
INTRODUCTION
In people over 80 years of age, multiple factors limit the application of the different cardiovascular practice guidelines. This population faces higher mortality, a frequently compromised quality of life and, in addition, is underrepresented in the different clinical trials, generating gaps in the evidence.
The main challenges include the discrepancy between chronological and biological age, multimorbidity, atypical presentation of cardiovascular diseases often influenced by geriatric syndromes, and variable therapeutic response.
Another characteristic in this population group is the heterogeneity within the functional continuum, which includes robustness, frailty, disability, and terminality. In a context of growing life expectancy and increasing prevalence of cardiovascular diseases, it is a priority to identify these gaps in order to improve outpatient clinical management and outcomes. (1,2,3,4,5,6)
Roundtables are an effective tool for discussing controversial scenarios and promoting consensuses applicable to clinical practice.
OBJECTIVES
To address this problem, the Cardiogeriatrics Council of the Argentine Society of Cardiology proposed and organized the first national roundtable that brought together referring physicians. The following scenarios were selected for this first meeting: frailty, polypharmacy, cardiovascular prevention, heart failure, atrial fibrillation and acute coronary syndromes. The objectives of the meeting were to discuss gaps in management and establish recommendations for this population, to promote a critical analysis of existing guidelines, and to explore strategies adapted to local needs. In the present publication we present the results obtained in the first four scenarios.
METHODS
The roundtable was held in person in June 2024 in the city of Buenos Aires, Argentina, and was attended by 40 referring physicians, 34 cardiologists and 6 geriatricians, with recognized clinical and academic careers.
The methodological process was structured in three stages to systematically address the knowledge gaps.
-Gap identification: In this initial phase, the organizing team of the Cardiogeriatrics Board of Directors conducted an exhaustive review of recent literature and clinical practice guidelines. This analysis allowed the identification of areas with insufficient evidence in the management of cardiovascular diseases in older adults and to draw up a preliminary list of gaps in knowledge.
-Scenario design: In this stage, the usefulness of various frailty tools and diagnostic and therapeutic strategies in patients over 80 years of age were discussed and analyzed. In scenarios with comorbidities, the condition was postulated to be stable, without terminal pathology. It was decided to divide this population into robust, mild frailty and moderate frailty, because they are different conditions in terms of prognosis and treatment. Based on the proposed clinical scenarios, the different rounds were designed. Selected literature was sent to the participating physicians and voting forms were designed for records that would be used during the discussion.
-Table of discussion and consensus : Finally, the meeting was conducted through a structured methodology that combined open discussion and then anonymous voting.
All these stages sought to ensure a comprehensive and systematic approach, aimed at generating practical recommendations to optimize cardiovascular management in elderly people.
In each case, the degree of recommendation is presented on a scale ranging from recommended to not recommended (Figure 1).

Discussion scenarios:
Round 1: Frailty
The bidirectionality between frailty and cardiovascular disease is influenced by pathophysiological mechanisms and common risk factors. In turn, treatment of cardiovascular disease impacts on frailty and vice versa. (7,8,9,10)
Frailty has been incorporated into cardiology guidelines as a variable that conditions the evolution and treatment in different scenarios, including prevention. The guidelines include it from a multidomain approach with a person-centered perspective and adapted to different clinical scenarios, although despite this, both in practice and in studies, the use of the functional frailty model continues to be prioritized. Lack of a universal definition, multiple assessment tools, the proposal of a functional phenotype and another based on the accumulation of deficits, has conditioned its use to date in clinical practice. (11)
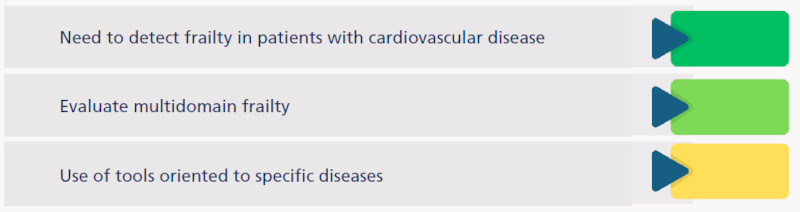
Results: The relevance of detecting frailty in patients with cardiovascular disease was discussed, and 100% of participants agreed on its importance. Functional assessment was considered more relevant by 32.5% of participants and 50% reported using some screening method to assess frailty. More than half (55%) considered the use of frailty tools oriented to specific diseases to be more appropriate, 22.5% did not consider this option and 22.5% were in doubt. If a multi-domain assessment tool had to be chosen, 35% would opt for the Clinical Frailty Scale (CFS), (12) 20% for the Comprehensive Geriatric Assessment-Frailty Index (CGA IF), (13) 15% for the Edmonton Frailty Scale, (14) 12.5% for the Frail-VIG index (15) and 17.5% would prefer a simple screening of each domain (Annex 1).
