
INTRODUCTION
Cardiovascular disease is the leading cause of death in both men and women. (1) It has been shown that in myocardial infarction, female gender, usually underrepresented in published works, (2,3) is associated with longer delays in consultation, lower rates of primary angioplasty, higher probability of developing heart failure and cardiogenic shock (CS), (4,5,6) and higher mortality. (7,8,9,10). In CS, a condition with mortality ranging between 40-60%, (11) differences in presentation, treatment received and evolution between men and women are not clearly defined. This "indefinition" is particularly relevant today, since there is evidence that biological gender (considering the different hormonal influence) implies some differences in physiological responses and in the action of certain drugs (12) that influence clinical disorders [as in sepsis (13, 14)], and should therefore be taken into special account. (1) Similarly, equity in access to health care is a current objective of many scientific societies. (15) To determine whether there is equity or differences in relation to gender, the contribution of regional multicenter registries, in our case the LATIN Shock registry, (16) is essential, since it has also been shown that there are differences in access to health care depending on whether high or low-income countries are evaluated. (17,18)
To date, there is scarce literature worldwide on the implications of gender differences in the characteristics, evolution and treatment of CS, and none in Latin America.
OBJECTIVES
1) To analyze whether there are differences in the clinical presentation, treatment received, and clinical evolution according to gender in patients with CS in the context of acute coronary syndromes (ACS), and 2) To establish whether gender is an independent predictor of in-hospital mortality.
METHODS
LATIN Shock is a multicenter, observational, prospective and consecutive registry of ACS complicated with CS. The Research Area of the Argentine Society of Cardiology provided computer and statistical support for the study.
Cardiogenic shock was defined as the presence of systolic blood pressure (SBP) <90 mmHg for at least 30 minutes or requirement of vasopressors and/or inotropic drugs to maintain SBP ≥90mmHg, associated with signs of hypoperfusion and signs of pulmonary congestion.
The inclusion criteria were: patients over 18 years of age, hospitalized in a coronary care unit or multipurpose critical care unit for ST-segment elevation ACS (STE-ACS) or non-ST-segment elevation ACS (NSTE-ACS), who presented CS since admission or developed it during hospitalization.
Data were collected by the responsible investigators of the different centers in an electronic file designed ad hoc with the RedCAP platform. In-hospital events were analyzed.
Further details on the characteristics of the participating centers can be found in LATIN Shock. (16)
Ethical considerations
The study was conducted in accordance with current national and international regulations: Declaration of Helsinki of the World Medical Association, the ICH E6 Good Clinical Practice Guidelines, Resolution 1480/11 of the National Ministry of Health and GCBA Law 3301/09. The protocol was approved by the Bioethics Committee of the Argentine Society of Cardiology (SAC). Informed consent was waived since no sensitive data were recorded and only in-hospital follow-up was performed.
Statistical analysis
The information obtained through RedCAP was exported in Excel and the database was analyzed using Epi-info 7. Continuous variables were expressed as mean and standard deviation for those with normal distribution and as median with interquartile range 25% -75% (IQR) for those non normal distribution. The statistical analysis of continuous variables was performed using Student's t test or the Wilcoxon rank sum test, as appropriate. Discrete variables were expressed as percentages and comparisons were performed using the chi-square test with Yates correction or Fisher's exact test, as appropriate.
Contingency tables were built to analyze variable association or independence. Linear and/or multiple logistic regression analyses were carried out to determine the existence of associations and/or independent predictions between the different variables involved and mortality. All statistical comparisons were two-tailed and values of p<0.05 were considered statistically significant.
RESULTS
Forty-one Latin American centers from seven counties (Argentina, Bolivia, Chile, Ecuador, Honduras, Paraguay and Perú) participated in the registry, recruiting 278 patients from October 2021 to September 2023. Seventy percent of patients were men (n=195) and overall median age was 66 years (IQR 59-75). Women were older [median age 71 years (IQR 61-78) vs. 64 years (IQR 58-73) in men, p<0.001]. Most CS (75%) were due to STE-ACS. Details of the causes of CS are shown in Figure 1.
