
INTRODUCTION
Delirium is a common and potentially preventable complication in the postoperative period of cardiovascular surgery (CVS). Postoperative delirium is defined as an acute disorder characterized by changes in attention, cognition and consciousness that occur during the postoperative recovery period. Its occurrence is associated with worse clinical outcomes, as longer length of hospital stay and higher mortality. It is a common but often underestimated clinical challenge in this context. (1) Despite advances in medical and surgical care, the incidence of delirium remains high, (2) which results in adverse clinical consequences for patients and economic consequences for the healthcare system. (3)
Delirium after cardiovascular surgery has been the subject of extensive international research. Multicenter cohorts and observational studies have reported prevalences ranging from 11.3% to 51.6%, depending on the population, type of surgery, and diagnostic method used. (4) According to the initial reports, several factors were identified as contributing to the development of delirium, including advanced age, baseline cognitive impairment, duration of surgery, cardiopulmonary bypass, and complications such as atrial fibrillation (AF) and sepsis. (5-8) These investigations have prompted the development of specific risk scales, such as the PRE-DELIRIC (PREdiction of DELIRium in ICU patients) model, which has been validated in intensive care patients and after CVS, (9) and recommended by international societies, such as the guidelines of the European Society of Anesthesiology, (10) which promote systematic detection and multimodal preventive strategies to mitigate its impact.
Although we have prior registries on CVS in Argentina, this complication has not been thoroughly explored. (11-13)
OBJECTIVE
The aim of this study was to analyze the incidence, risk factors, and outcomes associated with delirium in patients undergoing CVS.
METHODS
We conducted an analysis of the Argentine National Registry of Cardiovascular Surgery (ARGEN-CCV) (14), a cross-sectional, multicenter study spanning 13 months from July 2021 to August 2022. Patients were recruited from 48 public and private centers. The inclusion criteria were patients > 18 years admitted on an elective, urgent, or emergency basis for central CVS. Surgeries for congenital heart defects and peripheral vascular surgery were excluded from the registry. Preoperative, operative, and postoperative data were recorded during the hospitalization period and collected on the REDCap platform. This project was carried out by the Argentine Society of Cardiology, in conjunction with the Argentine College of Cardiovascular Surgeons. The study was registered in ClinicalTrials.gov (NCT0519916).
Diverse studies have examined the predictive variables associated with delirium included in internationally validated risk scores in critical care patients after CVS. (4) These predictors were age, cognitive impairment, the APACHE II (Acute Physiology and Chronic Health Assessment II) score, infection, emergency surgery, type of surgery, preoperative plasma creatinine levels, postoperative urea concentration, use of sedatives or analgesics, history of cerebrovascular disease, EuroSCORE (European System for Cardiac Operating Risk Evaluation), preoperative depression, blood transfusion, metabolic acidosis, alcohol abuse, insomnia, and coma. (9, 15-23)
The ARGEN-CCV database includes the following variables: age, history of cerebrovascular disease, creatinine levels, emergency surgery, type of surgery, alcohol abuse, EuroSCORE, APACHE II score, postoperative urea concentration, transfusions, and postoperative infection.
Ethical considerations
The study was approved by the ethics committee of the Argentine Society of Cardiology.
Statistical analysis
Continuous variables with normal distribution were expressed as mean ± standard deviation, and those with non-Gaussian distribution as median and interquartile range (IQR) 25%-75%. Qualitative variables were expressed as frequencies and percentages. Comparisons between groups were performed using Student's t-test or Wilcoxon test according to the distribution for continuous data, and 2x2 tables were used, as well as the chi-square test with Yates's correction for continuity for categorical variables. Univariate and multivariate analyses were performed to define independent predictors of delirium with the corresponding odds ratio (OR) and 95% confidence interval (95% CI). Different multivariate models were explored to develop a predictive model for postoperative delirium. Those variables with a p-value < 0.10 in the univariate analysis were included so as not to limit the variables potentially useful in the diagnosis. The Hosmer-Lemeshow test was employed to evaluate the adequacy of the model, and a ROC curve was constructed with the variables obtained to assess diagnostic performance, selecting the one with the optimal discrimination. A p value < 0.05 was considered statistically significant. The analysis was performed in R.