Opinion: Although all the participants considered the importance of detecting frailty in cardiology, only 50% used some type of frailty screening (it should be noted that 6 of the participants were geriatricians). It is relevant to note that only 32.5% believe it is more important to evaluate frailty from a functional approach.
The Cardiogeriatrics Council promotes multidomain assessment, which includes the functional component, with a person-centered approach. Although no agreement was reached at the meeting on which tool to use, we understand frailty as a global condition of the patient and prefer comprehensive assessment tools rather than those specific to each pathology. Not having reached agreement on this point opens the way for future research (Figure 2).
Round 2: Polypharmacy
Multimorbidity and polypharmacy are highly prevalent in this population group. (16)
Their association with frailty exponentially increases the likelihood of major adverse cardiovascular events and poor adherence to treatment. (17,18) The criteria for appropriate prescribing and potentially inappropriate drugs described for the elderly are not frequently used in cardiology practice.
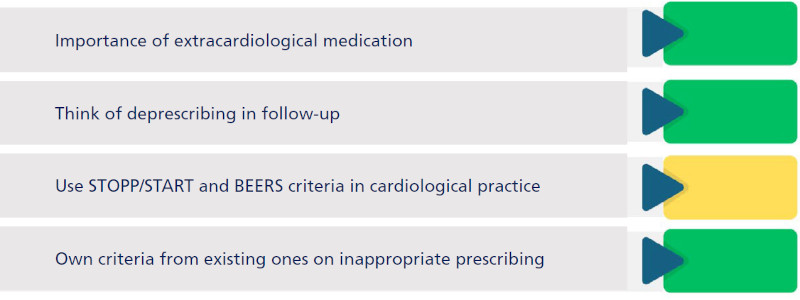
Results: The evaluation of extracardiac medication was relevant for all participating physicians and 97.5% think of deprescribing drugs during follow-up.
In 75% of cases, participants would use STOPP/START (19,20) and BEERS (21) criteria and 87.5% found it interesting to generate our own criteria on inappropriate prescription (Annex 1).
Opinion: From the Council, we emphasize the importance of evaluating the patient's total medication, assessing appropriate prescription, encouraging deprescribing of potentially inappropriate drugs, and the search for criteria that facilitate their application in daily practice at the local level. This motivated us to work on a project on appropriate medication in cardiovascular therapeutics (MATE, in progress). (Figure 3).
Round 3: Primary cardiovascular prevention
The 2023 SAC guideline on cardiovascular prevention questions the use of cardiovascular risk (CVR) scores as they are not validated in the Argentine population. (22) However, the use of scores in primary prevention in validated populations is useful and necessary and is a IC recommendation in the guidelines. Within the IC recommendations, frailty and other morbidities are included as risk modulators. (23) A 10-year CV risk estimation using the SCORE2-OP for patients over 70 years of age, strongly recommends the evaluation of the treatment risk/benefit, the presence of frailty and other risk modifiers, polypharmacy and patient preferences.(24) The use of validated scores in this patient population has an impact on therapeutic decisions.