Fig. 1:
Causes of CS
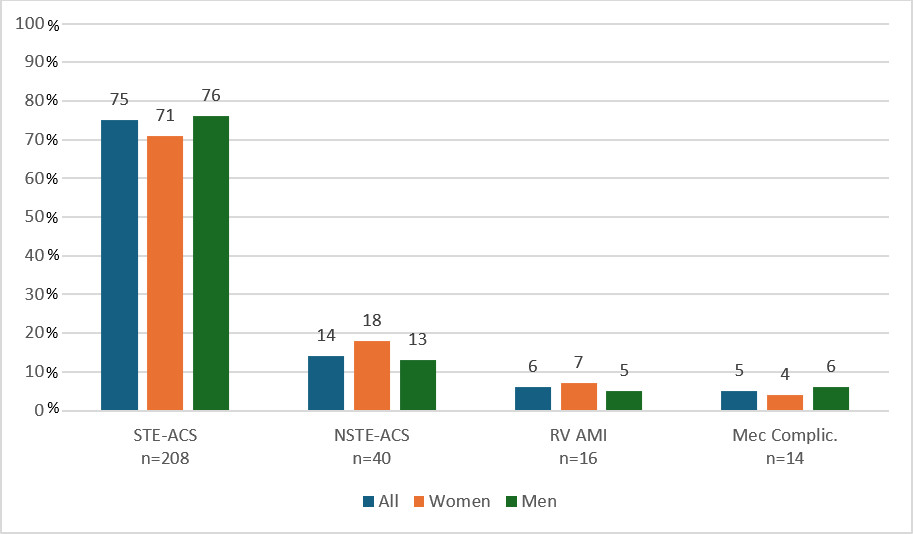
CS: Cardiogenic shock; Mec Complic: mechanical complications; NSTE-ACS: non-ST-segment elevation acute coronary syndrome; RV AMI: right ventricular acute myocardial infarction; STE-ACS: ST-segment elevation acute coronary syndrome
CS was present from admission in 60% of cases (66% in women and 57% in men; p=0.181). In those admitted with another Killip, 81% developed CS on the first day of hospitalization, 13% on the second day and 6% on the third day, with no differences according to gender.
Baseline characteristics according to gender are shown in Table 1
Table 1
Baseline characteristics of the population
| Total (n=278) | Female (n=83) | Male (n=195) | p | |
|---|---|---|---|---|
| Age (years) | 66 (59-75) | 71 (61-78) | 64 (58-73) | <0.001 |
| Hypertension | 206 (74) | 66 (80) | 140 (72) | 0.179 |
| Dyslipidemia | 95 (34) | 28 (34) | 67 (34) | 0.920 |
| Smoking | 72 (26) | 13 (16) | 59 (30) | 0.011 |
| Type 2 diabetes | 117 (42) | 35 (42) | 82 (42) | 0.494 |
| Obesity | 79 (29) | 26 (31) | 53 (27) | 0.483 |
| COPD | 19 (7) | 3 (4) | 16 (8) | 0.165 |
| Chronic anemia | 14 (5) | 5 (6) | 9 (5) | 0.623 |
| Chronic kidney disease | 17 (6) | 4 (5) | 13 (7) | 0.556 |
| Previous AMI | 44 (16) | 8 (10) | 36 (19) | 0.065 |
| Previous HF | 20 (7) | 6 (7) | 14 (7) | 0.483 |
| Previous stroke | 15 (5) | 4 (5) | 8 (4) | 0.781 |
AMI: Acute myocardial infarction; COPD: Chronic obstructive pulmonary disease; HF: Heart failure.
Quantitative variables are presented as median and interquartile range, qualitative variables as frequency and percentage.
