
The discrepancy between the results of a treadmill exercise test (TET) and those of myocardial perfusion imaging poses a complex scenario. Although a “normal” SPECT (single-photon emission computed tomography) result suggests the absence of obstructive coronary artery disease, it does not necessarily ensure normal coronary circulation. Various macrovascular and/or microvascular conditions limit the increase in myocardial blood flow during exercise, without evidence of localized perfusion defects.
Treadmill exercise test is highly available, lowcost, noninvasive and commonly used for the early detection of coronary artery disease in asymptomatic patients (with a sensitivity of 68% and specificity of 76%) or to assess functional capacity and/or chronotropic response in various clinical settings. A TET is considered positive in the presence of a horizontal or downsloping ST-segment depression of at least 1 mm and/or the presence of angina or angina-like symptoms.
Rest-stress SPECT myocardial perfusion imaging (MPI) enhances the standard TET by providing tomographic images. It provides not only information on the presence or absence of perfusion abnormalities in arterial territories but also allows assessment of left ventricular ejection fraction (LVEF) and volumes during both phases of the test. The combination of both tests significantly increases the likelihood of detecting ischemic heart disease, with a sensitivity of 82% and a specificity of 77%.
Homogeneous MPI with normal ventricular volumes and LVEF has high negative predictive value —a low probability of presenting cardiovascular events. However, when the results of both methods are discordant (positive TET with “normal” MPI), the prognostic implications are unknown, and the therapeutic strategy is not clearly defined. (1)
We present two clinical cases with discordant findings.
CASE 1
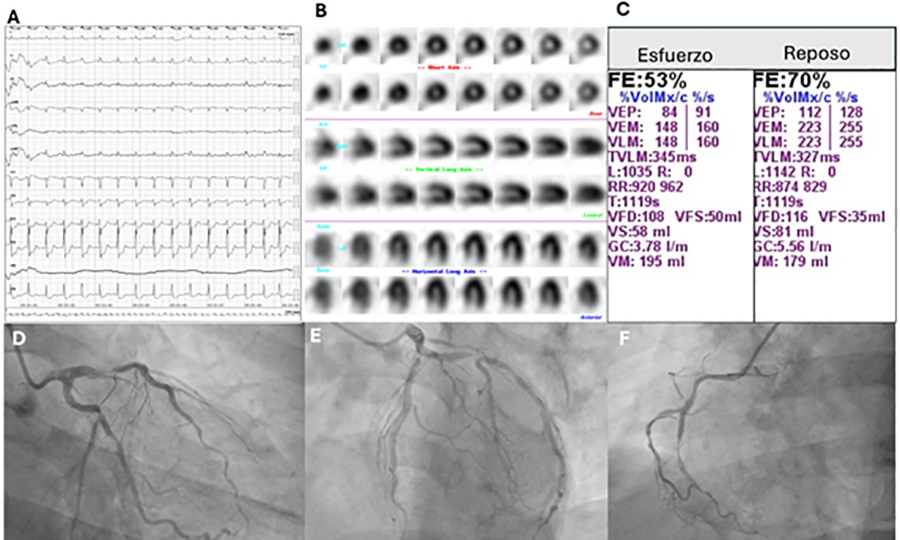
A 56-year-old male patient underwent a TET as part of the workup for a health certificate. The patient was an athlete with a history of hypertension under medical treatment and was currently asymptomatic. The TET was positive for ST-segment depression. Myocardial perfusion imaging with rest/stress SPECT was performed. The TET (Figure 1A) was positive, demonstrating a 4-mm horizontal ST-segment depression in leads V2 through V6 at 750 kgm/min (5.1 METs), with a tension-time index (TTI) of 20 002. The patient remained asymptomatic. There were no perfusion defects (Figure 1B). However, transient LV dilation and a 17% decrease in LVEF during peak exercise were identified as high-risk criteria (Figure 1C). Coronary angiography (CA) was performed, revealing three-vessel disease with severe stenosis in the mid left anterior descending coronary artery, mid left circumflex artery and lateral marginal artery, as well as chronic total occlusion in the mid right coronary artery with heterocoronary collateral circulation (Figure 1D-F).
CASE 2
A 57-year-old male patient presented with atypical chest pain with variable functional class. He had a history of dyslipidemia that was currently being treated. During a routine cardiovascular checkup, he underwent a TET that was positive for chest pain associated with a horizontal ST-segment depression during peak exercise at 1200 kgm/min (9.6 METs) with an ITT of 35,775 (Figure 2A). Myocardial perfusion was normal (Figure 2B). A coronary angiography was performed, which revealed no significant coronary artery lesions (Figure 2D and E). Therefore, noninvasive assessment of myocardial flow reserve (MFR) using dipyridamole and cold test was requested, resulting in MFR of 1.3 (normal value >2.0) and 0.5 (normal value >1.5), respectively (Figure 2C and F). This result was consistent with smooth muscle-dependent and endothelium-dependent microvascular dysfunction.

All patients gave their informed consent before undergoing these tests.
Discordant tests account for 4 to 24% of perfusion imaging tests. Previously, a positive TET result in the absence of significant coronary artery disease was considered a false positive. Today, the paradigm shift in our understanding of coronary artery disease has made us realize that epicardial circulation accounts for only 5% of the entire coronary artery tree, while the remaining 95% corresponds to microcirculation. (2)
We present two clinical cases with discordant findings, resulting from two distinctly different clinical scenarios:
In case 1, the TET was positive while the SPECT scan showed homogeneous perfusion with high-risk signs in the presence of severe multivessel obstructive coronary artery disease. In this scenario, homogeneous MPI results from balanced ischemia due to reduced blood flow across the various coronary artery territories; thus, regional hypoperfusion cannot be observed. (3)
On the other hand, the TET was positive in case 2 with homogeneous MPI and no high-risk signs in the absence of significant obstructive coronary artery disease. In this case, an imbalance between myocardial blood flow supply and demand is due to inadequate microcirculation vasodilation; this may or may not manifest as a perfusion defect, but it can be detected by quantifying MFR. (4)
Microvascular disease occurs when smooth muscle relaxation is impaired or when there is abnormal nitric oxide release due to endothelial dysfunction. (5) In both situations the reduction in MFR is associated with higher mortality and worse prognosis, with or without obstructive coronary artery disease. (6)
Based on the discussion so far, it is clear that a discordant result does not necessarily mean a falsepositive EST result (absence of myocardial ischemia). Conversely, it should raise suspicion of one of these two clinical scenarios, which must be evaluated in the context of a history of coronary artery disease, the presence or absence of symptoms, and their relationship to coronary artery anatomy. In the absence of significant stenosis, assessment of MFR should be considered.
An interpretation of MPI that incorporates the systematic assessment of each clinical and electrocardiographic finding will facilitate risk stratification and help to determine which patients should be selected for invasive tests or medical treatment.