The European guidelines recommend the use of statins in patients over 70 years of age at high or very high risk (IIb recommendation) based mainly on the analysis of age subgroups of the JUPITER and HOPE-3 studies. (25) On the other hand, the American guidelines recommend their use in patients over 75 years of age at high risk (IIb recommendation), incorporating the use of calcium scoring by means of coronary angiography as a risk modifier. (26)
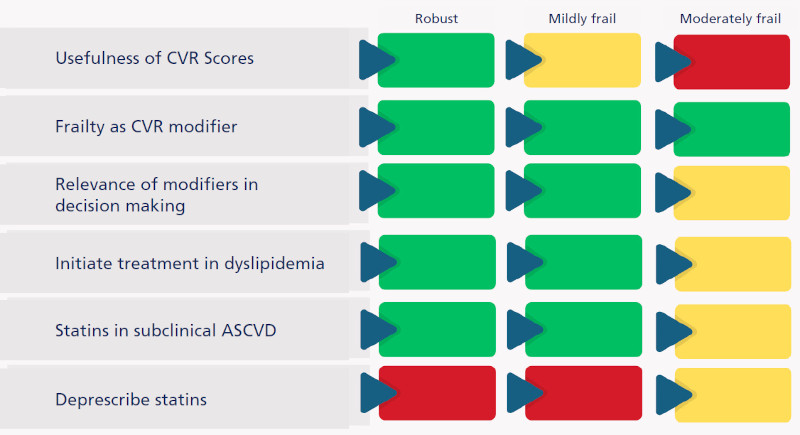
Results: The usefulness of CVR scores was considered to be inversely proportional to the degree of frailty: 66.7% in robust patients, 46.2% in mild frailty and 25.6% in moderate frailty.
A hundred percent of participating physicians considered frailty as a CVR modifier. The relevance of these modifiers in clinical decision making reached 84.6% in both robust and mild frailty patients, dropping to 64.1% in moderate frailty (with 33.3% doubt/indecision in this scenario).
Regarding the initiation of lipid-lowering treatment, acceptance showed a descending gradient according to frailty: 82.1% in robust patients, 69.2% in mild frailty and 23.1% in moderate frailty, with significant uncertainty (51.3%) in the latter group.
Screening for subclinical atherosclerosis was accepted by 64.1% of participants in robust patients, 56.4% in mild frailty (30.8% of doubt) and 20.5% in moderate frailty (43.6% of doubt).
In the case of statin prescription in primary prevention with documented subclinical atherosclerosis, acceptance was 76.9% in robust patients (12.8% of doubt), 64.1% in mild frailty (15.4% of doubt) and 38.5% in moderate frailty (28.2% of doubt).
Statin deprescribing with documented subclinical atherosclerosis was considered in 23.1% of robust patients, 20.5% with mild frailty and 41% with moderate frailty. (Annex 1).
Opinion: As we can see, the lack of evidence in older patients limits decisions, whether from risk stratification with scores or their use in primary prevention.
Although the guidelines postulate frailty as a modifier of CVR, and taking into account that frailty increases the risk of major events, the indication for statins decreased as the degree of frailty increased, even in the presence of subclinical atheromatosis. (27,28) The board recommends the use of statins in these groups of patients while the evidence progresses (Figure 4).
Round 4: Heart failure
Heart failure (HF) represents a major epidemiological challenge with a high number of hospitalizations, deterioration in quality of life and high morbidity and mortality. Multimorbidity, polypharmacy and frailty are highly prevalent in both aging and HF, to which we must add the heterogeneity of this population and their longer life expectancy, turning decision-making difficult.
