST segment depression at lead D3. Acute anterior transmural myocardial infarction (MI) was diagnosed on the basis of now Q (0.04 sec or more) or QS waves together with segment elevation at the anterior leads (precordial leads V1-V6), with or without such ECG findings at D1-aVL, together with typical anginal-pain prolongued for more than 10 minutes, and/or peak CPK enzyme levels above 50% the upper normal values. Patients with previous cardiac damage, ischemic or not, with concurrent involvement of the inferior wall of the left ventricle, with ECG findings of either fibrosis or hypertrophy of the ventricles, complete left bundle branch block, or with references of pericardial friction rubs were not included in the study. A deviation from the isoelectric line at 0.08 sec from the] point equal or greater than 2 mm was required for diagnosing either significant ST segment elevation or depression, and determination of the level of ST segment deviation was done by addition of the distances of deviations at each lead with significant changes. Practice of measurement were done in the ECG with greater ST segment elevation at the precordial leads by an independent observer. Clinical evolution of patients was studied by including the patient into one of the following groups: 1) death patients; 2) patients developing cardiac heart failure (those in Killip and Kimball class III and IV, chest X-ray corroboration of radiologycal signs of interstitial or alveolar edema being a desirable criteria); 3) patients developing high risk cardiac arrhythmias, as defined by Surawicz, Madsen and Luria; 4) patients without in- hospital serious cardiac events, including those in Killip and Kimball class I and II, patients with isolated first degree atrioventricular block between 0.20-0.24 seconds, intraventricular conduction disturbances (complete left bundle branch blocks excluded patients from the study), and patients with extrasystolia of any type. We also investigated the real incidence of cardiac pump failure and of dangerous cardiac arrbythmias in each group. A X2 test was applied in order to establish differences among groups, and values for P equal or inferior to 0.05 were considered significant for dif ferences. There is a direct linear correlation between tbe ST segment elevation levels at tbe anterior leads and tbe levels ofinferior deviation of tbe ST segment at tbe inferior leads (P inferior to 0.000.25). Tbis correlation bas tbe same value for P wben comparing ST segment anterior elevation levels witb incidence of ST segment depression at lead DJ alone. Tbe discriminant prognostic capability of tbe ECG by analysis of tbe reciprocal ST segment cbanges during MI increases witb tbe following procedures: 1) ST segment elevation levels at tbe leads exploring tbe anterior wall oftbe left ventricle (P: 0.5-0.4); 2) ST segment inferior deviation levels from tbe isoelectric line at leads D2-DJ-aVF (P: 0.05- 0.025); J) level of ST segment depression at isolated lead DJ (P: 0.01-0.005). (...)
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









