
Clinical Predictors of No-Reflow in Percutaneous Coronary Intervention for Acute Myocardial Infarction
pp. 222-227
DOI:
https://doi.org/10.7775/rac.es.v81.i3.1423Keywords:
Myocardial infarction, No-reflow, Percutaneous coronary intervention, reperfusionAbstract
Background: The no-reflow phenomenon in the setting of primary coronary intervention for acute myocardial infarction (AMI) is relatively common and is associated with adverse outcomes. The detection of clinical variables associated with this phenomenon before the procedure might help to adopt preventive measures and thus improve the results.
Objective: The aim of this study was to identify clinical predictors of the no-reflow phenomenon in the setting of percutaneous coronary intervention for ST-segment elevation acute myocardial infarction, prior to the procedure.
Methods: A total of 742 patients with AMI < 12 hours since onset of symptoms treated with primary percutaneous coronary intervention were analyzed. Patients with epicardial TIMI grade 0 flow after the procedure were excluded. No-reflow was considered as the presence of TIMI grade 1-2 flow immediately after the procedure in the absence of residual stenosis. Demographic variables, coronary risk factors, family history and delay to reperfusion were analyzed. Multivariate logistic regression was used to determine the independent prognostic value of the variables associated with no-reflow.
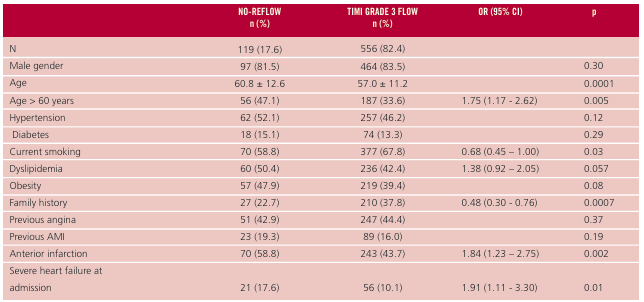
Results: A total of 675 patients were included. The no-reflow phenomenon was present in 119 patients (17.6%). Patients with no-reflow were older (60.8 ± 12 vs. 57.0 ± 11 years; p = 0.0001) and had less prevalence of current smoking (58.8% vs. 67.8%, p = 0.03) and of previous history (22.7% vs. 37.8%, p = 0.0007), with no significant differences in the rest of coronary risk factors and history of cardiovascular disease. Anterior AMI (58.8% vs. 43.7%, p = 0.002), heart failure at admission (17.6% vs.10.1%, p = 0.01) and delay to reperfusion (240 [151-360] vs.195 [120-302] minutes, p=0.02) were more frequent in the no-reflow group. Multivariate analysis identified age > 60 years, anterior infarction and delay to reperfusion > 3 hours as independent predictors of no-reflow.
Conclusion: Advanced age, anterior infarction and delay to reperfusion were independent clinical predictors of no-reflow. The confirmation of these findings in prospective studies might allow the implementation of strategies to prevent this phenomenon and eventually improve the long-term clinical outcomes.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