Frailty may affect up to 45% of HF patients and, in turn, increases the risk of HF. (29)
Symptoms are often assumed to be part of aging, which generates difficulty and delay in their diagnosis. Moreover, in this group of patients the cut-off values of natriuretic peptides for diagnosis are higher and are strongly influenced by renal function and other comorbidities, which often reduces their degree of certainty. (30)
Heart failure with preserved left ventricular ejection fraction (HF-pEF) is a complex clinical syndrome affected by comorbidities, and it is also multicausal, since it can be a manifestation of cardiovascular dysfunction or a combination with other morbidities. At the time of the Round Table discussion, the specific therapy was reduced to gliflozins. (31) The publication of the FINEARTS-HF study with finerenone was later. (32)
In HF with reduced left ventricular ejection fraction (HF-rEF), quadruple therapy is the cornerstone of treatment with class IA indication (33,34,35).
a. HF-pEF
Results: The indication of gliflozins in patients without volume overload was accepted by 94.6% of participants in robust patients, 86.5% in mildly frail patients and 54.1% in moderately frail patients (40.5% of doubt). In the scenario of creatinine clearance between 20 and 30 ml/min, 78.4% would indicate them in robust patients (16.2% of doubt), 45.9% in mildly frail patients (43.2% of doubt) and 24.3% in moderately frail patients (51.4% of doubt).
In patients with atrial fibrillation (AF) and obesity, the use of glucagon-like peptide 1 receptor agonists (GLP-1 RA) had an acceptance rate of 40.5% in robust, 16.2% in mildly frail and 5.4% in moderately frail patients. Uncertainty was 29.7%, 45.9% and 32%, respectively.
The usefulness of the N-terminal pro B-type natriuretic peptide (NT-proBNP) as a diagnostic tool was accepted by 59.5% of participants for robust, 48.6% for mildly frail and 40.5% for moderately frail patients, with 21.6% were in doubt about its usefulness in robust, and 29.7% in mild and moderate frailty (Annex 1).
b. HF-rEF
Results: Simultaneous initiation of the four therapeutic pillars in the absence of clinical signs of HF showed an acceptance rate of 45.9% in robust, 27% in mildly frail, and 2.7% in moderately frail patients (24.3%, 29.7%, and 35.1%, respectively). In the pharmacological prioritization, in the 3 scenarios, gliflozins emerged as the first option, followed by sacubitril valsartan and mineralocorticoid receptor antagonists.
In the presence of a clearance <30 ml/min, in all three scenarios, gliflozins were the drugs of choice with 81.1% acceptance for robust and mildly frail patients and 70.3% acceptance in cases of moderate frailty.
In patients with recovered left ventricular ejection fraction, 91.9% of participating physicians would maintain treatment in robust, 73% in mildly frail and 59.5% in moderately frail patients, with a doubt rate of 8.1%, 24.3% and 21.6% for the respective scenarios.
The implementation of palliative care from the diagnosis of HF was supported by 32.4% for robust patients, 43.2% for mild frailty (with an equal percentage of doubt) and 89.2% for moderate frailty. The use of tools such as the NECPAL (36) appeared to be useful in 43.2% for robust, 51.4% for mildly frail and 69.4% for moderately frail patients.
Prioritizing intensive care management in the emergency room over hospitalization had an acceptance rate of around 60% in both robust and moderately frail patients (Annex 1).
Opinion: In HF-pEF, the use of NT-proBNP as a tool was not considered of great relevance, losing even more value as the degree of frailty increases. We consider that in the case of HF presentation and multimorbidity in this group, the diagnosis remains a major challenge. Regarding the prescription of specific treatment with gliflozins, it had high acceptance for robust and mildly frail patients and decreased by half in moderate frailty, with a high percentage of doubts, and the indication was somewhat lower in renal patients as frailty increases.
Treatment of multimorbidity in HF-pEF is a priority, together with potential decompensating causes. Following appropriate prescribing criteria, we recommend considering the use of gliflozins.
