
Pulmonary Perfusion Scentellography in Total or Partial Right Ventricular By-Pass
pp 151-163
DOI:
https://doi.org/10.7775/rac.v62i2.3336Keywords:
Pulmonary perfusion, Scintigraphy, Total bypass: Partial bypass, Congenital heart disease, Pulmonary hypoperfusionAbstract
Background
Since the introduction of the partial right ventricular by-pass in 1958, and of the total by-pass in 1971 to treat complex congenital heart disease with diminished pulmonary flow not subject to other techniques of correction, different technical approaches have been developed. The dynamics of pulmonary flow in these patients has been studied by means of bidimensional echocardiogram and Doppler. However, the venous pulmonary inflow is better quantitated by means of pulmonary scentellography.
Material and method
From 1990 through 1993, 65 patients with age range from Ito 38 years (mean 8.5 years) have been studied with pulmonary perfusion scentellography with Tc99-mMAA in supine position. The studies were performed within the first postoperative year after surgical treatment of complex congenital heart disease with diminished pulmonary flow:atrioventricular connection in 36, congenital cardiopathy with hypoplasia of the right or left ventricle in 25 and 4 not subject to biventricular correction. The restriction to pulmonary flow was secondary to stenosis or pulmonary atresia in 54, Ebstein's anomaly with hypoplasia of the right ventricle in 4 and binding of the pulmonary artery in7.
Results
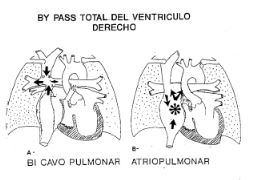
Twenty-three patients with total by-pass were classified into: a) atriopulmonary by-pass (13 cases);b) total cavopulmonary by-pass (4patients); c) cavoatriopulmonary by-pass: directional cavopulmonary and atriopulmonary by-pass in 4 patients; d) Kawahisma's technique in 2 patients. Partial by-pass was performed in 42 patients falling into the following classification: a) bi-directional cavopulmonary anastomosis in 29 patients (23 pulsatile or hyperpulsatile); b) classical Glenn in3 patients; c) partial biventricular by-pass in 10 patients.
Conclusions
Pulmonary scentellography via superior vein showst hat in bidirectional and total cavopulmonary anastomosis, pulmonary perfusion dominates the side- where the correction was performed, unlike the atriopulmon-ary anastomosis in which distribution prove to be homogeneous. This suggests that in the presence of an atrial mix chamber of the systemic venous pulmonary in flow, atriopulmonary an astomosis would be more physiological because a similar flow is maintained in both lungs.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