RESULTS
Of the 1515 patients evaluated, the incidence of delirium as a postoperative complication was 9.1% (137 patients). Patients who developed delirium were older (67.5 ± 11 versus 63.6 ± 11.3 years; p<0.001).
The clinical history of patients with and without postoperative delirium is summarized in Table 1. The prevalence of hypertension, smoking habits, peripheral vascular disease, chronic obstructive pulmonary disease, alcohol abuse, recent use of illicit drugs, and frailty was higher in patients with delirium.
Table 1
Baseline clinical characteristics (n = 1515)
| Total | Delirium - | Delirium + | P | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Patients | 1515 | 100 | 1368 | 90.9 | 137 | 9.1 | |
| Age, years, mean (SD) | 64 (11) | 63.6 (11.3) | 67.5 (11) | <.001 | |||
| Male | 1122 | 74.1 | 1013 | 74.0 | 109 | 79.6 | 0.007 |
| Hypertension | 1159 | 76.5 | 1043 | 76.2 | 116 | 84.7 | 0.010 |
| Diabetes Mellitus | 436 | 28.8 | 391 | 28.6 | 45 | 32.8 | 0.150 |
| Dyslipidemia | 814 | 53.7 | 737 | 53.9 | 77 | 56.2 | 0.280 |
| Active smoking | 234 | 15.4 | 204 | 14.9 | 30 | 21.9 | 0.001 |
| Reduced LVEF | 243 | 16.0 | 207 | 15.1 | 36 | 26.3 | 0.280 |
| Heart failure | 225 | 14.9 | 202 | 14.8 | 23 | 16.8 | 0.260 |
| AMI ≤30 days | 157 | 10.4 | 137 | 10.0 | 20 | 14.6 | 0.200 |
| AMI >30 days | 190 | 12.5 | 172 | 12.6 | 18 | 13.1 | 0.200 |
| CABG | 69 | 4.6 | 65 | 4.8 | 4 | 2.9 | 0.170 |
| Heart valve surgery | 83 | 5.5 | 72 | 5.3 | 11 | 8.0 | 0.097 |
| PCI | 181 | 12.0 | 161 | 11.8 | 20 | 14.6 | 0.160 |
| Immunosuppression | 18 | 1.2 | 13 | 1.0 | 5 | 3.6 | 0.010 |
| Chronic AF | 109 | 7.2 | 101 | 7.4 | 8 | 5.8 | 0.260 |
| Family history of CAD | 159 | 10.5 | 137 | 10.0 | 22 | 16.1 | 0.010 |
| Peripheral vascular disease | 141 | 9.3 | 120 | 8.8 | 21 | 15.3 | 0.009 |
| Pulmonary hypertension | 96 | 6.3 | 83 | 6.1 | 13 | 9.5 | 0.060 |
| Cerebrovascular disease | 72 | 4.8 | 62 | 4.5 | 10 | 7.3 | 0.080 |
| OSAHS | 56 | 3.7 | 47 | 3.4 | 9 | 6.6 | 0.040 |
| Moderate/severe COPD | 106 | 7.0 | 86 | 6.3 | 20 | 14.6 | <0.001 |
| Recent use of illicit drugs | 12 | 0.8 | 7 | 0.5 | 5 | 3.6 | 0.008 |
| Alcohol abuse | 226 | 14.9 | 195 | 14.3 | 31 | 22.6 | 0.020 |
| Frailty | 90 | 5.9 | 65 | 4.8 | 25 | 18.2 | <0.001 |
| Acetylsalicylic acid | 796 | 52.6 | 717 | 52.4 | 79 | 57.7 | 0.120 |
| P2Y12 inhibitor | 194 | 12.8 | 167 | 12.2 | 26 | 19.0 | 0.020 |
| Statins | 875 | 57.8 | 793 | 58.0 | 82 | 59.9 | 0.330 |
| Beta blockers | 878 | 58.8 | 791 | 57.8 | 87 | 63.5 | 0.090 |
| ACEI | 436 | 28.8 | 397 | 29.0 | 39 | 28.5 | 0.450 |
| ARB | 492 | 32.5 | 441 | 32.2 | 51 | 37.2 | 0.110 |
| Furosemide | 207 | 13.7 | 194 | 14.2 | 13 | 9.5 | 0.060 |
| Thiazides | 97 | 6.4 | 88 | 6.4 | 9 | 6.6 | 0.450 |
| Spironolactone | 108 | 7.1 | 96 | 7.0 | 12 | 8.8 | 0.220 |