Concerning HFrEF, the upper range for inclusion in clinical trials has typically been 75 ± 5 years; for this reason, we have very few data on randomly assigned interventions in patients over 80 years of age. This could be one of the reasons why simultaneous treatment with quadruple therapy has been considered by less than half in robust patients, decreasing significantly to almost zero in moderate frailty, with a relevant percentage of doubt as frailty increases. In both HF-pEF and HF-rEF it has a generally consistent efficacy in older individuals, where target doses could be attempted with slow titration and close monitoring, considering that the greater the frailty, the greater the risk of HF and its complications and vice versa. There is also no evidence to suggest that therapies should be discontinued or doses modified in the context of frailty (Figures 5 and 6).
Fig. 5
Heart failure with preserved left ventricular ejection fraction (HF-pEF).
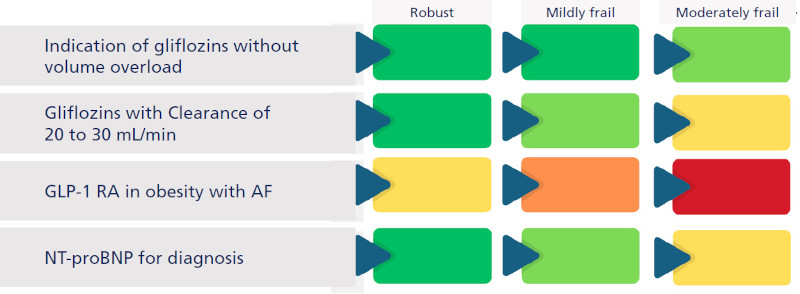
AF, atrial fibrillation; GLP-1, glucagon-like peptide-1 receptor agonists; NT-proBNP: N-terminal pro-B-type natriuretic peptide
Fig. 6
Heart failure with reduced left ventricular ejection fraction (HF-rEF).
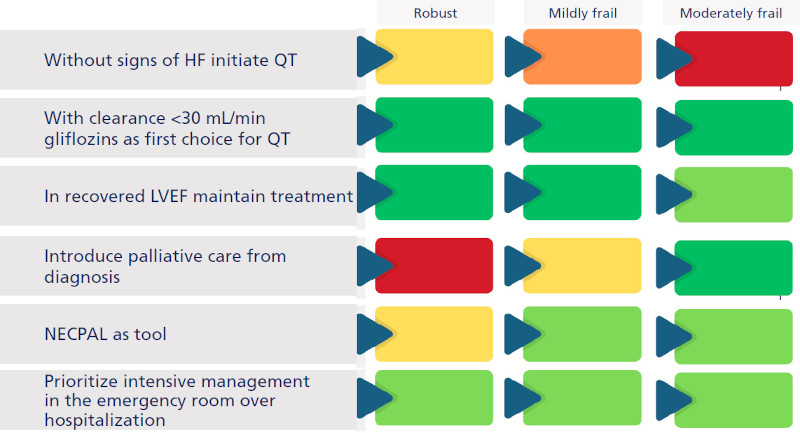
HF: heart failure; LVEF: left ventricular ejection fraction; NECPAL: need for palliative care; QT: quadruple therapy.
This shows how the degree of frailty conditions therapeutic decisions. As frailty increases, the indication for treatment decreases, with greater uncertainty about the balance between risks and benefits.
The observed results underscore the need to create clear guidelines, design specific strategies, identify and individualize clinical and hemodynamic profiles, in order to provide adequate guidance for this population group.
Limitations
The main limitations derive from the methodology used, based on expert consensus, which implies that the recommendations reflect the experience and clinical judgment of the participants. Although the group consisted of experts in cardiology and geriatrics, most of them are not exclusively dedicated to cardiogeriatrics. Therefore, it is necessary to validate these recommendations in future studies to confirm and adjust these findings in clinical practice. The approach of multiple scenarios also limited the discussion time.
CONCLUSIONS
The number of elderly patients has increased significantly, reaching 20% of the total population, and demographic trends show that this population will increase even more in the coming decades. The evidence and guideline recommendations for the management of older patients are often not as robust and rigorous as for younger patients (atypical presentations, presence of frailty, evidence gaps, etc.).