The use of vasoactive agents was 97.8%, with no differences by gender according to the type of drug used, except for vasopressin, which was used in 7.2% of women and 16% of men (p=0.041). Mechanical ventilation was used in 52.5% of cases in both genders, Swan Ganz catheter in 17% (11% in women and 20% in men, p=0.073), intra-aortic balloon counterpulsation in 22.2% (14% in women and 26% in men, p=0.032) and extracorporeal membrane oxygenation (ECMO) in 1% of women and 3% of men, p=0.676). No other supports were used.
The culprit vessel was revascularized in 81% of the overall population, with no differences according to sex (80% of women vs. 82% of men, p= 0.768).The prevalence of multivessel disease was 71% (63% in women and 73% in men, p=0.113) and there was no difference in the prevalence of revascularization of other vessels, (40% in women and 31% in men, p=0.408).
In-hospital evolution by gender is detailed in Table 2.
Table 2
In-hospital evolution according to gender.
| Variable | Total (n=278) | Female (n=83) | Male (n=195) | p |
|---|---|---|---|---|
| Revascularization (CV) | 222 (81) | 65 (80) | 157 (82) | 0.768 |
| Angina/ reAMI | 9 (3) | 4 (5) | 5 (3) | 0.331 |
| Arrhythmias | 88 (32) | 26 (31) | 62 (32) | 0.939 |
| AF | 27(10) | 6 (7) | 21 (11) | 0.362 |
| VT/VF | 39 (14) | 11 (13,2) | 28 (14,3) | 0.808 |
| AV block | 16 (6) | 7 (8) | 9 (5) | 0.211 |
| Transient PM | 15 (5) | 2 (2) | 13 (7) | 0.151 |
| ECV | 36 (13) | 7 (8) | 29 (15) | 0.143 |
| Fever | 36 (13) | 11 (13) | 25 (13) | 0.922 |
| Dialysis | 20 (7) | 6 (7) | 14 (7) | 0.988 |
| Transfusion | 21 (8) | 7 (8) | 14 (7) | 0.717 |
| Mortality | 146 (53) | 41(49) | 105 (54) | 0.470 |
AF: atrial fibrillation; CV: culprit vessel; ECV: electrical cardioversion; PM: pacemaker; reAMI: reinfarction; VT/VF: ventricular tachycardia/ventricular fibrillation
Qualitative variables are presented as frequency and percentage.
The median (IQR) hospital stay was 6 days (1-16). Overall in-hospital mortality was 52.7%, with no differences between ACS with or without ST-segment elevation or according to gender: women 49% vs. men 54%, p=0.470).
The variables shown in Table 3 were considered for the analysis of univariate predictors of mortality
Table 3
Univariate analysis for mortality
| Dead (n= 146) | Alive (n= 132) | p | |
|---|---|---|---|
| Age (years) | 68 (60-78) | 65 (57-76) | 0.010 |
| Female gender | 41 (28) | 42 (32) | 0.470 |
| HTN | 113 (77) | 93 (71) | 0.223 |
| Smoking | 35 (24) | 36 (28) | 0.504 |
| Type 2 diabetes | 59 (40) | 58 (44) | 0.516 |
| Previous AMI | 30 (20) | 14 911) | 0.025 |
| STE-ACS | 114 (78) | 93 (71) | 0.175 |
| Revascularization | 111 (77) | 111 (87) | 0.041 |
| Swan Ganz | 25 (17) | 22 (17) | 0.988 |
| Balloon counterpulsation | 37 (26) | 24 (19) | 0.170 |
| MVD | 106 (73) | 91 (69) | 0.551 |
AMI: acute myocardial infarction; HTN: Hypertension; MVD: Multiple vessel disease; STE-ACS: ST-segment elevation acute coronary syndrome
Quantitative variables are presented as median and interquartile range, qualitative variables as frequency and percentage.