| Insulin | 94 | 6.2 | 84 | 6.1 | 10 | 7.3 | 0.280 |
| Oral hypoglycemic agents | 307 | 20.3 | 278 | 20.3 | 29 | 21.2 | 0.400 |
| Oral anticoagulants | 111 | 7.3 | 102 | 7.5 | 9 | 6.6 | 0.360 |
ACEI: angiotensin-converting enzyme inhibitor; AF: atrial fibrillation; AMI: acute myocardial infarction; ARB: angiotensin II receptor blocker; CABG: coronary artery bypass grafting; CAD: coronary artery disease; COPD: chronic obstructive pulmonary disease; LVEF: left ventricular ejection fraction; OSAHS: obstructive sleep apnea-hypopnea syndrome; PCI: percutaneous coronary intervention; P2Y12 inhibitor: P2Y12 receptor platelet inhibitor
The following variables were significantly associated with the development of postoperative delirium: coronary artery disease, combined surgery and median ArgenSCORE values (Table 2). There was no difference in baseline laboratory data. Regarding the intraoperative and postoperative variables, we highlight differences in transfusion requirements, longer cardiopulmonary bypass (CPB) time (105 min. vs. 98 min., p<0.001), prolonged mechanical ventilation (MV), development of low cardiac output syndrome (LCOS), atrial fibrillation (AF), kidney failure, stroke, sepsis, and total length of hospital stay (medians of 9 vs. 6 days, p<0.001). All patients who developed delirium received antipsychotic treatment during hospitalization. Seventy-two percent received monotherapy, while 24% were treated with two antipsychotic agents and 4% with three. The most used drugs were quetiapine (55 patients; 40%), haloperidol (54 patients; 39%), and risperidone (20 patients; 15%). In 53 cases (39%), other therapeutic alternatives were used, primarily benzodiazepines (Table 3).
Table 2
Main preoperative variables
| Total | Delirium - | Delirium + | P | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Patients | 1515 | 100 | 1368 | 90.9 | 137 | 9.1 | |
| HF | 53 | 3.5 | 49 | 3.6 | 4 | 2.9 | 0.600 |
| Endocarditis | 48 | 3.2 | 45 | 3.3 | 3 | 2.2 | 0.600 |
| Acute aortic syndrome | 27 | 1.8 | 22 | 1.6 | 5 | 2.6 | 0.650 |
| Valvular heart disease | 599 | 39.6 | 546 | 39.6 | 53 | 38.7 | 0.680 |
| Coronary artery disease | 933 | 61.6 | 834 | 61.1 | 99 | 72.3 | 0.004 |
| Combined surgery | 247 | 16.3 | 217 | 15.9 | 30 | 21.9 | 0.030 |
| Type of procedure | |||||||
| Elective | 1195 | 78.9 | 1094 | 80.0 | 101 | 73.7 | 0.340 |
| Urgency | 280 | 18.5 | 249 | 18.2 | 31 | 22.6 | 0.400 |
| Emergency | 26 | 1.7 | 23 | 1.7 | 3 | 2.2 | 0.480 |
| Scores | |||||||
| EuroSCORE, median (IQR) | 1.52 (0.93-2.94) | 1.46 (0.88-2.83) | 1.83 (1.25-3.44) | 0.301 | |||
| ArgenSCORE, median (IQR) | 2.33 (1.12-4.78) | 2.23 (1.08-4.74) | 3.34 (1.86-7.31) | 0.004 | |||
HF: heart failure; IQR: interquartile range
Table 3
Main intraoperative and postoperative variables
| Total | Delirium - | Delirium + | P | ||||
