
“Let us hold to high ideals and strive to achieve greatthings, because life always falls short, and we rarelyachieve more than a fraction of what we hope for; byaiming high we will accomplish much more. For a steadfast will, nothing is impossible, there is no suchthing as easy or difficult; what is easy is what we already know how to do, and what is difficult is whatwe have not yet learned to do well.
”Dr. Bernardo Houssay
(first Nobel laureate fromArgentina and Latin America)
Three cardiologists from an imaginary world—Sergio Nonrich, Mirza Ten, and Mario Halcón—continue to debate the current state of the healthcare system. They wonder why healthcare is not a priority for either political programs or the general public. In this regard, we physicians observe the progressive decline of the healthcare system, without a sustained responsiveness that would allow it to be placed on the agenda of various national and/or provincial governments. Although the health crisis caused by the pandemic highlighted the shortcomings of a system that cries out for reform, the political class continues to postpone a genuine debate. It is imperative to rethink a healthcare model that transcends economic interests and recovers its fundamental essence: guaranteeing health as a universal right.
The number of working hours devoted to medical care has likely been impacted as a result of meager fees. The time dedicated to healthcare in Argentina has shown a progressive decline that has not only affected care assistance but has also increased the level of dissatisfaction, leading to a rise in the prevalence of burnout among healthcare professionals. (1-3)
There is no defined, uniform health care plan for the various public hospitals and health facilities. The provision of health services depends on the availability of healthcare personnel (and their specialties), equipment, supplies, and care capacity (e.g., available beds, appointment availability, etc.) at the time the demand arises. When demand exceeds supply, restrictions on access to health services emerge. Lack of systematic planning of the offer (or its financing) results in disparities among the different provinces.
The fragmentation and segmentation of the Argentine health system is not accidental; it stems from a historical lack of coordination among its three pillars (the state, the social welfare organizations, and the private sector) and from the country’s federal nature itself. (Figure 1) These structural divisions have, to date, prevented the efficient integration of health care. According to our Constitution, primary responsibility for the regulation, financing, provision, and supervision of health care lies with the provinces. Coordination on health matters among the national government, the provinces, and the Autonomous City of Buenos Aires is carried out through the Federal Health Council (COFESA), established by Law 22 373, within whose framework federal health policies and actions in the country are coordinated. (4)
Fig. 1
Estimated overall distribution of coverage by subsystem type 2022/23 (data provided by Prosanity Consultant)
| Type of coverage | Population covered n | Share % |
|---|---|---|
| State Subsystem | 16 500 000 | 36.00% |
| Social Security Subsystem (Social Insurance) | 27 928 500 | 60.97% |
| Private Subsystem | 6 321 500 | 13.57% |
| Total | 50 750 000 | 110.54% |
| Argentine Population | 45 808 000 | 100.00% |
| Population with more than one health plan | 4 942 000 | 10.54% |
Sustainable solutions cannot be achieved in a health care system unless models of care, management, and financing are integrated. Our federal system (23 provinces and the Autonomous City of Buenos Aires) is characterized by fragmentation, segmentation, and a lack of coordination among its components, with a lack of care standards, unevaluated or suboptimal outcomes, in health emergency since 2002, with a high degree of dissatisfaction (from patients, healthcare personnel, and providers), unequal access and quality, with infrastructure and resource problems (shortage of hospital beds and healthcare personnel), and with insufficient funding (healthcare investment is low). (5)
When addressing disparities in healthcare, it is important to recognize the difference between equality and equity. Equality refers to the provision of the same care for all people and leads to policies that ensure everyone has the same resources. Health equity is the state in which all people have a fair and equal opportunity to achieve their highest attainable level of health. Equity recognizes that those who have suffered exclusion or marginalization—both currently and historically—will generally require individualized resources to address the consequences of such exclusion and marginalization. From a healthcare perspective, we cannot reduce the patient to a client with varying levels of coverage; rather, we must view him as a citizen entitled to receive appropriate medical care. Equity takes into account barriers, circumstances, and conditions. In contrast, health inequity refers to differences that are unnecessary and preventable—and that are also considered unfair. Achieving equity requires eliminating barriers to health such as poverty, discrimination, and powerlessness, as well as their consequences—including lack of access to good jobs with fair wages, safe environments, education, housing, and quality medical care. (6)
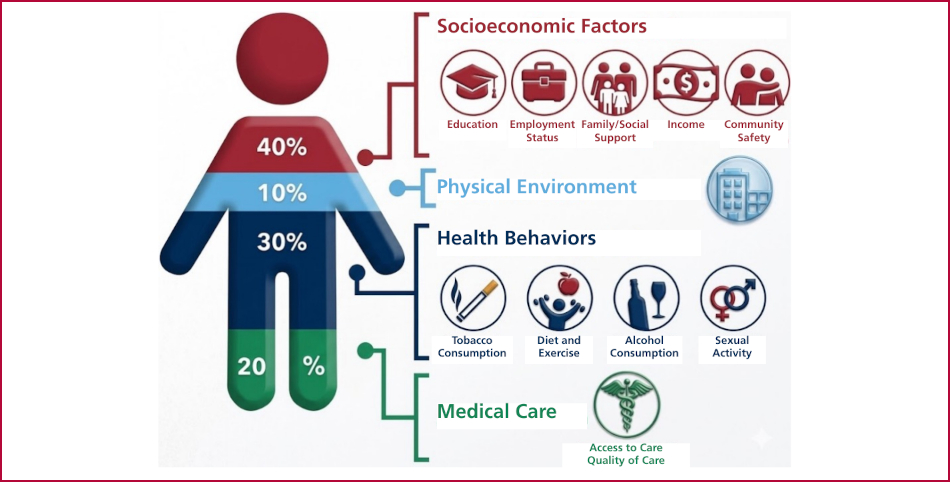
According to a survey by the Institute for Clinical Systems Improvement, 20% of a person’s health and wellbeing is related to access to care and quality of services; however, 80% of health outcomes are determined by the physical environment, social determinants, and behavioral factors (Figure 2). Socioeconomic factors, such as employment status, social support, income, community safety, and physical and environmental settings are just as important as more routinely assessed health behaviors, such as tobacco use, diet and exercise, alcohol consumption, and sexual activity. (7,8) In this sense, health is a multifaceted and complex issue linked to social, educational, and behavioral factors that involve stakeholders beyond healthcare personnel.
Fig. 2
Determinants of health status (modified from Prog Cardiovasc Dis. 2024;82:55-60. https://doi.org/10.1016/j.pcad.2024.01.005
Furthermore, the health area does not function as a conventional market for several compelling reasons. There is a clear imbalance in access to information and a demand that, by its nature, does not respond to
price changes (inelastic). Since no individual can afford comprehensive care on its own, health insurance becomes indispensable. If we add the impact of external phenomena such as health crises, it is undeniable that an indepth analysis, greater integration among stakeholders, and regulatory actions are required to correct these structural deficiencies. (
CONCLUSION
Considering the challenges facing the healthcare system, it is urgent to strengthen the authorities’ capacity to lead change processes. Effective transformation will only be possible if it is built collectively with all stakeholders (governance), focusing efforts on a common goal: achieving universal health coverage and access. The Argentine Society of Cardiology has decided to contribute to the debate of the healthcare personnel and the healthcare system situation through the creation of the 24 Leading Scientific Societies Forum.
Sergio BarattaMTSAC ![]()
President of the Argentine Society of Cardiology