In the multivariate analysis model that included age, gender, diabetes, reperfusion and use of intra-aortic balloon counterpulsation, only age maintained its prognostic value (odds ratio 1.025, 95% CI 1.002-1.048, p=0.011).
In patients with STE-ACS without mechanical complications on admission (n=208) there were no differences in baseline characteristics; median (IQR) time to overall consultation was 300 min (120-780); 360 min (120-540) in women and 274 min (120-870) in men, p=0.196. AMI was anterior in 68% of cases (women: 55.9% vs. men: 72.5%, p=0.012) and percutaneous coronary intervention (PCI) was performed in 88.9% of women and 82% of men (p=0.149) and the door-to-balloon time was 120 min (60-240), without differences according to gender. There were 19.1% of failed PCI in women and 21.2% in men (p=0.398). Mortality in women was 54.2% and 55.4% in men (p=0.437).
DISCUSSION
LATIN Shock, the first Latin American study of CS in the context of ACS, allows us to learn about the reality of CS management in low-moderate income countries and at the same time, with a culture different from the European/American one, which could entail disparities according to gender.
It is well known that the proportion of women with CS due to infarction is higher than that of men, as shown by the Argentine ARGEN IAM ST registry (6) or the French FAST AMI study, in which it is almost twice that of men. (19) This is probably due, among other things, to the fact that women have a longer life expectancy and, in general, are older at the time of infarction with shock. In our case, women had a median age 7 years older than men.
The prevalence of women with CS in the different published studies and registries ranges from 21% to 37%. (20,21,22,23,24,25) In our study it was 30%. Women were older and did not present more risk factors or comorbidities than men, as has been observed in some studies. (22,23,24,25)
Revascularization is the mainstay in the treatment of CS, (26) but some studies reveal considerable differences according to gender. (27) It even emerges from the analysis of the National (nationwide) Inpatient Sample (NIS) database, with more than 134 000 elderly patients ( ≥75 years) with CS, that women were less likely to receive angiography, angioplasty and mechanical support compared with men. (28) In our study there were no significant differences in revascularization between men and women, probably because most of the participating centers had available angioplasty and current guideline recommendations were followed, (29,30) but there was a difference in the indication of mechanical support, which was significantly lower in women, with the indication for balloon counterpulsation being half that of men. Extracorporeal membrane oxygenation was used in less than 4% of cases, which reflects the lack of availability and/or implementation given the socioeconomic conditions in Latin America. However, with the results of the IABP-SHOCK II trial, (31) those of ECMO-CS (32) and of ECLS-SHOCK, (33,34) which did not show benefits in survival, its routine use is not proposed for either men or women. The DanGer Shock study (35) in which Impella was used on a randomized basis, showed lower mortality with the use of the device in the included population, but in the subgroup analysis, only men benefited from its use. In Latin America, Impella was not used in any patient, although it should be noted that the registry was carried out prior to the publication of that study.
Mortality in our environment was high and there were no differences by gender as in other studies; (36,37) however, it is on this point where there is more controversy, since some recent studies report higher mortality in women. (38,39,40 )
It should be noted that women may have some different baseline characteristics and that they are usually underrepresented in studies, but there have been no significant outcome differences with respect to gender, neither with revascularization (SHOCK trial), nor with the use of balloon counterpulsation (IABP-SHOCK II), or with revascularization of only the culprit vessel (CULPRIT-SHOCK). (41,42) There were also no differences according to gender in the use of other mechanical supports, except in the DanGer Shock study (35) in which the benefit of Impella was limited to the male group. In any case, it cannot be ruled out that this is due to the low number of women included. With the current data, both genders should continue to be treated equally. (43,44)
The heterogeneity of populations, treatment received and evolution makes it essential to have local and regional epidemiological data. Only by measuring and becoming aware of our own situation it is possible to evaluate whether it is necessary to implement change actions.
LIMITATIONS
The SCAI classification was not used, the registry did not report cardiac arrest at admission and there was no external audit of the data.