|---|---|---|---|---|---|---|---|
| N | % | N | % | N | % | ||
| Patients | 1515 | 100 | 1368 | 90.9 | 137 | 9.1 | |
| Intraoperative | |||||||
| Transfusions | 500 | 33.0 | 439 | 32.1 | 61 | 44.5 | 0.002 |
| CPB | 1126 | 74.3 | 1016 | 74.3 | 110 | 80.3 | 0.059 |
| CPB time (min), median (IQR) | 100 (75-123) | 98 (75-122) | 105 (85-134.3) | 0.007 | |||
| ACC time (min), median (IQR) | 71 (50-94) | 70 (50-93) | 77.5 (60-94) | 0.024 | |||
| Bleeding | 100 | 6.6 | 86 | 6.3 | 4 | 2.9 | 0.047 |
| Cardiac arrest | 38 | 2.5 | 33 | 2.4 | 5 | 3.6 | 0.190 |
| Return to CPB | 28 | 1.8 | 22 | 1.6 | 6 | 4.4 | 0.020 |
| Postoperative | |||||||
| IABP | 24 | 1.6 | 20 | 1.5 | 4 | 2.9 | 0.110 |
| Pulmonary artery catheter | 29 | 1.9 | 24 | 1.8 | 5 | 3.6 | 0.070 |
| Inotropic agents | 30 | 2.0 | 27 | 2.0 | 3 | 2.2 | 0.400 |
| Prolonged MV | 140 | 9.2 | 104 | 7.6 | 36 | 26.3 | <0.001 |
| Days in MV, median (IQR) | 4.5 (2-10) | 4 (2-8.3) | 7 (3-17) | 0.030 | |||
| Bleeding | 159 | 10.5 | 140 | 10.2 | 19 | 13.9 | 0.090 |
| Transfusions | 141 | 9.3 | 126 | 9.2 | 15 | 10.9 | 0.090 |
| Right ventricular failure | 40 | 2.6 | 34 | 2.5 | 6 | 4.4 | 0.100 |
| Low cardiac output syndrome | 235 | 15.5 | 194 | 14.2 | 41 | 29.9 | <0.001 |
| Perioperative AMI | 50 | 3.3 | 45 | 3.3 | 5 | 3.6 | 0.390 |
| Postoperative AF | 361 | 23.8 | 303 | 22.1 | 58 | 42.2 | <0.001 |
| Atrioventricular block | 108 | 7.1 | 95 | 6.9 | 13 | 9.5 | 0.130 |
| Ventricular arrhythmia | 43 | 2.8 | 38 | 2.8 | 5 | 3.6 | 0.260 |
| Temporary PM | 370 | 24.4 | 344 | 25.1 | 26 | 19.0 | 0.053 |
| Permanent PM | 42 | 2.8 | 35 | 2.6 | 7 | 5.1 | 0.056 |
| Kidney failure | 201 | 13.3 | 155 | 11.3 | 46 | 33.6 | <0.001 |
| Hemodialysis | 61 | 4 | 50 | 3.7 | 11 | 8.0 | 0.140 |
| Stroke | 50 | 3.3 | 39 | 2.9 | 11 | 8.0 | 0.002 |
| Fever | 131 | 8.6 | 102 | 7.5 | 29 | 21.2 | <0.001 |
| Sepsis | 89 | 5.9 | 62 | 4.5 | 27 | 19.7 | <0.001 |
| Total length of hospital stay (days) Median (IQR) | 6 (5-9) | 6(5-8) | 9 (6-15.8) | <0.001 | |||
AF: atrial fibrillation; AMI: acute myocardial infarction; CPB: cardiopulmonary bypass; IABP: intra-aortic balloon pump; IQR: interquartile range; MV: mechanical ventilation; PM: pacemaker
Table 4 presents the univariate logistic regression analysis for the prediction of postoperative delirium, with the variables considered, their OR, 95% CI, and p-values. All variables with a p-value < 0.15 were considered in the multivariate analysis for the construction of different predictive models of postoperative delirium. The following model was found to have adequate predictive performance: postoperative AF (OR 2.07; 95% CI 1.29-3.32; p=0.0026), prolonged MV (OR, 2.86; 95% CI, 1.68-4.86; p<0.001), coronary artery disease (OR 1.64; 95% CI 1.02-2.64; p=0.040), and sepsis (OR 3.13; 95% CI 1.65-5.96; p<0.001) (Table 5).
