
Ergospirometry or cardiopulmonary exercise test (CPET) in patients with pulmonary artery hypertension (PAH) and non-surgical chronic thromboembolic pulmonary hypertension (CTEPH) allows obtaining predictor variables, such as peak oxygen uptake (peak VO2) and ventilation (VE)/carbon dioxide production (VCO2) ratio, and is suggested by the Guidelines on Pulmonary Hypertension for risk stratification, as is the tricuspid annulus plane systolic excursion distance (TAPSE)/systolic pulmonary artery pressure (sPAP) ratio measured by transthoracic echocardiography (TTE). (1) The predictive association between the TAPSE/sPAP ratio and the above mentioned CPET variables is not defined in this population.
The primary objective of this study was to evaluate echocardiographic parameters of right ventricular (RV) function as predictors of exercise capacity in patients with PAH and non-surgical CTEPH. Secondary objectives were to determine the association between VE/VCO2 and echocardiographic variables such as TAPSE, sPAP, right ventricle (RV) fractional area change (FAC) and right atrial area.
It was an observational, cross-sectional, pathophysiological and prospective study.
We recruited 7 patients aged between 18 and 65 years, of whom 5 were diagnosed with idiopathic PAH, 1 with PH associated with connective tissue disease, and 1 with non-surgical CTEPH. All were followed up as part of the Pulmonary Hypertension Program at Hospital Ramos Mejía. The diagnosis of PH was confirmed by right heart catheterization according to the 2022 European Society of Cardiology (ESC) and European Respiratory Society (ERS) Guidelines on Pulmonary Hypertension. (1)
Patients were required to be on stable drug therapy for at least the last 4 weeks prior to study entry.
This was defined as no new PH-specific therapy or no change in the dose of the current specific therapy.
The CPETs and TTEs were performed no more than 15 days apart and by the same operator in each study. Patients were at low risk according to REVEAL 2.0. The CPETs were performed with portable equipment, on a treadmill, using a COSMED model K5 gas analyzer and a modified Bruce protocol with procedures in accordance with the current guideline recommendations. (1) The following variables were considered: peak VO2, VCO2, minute ventilation (VE) and heart rate. The echocardiograms were performed using a General Electric VV7 equipment. All measurements of cardiac structure and function were performed according to the current guidelines. (2)
Statistical analysis was performed using Student's test and Wilcoxon rank-sum test for paired data and a p-value < 0.05 was considered significant.
Five of the seven patients were female. The median age (interquartile range, IQR) was 48 (29-53) years. Two patients received treprostinil, macitentan and sildenafil, two received sildenafil, ambrisentan and selexipag, two received tadalafil and ambrisentan and one received sildenafil and ambrisentan. Table 1 shows the hemodynamic values of the population.
Table 1
General characteristics
| Characteristic | Median (IQR) |
|---|---|
| mPAP (mmHg) | 59 (34-70) |
| CO (L/min) | 4.75 (4.3-5) |
| CI (L/min/m2) | 2.83 (2.6-2,9) |
| ISV (mL/m2) | 34.5 (27.5-41) |
| PA SaO2 (%) | 68 (63-73) |
| PVR (WU) | 11 (7.8-12,3) |
| peak VO2 (mL/kg/min) | 17.1 (15.7-21) |
| peak VE/VCO2 | 34.1 (28.4-43.2) |
| Right atrium (cm2) | 20 (18-23) |
| TAPSE (mm) | 18 (17-19) |
| sPAP (mmHg) | 40 (35-69) |
| TAPSE/sPAP | 0.45 (0.26-0.49) |
| FAC (%) | 35 (24-48) |
CI, cardiac index; CO: cardiac output; IQR, interquartile range; FAC: right ventricular fractional area change; ISV: indexed left ventricular systolic volume; mPAP: mean pulmonary artery pressure; MV: minute volume; PA SaO2: pulmonary artery O2 saturation; PVR: pulmonary vascular resistance; sPAP: systolic pulmonary artery pressure; TAPSE, tricuspid annulus plane systolic excursion; VE/VCO2: minute ventilation/CO2 production ratio at peak exercise; WU: Wood unit; peak VO2: peak oxygen uptake;
Among different echocardiographic variables, a statistically significant association was found in linear regression between the TAPSE/sPAP variable and peak VO2 with a β coefficient = 27.5 (p=0.003) (Figure 1). No significant association was found among other CPET parameters with predictive value in PAH, such as the VE/VCO2 ratio, and other echocardiographic variables.
Fig. 1
Association between peak VO2 and TAPSE/sPAP ratio.
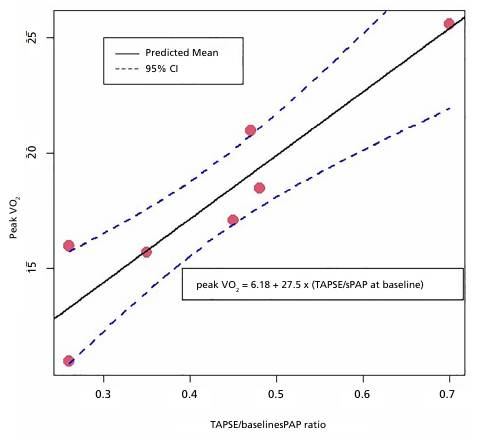
95% CI: 95% confidence interval; sPAP: systolic pulmonary artery pressure; TAPSE: tricuspid annular plane systolic excursion; peak VO2: peak oxygen consumption.
Remodeling of the arterioles, inherent to precapillary pulmonary hypertension, causes a progressive increase in physiological dead space, that is, an increase in the number of alveoli that are healthy and wellventilated but poorly perfused at rest. As the disease progresses and remodeling continues, the number of perfused alveoli decreases, as does their recruitment during exercise. This ventilation/perfusion mismatch causes progressive ventilatory inefficiency that is responsible for the exertional dyspnea in these patients: they need to increase ventilation to take in O2 and eliminate CO2. The pathophysiology of patients with PAH that becomes evident during CPET has been described in numerous studies. (3)
As pulmonary vascular disease progresses, adaptive and maladaptive right ventricle remodeling occurs, conditioning the right ventricular-pulmonary artery coupling (RV-PA). (4,5)
The TAPSE/sPAP ratio is a noninvasive measurement that correlates with invasive measurement of RV-PA coupling. This association has prognostic implications in patients with precapillary PH. Ghio et al. examined the RV-PA coupling, assessed as TAPSE/ sPAP, during a dobutamine stress test in patients with precapillary PH. (6) Considering the inclusion of the TAPSE/sPAP parameter in the Guidelines on Pulmonary Hypertension and the demonstration of its predictor value in patients with PH as well as the already established usefulness of the CPET for risk stratification, diagnosis and follow-up of these patients, the main finding of our study is the solid association between baseline TAPSE/sPAP variable with peak VO2 in only 7 patients.
At the time of writing, no further evidence on the association between TAPSE/sPAP variable and peak VO2 has been found. The predictive information of an easily obtained parameter such as the TAPSE/ sPAP ratio is very useful in view of the accessibility and lower cost of echocardiography compared to ergospirometry, especially in contexts such as the treatment of this hemodynamic condition in low and middle-income regions. In our opinion, this result allows the development of a hypothesis that will encourage the performance of a study involving a larger number of patients.
Ethical Considerations
Not applicable
Conflicts of interest
None declared. (See conflicts of interest forms on the website).