CONCLUSIONS
Latin American women who present with CS in the context of ACS are older than men, are revascularized in a similar manner, and have an equally high mortality. Although the use of mechanical supports was lower in women, this has not had an impact on mortality, nor has it had an impact on the results of randomized studies.
Conflicts of interest
Conflicts of interest None declared. (See authors' conflict of interests forms on the web).
ACKNOWLEDGEMENTS
To the centers and researchers who participated in the registry: Hospital El Cruce, Argentina: Dr Mariano Adamowski; Hospital Nacional Edgardo Rebagliati Martins, Peru: Dr Maicol Cortez Sandoval; Hospital Luis Vernaza, Ecuador: Dr Freddy Pow Chon Long; Instituto Cabral de Corrientes, Argentina: Dr Stella Macin; Hospital de especialidades Dr Teodoro Maldonado Carbo, Ecuador: Dr Julio Burgos Acosta, Instituto nacional cardiovascular INCOR, Peru: Dr Manuel Chacon; Sanatorio Güemes, Argentina: Dr Joaquin Perea, Hospital Cemesa, Honduras: Dr Francisco Somoza; Hospital Univalle Norte, Bolivia: Dr Claudia Paz Soldan Patiño; Instituto Cardiovascular Migone, Paraguay: Dr Miguel Quintana; Clinica Pasteur, Argentina: DrAndres Perelmuter; Instituto nacional de cardiologia Prof Dr Juan Cattoni, Paraguay: Dra Fabiola Rodriguez Caballero; Hospital Descentralizado Rawson, Argentina: Dra Maria De Los Angeles Navarta Navarro; Hospital Santojanni, Argentina: Dra Gabriela Velasco; Clinica Santa Isabel, Argentina: Dra Yanina Castillo Costa, Dr Flavio Delfino; Sanatorio Anchorena San Martin, Argentina: Dr. Juan Souto; Hospital Español de Mendoza, Argentina: Dr Valentina Rodriguez; Sanatorio Pasteur de Catamarca, Argentina: Dr Maria Pia Marturano; Sanatorio Sagrado Corazón, Argentina: Dr Diego Costa; Hospital de especialidades Eugenio Espejo, Ecuador: Dr Diego Rengifo Escobar; Clinica Modelo Lanus, Argentina: Dr Diego Novielli; Hospital de Clinicas, Argentina: Dr Sandra Swieszkowski; Sanatorio Bernal, Argentina: Dr Juan Kinaszuk; Clinica Bazterrica, Argentina: Dr Victor Mauro; Instituto Cardiovascular de Buenos Aires, Argentina::Dr Leonardo Seoane; Sanatorio Modelo de Quilmes, Argentina: Dr Adrian Hrabar; Hospital Obrero 2, Bolivia: Dr Ruben Coca Pozo, Hospital El Carmen, Argentina: Dr Jose Di Milta; Sanatorio Americano, Argentina: Dr Mario Ciafardoni; Sanatorio Adventista, Argentina: Dr Ramiro Ayala; Hospital Obrero 1, Bolivia: Dr Yhaquelina Quispe Villca; Hospital Barros Luco Trudeau, Chile: Dr Ricardo Ramirez, Clinica Privada Mayo, Argentina: Dr Eduardo Quinteros; Fundación Favaloro, Argentina: Dr Fabricio Procopio; Hospital Italiano Regional del Sur, Argentina: Dr Veronica Heredia; Hospital Santa Isabel de Hungría, Argentina: Dr Maria Victoria Haedo; Sanatorio Allende, Argentina: Dr Nicolas Zaderenko; Sanatorio Anchorena, Argentina: Dr Alessis Raffaeli; Sanatorio Finochieto, Argentina: Dr Diego Crippa; Caja Nacional de Salud, Bolivia: Dr Richard Urquieta Cayoja; Hospital Nacional Guillermo Almenara, Peru: Dr Ciro Barrantes