Table 4
Univariate logistic regression model
| Predictors of delirium | OR | 95% CI | p |
|---|---|---|---|
| Hypertension | 1.65 | 0.83-3.25 | 0.150 |
| Frailty | 2.23 | 0.93-5.31 | 0.070 |
| Prior coronary artery disease | 1.45 | 0.84-2.53 | 0.180 |
| Postoperative AF | 1.83 | 1.09-3.09 | 0.020 |
| Prolonged MV | 2.63 | 1.41-4.75 | 0.002 |
| Stroke | 2.14 | 0.89-5.03 | 0.085 |
| Postoperative sepsis | 2.82 | 1.35-5.89 | 0.006 |
| Peripheral vascular disease | 1.67 | 0.83-3.34 | 0.150 |
| Kidney failure | 1.23 | 0.65-2.35 | 0.520 |
AF: atrial fibrillation; CI: confidence interval; MV: mechanical ventilation; OR: odds ratio
Table 5
Multivariate logistic regression model
| Predictors of delirium | OR | 95% CI | p |
|---|---|---|---|
| Prior coronary disease | 1.64 | 1.02 – 2.6 | 0.04 |
| Postoperative sepsis | 3.13 | 1.65 – 5.96 | <0.001 |
| Postoperative AF | 2.07 | 1.29–3.32 | <0.001 |
| Prolonged MV | 2.86 | 1.68–4.86 | <0.001 |
| Frailty | 2.16 | 0.94 – 4.98 | 0.068 |
AF: atrial fibrillation; CI: confidence interval; MV: mechanical ventilation; OR: odds ratio
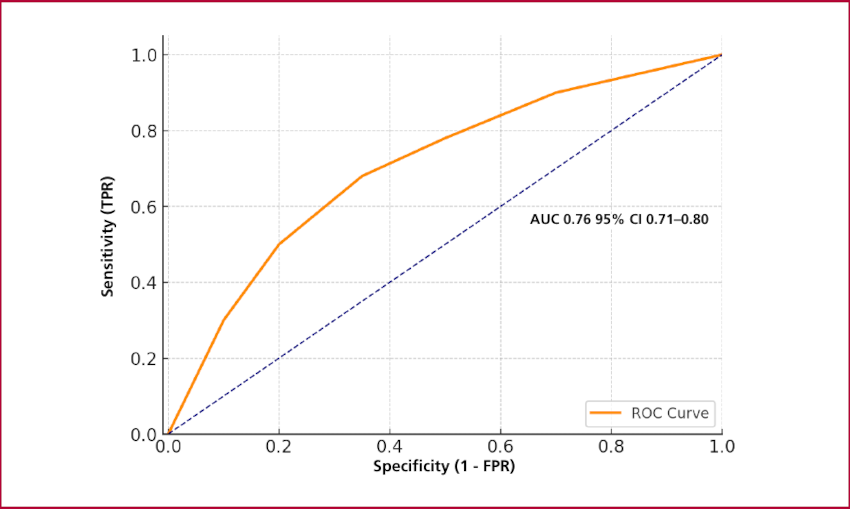
Although preoperative frailty did not reach statistical significance on multivariate analysis (OR, 2.16; 95% CI 0.94-4.98; p=0.068), we decided to incorporate it into the final model due to its theoretical weight and reproducibility as a predictor of delirium in other models.
The area under the curve for this model was 0.76 (95% CI 0.71-0.80) (Figure 1). The p-value for calibration of the model with Hosmer-Lemeshow test was 0.999.
DISCUSSION
This subanalysis of the ARGEN-CCV registry evaluated the incidence and factors associated with postoperative delirium in patients undergoing CVS in Argentina. Given that this common complication has prognostic impact that is often underestimated, this study attempts to provide evidence on the factors associated with its development. The observed incidence of delirium (9.1%) was close to the lower limit of the 10-51% range reported in international studies. (4)
Through multivariate analysis, risk factors that had already been validated in previous studies were identified, such as previous coronary artery disease and postoperative sepsis. Both factors reflect clinical conditions that can influence patients' inflammatory and hemodynamic status. These elements are considered essential in the pathophysiology of delirium and have been described in previous studies, including those conducted by Sugimura et al. (1) and Smulter et al. (3)
However, two traditionally less prominent variables also emerged as significant predictors on univariate analysis: AF and the need for prolonged MV, which were confirmed as independent predictors through multivariate analysis. These findings could theoretically play a relevant role in the onset of delirium due to their level of association, with OR of 2.07 and 2.86 for AF and prolonged MV, respectively. Should this assertion be consistently confirmed, their inclusion in future predictive scores could improve the sensitivity for detecting patients at risk. Brown et al. (6) have reported similar findings when they reported an association between AF and increased risk of postoperative neurological impairment. Nevertheless, we believe it is prudent to interpret these findings with caution. On the one hand, patients with prolonged MV are more prone to develop infections, kidney injury, and to be exposed to drugs such as opioids and benzodiazepines, and all these situations are associated with the risk of delirium. The association between postoperative AF and delirium through intensified inflammatory mechanisms in the context of surgical trauma is plausible, reinforcing the need to evaluate these factors together rather than in isolation. (24)
A notable finding is the role of preoperative frailty, which has been strongly linked to adverse events in multiple settings. While the present analysis did not demonstrate a significant association between frailty and postoperative delirium, its systematic evaluation in the context of CVS should be considered, not only due to its growing interest and theoretical basis, but also because it is part of comprehensive patient care, as proposed by Inouye et al., (25) who suggested including frailty as a key element in preventive strategies for delirium.
