
Prognostic Value of Infarct Size Measured by Gated SPECT Scintigraphy
pp. 531-535
DOI:
https://doi.org/10.7775/rac.v83.i6.7130Keywords:
Myocardial Infarction/physiopathology, Cardiac Gated Single-photon Emission Computer Assisted Tomography, PrognosisAbstract
Background: Despite the improved sensitivity and specificity of SPECT myocardial perfusion imagingto detect myocardial involvement after acute myocardial infarction (AMI), there is little information about the usefulness of early infarct size (IS) measurement by this method for risk stratification and prognosis.
Objectives: The goal of this study was to evaluate the usefulness of quantifying IS by gated SPECT scintigraphy to predict cardiovascular events in patients with a first AMI.
Methods: Patients with a first ST-segment elevation AMI were included from 2009 to 2014. Infarct size was estimated using the Cedars QPS software. The incidence of events (heart failure, ventricular arrhythmias, mortality and a composite of the three events) was evaluated at one year.
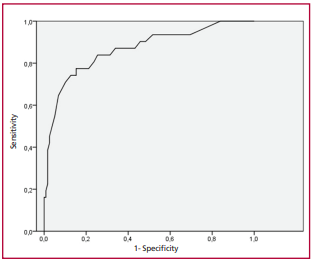
Results: One-hundred and forty nine patients were included in the study; mean age was 59±11 years and 81.9% were men. Diabetes was present in 16.1% of cases, 9.4% had a history of myocardial revascularization, 84.6% were admitted in Killip and Kimball class A, 43% of AMIs were located in the anterior wall and 69.8% of the patients underwent reperfusion. Left ventricular ejection fraction estimated by gated SPECT scintigraphy was 51%±14%. Follow-up was completed in 95.9% of cases. An IS cutoff point of 22% (ROC curve) was established to predict the composite endpoint at follow-up (sensitivity 92%, specificity 81%, AUC: 0.94%), dividing the sample into two groups: Group I (IS <22%) and Group II (IS ≥22%). The prevalence of the composite endpoint was greater in Group II (2.1% Group I vs. 50% Group II; p<0.001). Infarct size ≥ 22% was the only variable identified as predictor of events during followup (OR 1.978; 95% CI 1.887-1.996; p<0.001).
Conclusion: Early quantification of IS by gated SPECT scintigraphy is an independent risk predictor at one year that allows risk stratification in patients with a first AMI.
Downloads
Published
Issue
Section
License
Copyright (c) 2025 Argentine Journal of Cardiology

This work is licensed under a Creative Commons Attribution-NonCommercial-ShareAlike 4.0 International License.