Aging is a complex and heterogeneous biological process, where we can observe that chronological age alone is not sufficient to define conducts. The results show how frailty significantly conditions therapeutic decisions in most scenarios, with a tendency towards more conservative approaches as the degree of frailty increases.
Frailty, unlike age, is a multidimensional and potentially reversible concept that is associated with poor clinical outcomes. To this end, it is crucial to approach frail patients with the necessary caution, but avoiding excessive care that may lead to unfairly denying them potentially beneficial treatments as in robust elderly patients.
Our goal is to incorporate frailty into the decision-making analysis and as part of the treatment strategy.
This meeting highlighted the need for a multicenter registry to know our population and to work on the development of a multidomain frailty score that combines the best tools. For this reason, the registry of frailty, multimorbidity and polypharmacy (RAFA) is under development.
It was also proposed to develop our own criteria, based on existing criteria such as STOPP/START and BEERS, to address appropriate and inappropriate prescribing in patients with cardiovascular diseases. The Council is currently working on this registry proposal (MATE: Medication Appropriateness in Cardiovascular Therapeutics).
While progress is being made in more studies, consensuses from referent scientific societies can provide guidance in current practice. For this reason, we are planning the second Roundtable based on heart failure, with the aim of generating recommendations with expert opinion in this scenario.
Conflicts of interest
None declared
(See authors' conflicts of interest forms on the Web).
Roundtable participants in alphabetical order:
Achilli Federico (Sanatorio Privado de Río Cuarto), Ahuad Guerrero Andrés, (Corporación Médica San Martín) Barbagelata Leandro (Hospital Italiano Buenos Aires), Barrero Carlos (Clínica Bazterrica, Santa Isabel and former president of SAC), Belziti César (Hospital Italiano Buenos Aires, former president of SAC), Blanco Patricia (Hospital Naval Buenos Aires and Scientific Secretary of the Cardiogeriatrics Council), Brenzoni Noelia (Hospital Austral), Duronto Enrique (Fundación Favaloro), Fernández Alberto (Sanatorio Modelo de Quilmes), Flor Laura (Instituto Cardiovascular del Buen Pastor), Forcada Pedro (Cardioarenales. Hospital Austral), Grancelli Hugo (Sanatorio Trinidad Palermo and former president SAC), Guardiani Fernando (Clínica Olivos), Guetta Javier (CEMIC), Hershson Alejandro (Fundación Favaloro EX president SAC), Hidalgo Anfossi Jaime (President of SGGCH Chile), Higa Claudio (Hospital Alemán), Iglesias Ricardo (former president SAC), Jara Rafael (Former president SGGCH, Chile), Jauregui José Ricardo (President of the International Association of Gerontology and Geriatrics (IAGG), López Adriana (Universidad de Santiago de Chile); Manzotti Matías (Hospital Alemán and President of SAGG), Nani Sebastián (Clínica Sagrada Familia), Nauhm Yalile (Clínica Alemana, Chile), Palacio María Soledad (Director of the Cardiogeriatrics Council), Pomes Iparraguirre Horacio (Director of the Health Policies Area SAC), Pulido Juan (Hospital Gandulfo), Salvati Ana (Hospital de Clínicas and president of Fundación Cardiológica Argentina, former president SAC), Salzberg Simón (Hospital Fernández), Schygiel Pablo (Clínica Bessone), Sokn Fernando (Instituto Médico Adrogué), Spennato Mario (Director of the Area of Advice and Standards SAC), Suarez Guillermo (Technical Secretary of the Cardiogeriatrics Council SAC), Swieszkowski Sandra (Hospital de Clínicas, Sanatorio Otamendi), Thierer Jorge (CEMIC and Director of the Revista Argentina de Cardiología), Trivi Marcelo (ICBA), Trongé Jorge (Advisory Member of the Cardiogeriatrics Council and former SAC President), Trossero Romina (ICBA), Villalba Núñez Mayra (CEMAR 1), Villarreal Ricardo (Sanatorio Güemes).