It is important to note that, although kidney failure did not reach statistical significance on the multivariate model, it has been consistently described as a predictor of delirium in multiple previous studies and should be assessed. (15,18)
In our cohort, all patients who developed delirium received treatment with antipsychotics, predominantly as monotherapy, though a considerable proportion required the administration of two drugs or greater. This finding reflects both the clinical burden of delirium and the complexity of its pharmacological management in the postoperative context of CVS. Although antipsychotics are commonly used to manage symptoms such as agitation or hallucinations, the evidence of their efficacy in delirium is inconclusive. Thus, their use must be balanced against the risk of adverse effects, especially in elderly patients or those with cardiovascular comorbidities. (26) The high frequency of haloperidol and quetiapine use in this series is consistent with standard practices reported in other critical care settings. However, it is necessary to move toward more standardized management strategies focused on non-pharmacological interventions whenever possible. (27)
We did not specifically evaluate the impact of monotherapy vs. the use of more than one drug on delirium duration or length of hospital stay. We consider that this analysis could provide valuable information for future research, given that the profile and combination of drugs could influence clinical evolution and functional recovery.
From a statistical point of view, the model constructed demonstrated good discrimination, with an area under the curve (AUC) of 0.76 (95% CI:0.71-0.80) and adequate calibration as assessed by the Hosmer-Lemeshow test (p = 0.999). These parameters indicate that the model not only discriminates well between patients with and without risk but also predicts events with acceptable accuracy across the entire population analyzed.
Regarding clinical implications, our findings underscore the need for implementing systematic measures to early detect delirium at the local level, as well as multimodal management protocols that integrate AF monitoring, ventilation, and sepsis diagnosis. Furthermore, incorporating variables such as frailty and intercurrent events into future predictive models should be contemplated, as it has the potential to result in more comprehensive and dynamic tools for risk stratification.
Future lines of research should consider prospective models using validated scales, as the CAM-ICU, and explore the impact of preventive interventions in high-risk groups. Furthermore, it would be beneficial to examine the incremental value of incorporating biomarkers of inflammation, as IL-6 (interleukin-6), CRP (C-reactive protein), and NLR (neutrophil-to-lymphocyte ratio) or nervous system function in predictive models of delirium in CVS. (28)
Study limitations
Firstly, it should be noted that the observational and cross-sectional design of the study prevents us from establishing definitive causal relationships between the analyzed factors and the occurrence of delirium.
Secondly, the diagnosis of delirium was based on the clinical assessment of the treating team, without the systematic use of validated scales such as the CAM-ICU. Therefore, the introduction of classification biases may be possible, and thus explain why the incidence of delirium is lower in this study than that observed in the literature. In addition, the database did not include certain relevant predictors, such as prior cognitive impairment or detailed use of sedatives, which could have introduced confounding variables that were not addressed in the analysis. Finally, although the study included multiple centers nationwide, no adjustments were made for center, and the impact of institutional variability on the detection or treatment of delirium was not explored.
CONCLUSION
Postoperative delirium was found to be a common and relevant complication in patients enrolled in the ARGEN-CCV registry. The proposed model of coronary artery disease, sepsis, AF, MV, and frailty as predictors of postoperative delirium showed adequate diagnostic performance. While not significant, frailty warrants particular consideration due to its potential clinical implications. These findings could guide early detection and preventive intervention strategies in high-risk surgical populations.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).