
Infective endocarditis (IE) is predominantly an infection of the valvular endocardium, produced by endothelial damage due to microorganisms implanted via a hematogenous route, generating vegetations. (1) Despite improved understanding of its pathophysiology, more precise diagnostic methods and more effective antibiotics, it is associated with high morbidity and mortality, and even more than 50% of patients suffer some complication during its evolution. (2)
The EIRA-3 study carried out in Argentina showed an overall in-hospital mortality of 25.5% and established age over 65 years, history of kidney failure, mitral valve disease and the presence of heart failure as predictors of mortality. The most frequently isolated pathogens were Gram-positive cocci: Staphylococcus spp (46.3%), Streptococcus spp (28.2%) and Enterococcus spp (12.8%). The main in-hospital complications observed were persistent fever after initiation of antibiotic therapy, new kidney failure, peripheral embolisms and new heart failure. (3)
The aim of this communication is to present a clinical case with extensive structural cardiac involvement and multiple distant septic embolization. The clinical presentation, initial management, treatment of extracardiac complications and final surgical resolution will be analyzed.
We present the case of a 61-year-old male patient, smoker, with a history of human immunodeficiency virus (HIV) infection since 2000, on antiretroviral treatment with lamivudine and dolutegravir, right kidney atrophy with subsequent chronic kidney disease secondary to left obstructive uropathy (requiring renal replacement therapy from January 2022 to March 2023), non-insulin-requiring type 2 diabetes, and hospitalization for one month in February 2023 for bacteremia with rescue of multi sensitive Enterococcus faecium that responded to treatment with vancomycin.
He consulted on this occasion for disabling low back pain of 3-month evolution, and a magnetic resonance imaging (MRI) study showed discopathy at the L5-S1 level, indicating surgical resolution. Among the pre-surgical complementary examinations, a transthoracic echocardiogram revealed an image suggestive of tricuspid valve vegetation associated with moderate regurgitation (Figure 1), requiring hospitalization for study and treatment.
Fig. 1
Transthoracic echocardiogram in 4-chamber apical view. The right ventricle shows image compatible with tricuspid valve vegetation

Upon interrogation, the patient reported febrile episodes associated with non-productive cough, asthenia and weight loss of 10 kilograms in the past two months. On physical examination he was lucid, with mucocutaneous pallor, without signs of neurological focus, with clinical signs of heart failure, good ventilatory mechanics with cavitary murmur in the right lower lung field, isolated underlying fine crackling rales, attenuated first heart sound and normal second heart sound, systolic murmur of 3/6 intensity in aortic focus and diastolic murmur of 2/6 intensity in tricuspid focus, symmetrical extremities without edema and peripheral pulsus magnus et celer.
The admission electrocardiogram presented sinus rhythm, heart rate of 75 bpm and complete right bundle branch block. Laboratory analysis showed: hematocrit 26.9%, hemoglobin 8.90 g/dL, leukocyte count 14 910/mm3 (75% neutrophils), urea 116 mg/dL and creatinine 2.71 mg/dL. Chest X-ray revealed two cavitated images with hydro-aerial level in the right lower pulmonary lobe (Figure 2), with free costophrenic sinuses and no other pathological findings. In the simple chest and abdomen tomography, the presence of pulmonary abscesses and a hypodense image in the spleen were reported. A transesophageal echocardiogram exhibited severe aortic regurgitation and moderate tricuspid regurgitation, with vegetations in these valves and in the Chiari network (Figure 3). Blood culture samples were taken and vancomycin-resistant Enterococcus faecium (VRE)was found, so major (blood cultures and positive image) and minor (fever, peripheral embolic phenomena) criteria of the modified Duke diagnosis for IE were easily met. (4) Therefore, a targeted antibiotic regimen with linezolid was started.
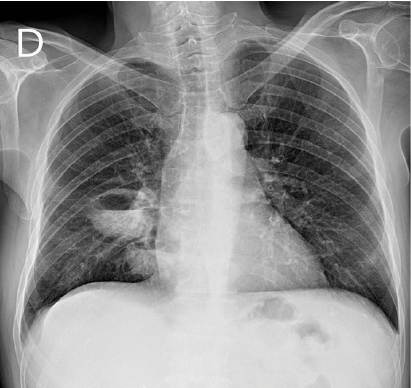
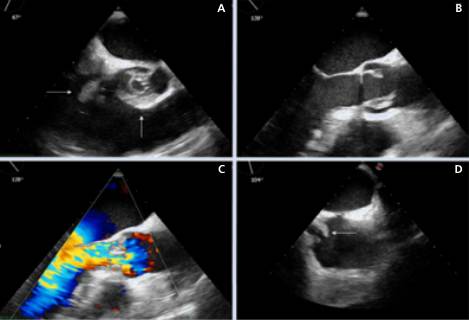
Fig. 3
Transesophageal echocardiogram. Image A shows an axial view at the basal level of the great vessels, with aortic valve compromise (vertical arrow) that prevents its correct closure, and the ventricular projection of a vegetation of the tricuspid septal leaflet (horizontal arrow). Image B shows a longitudinal view of the left ventricular outflow tract, with two vegetations in the aortic valve. Image C shows the color Doppler of the previous image, in which an aortic regurgitant flow in diastole can be observed. Image D shows a slightly rotated bicaval view in which a vegetation (horizontal arrow) can be seen over the mouth of the inferior vena cava, compatible with vegetation of the Chiari network
With respect to the pulmonary and splenic abscesses, the Percutaneous Surgery Service performed their drainage guided by tomography and fluoroscopy respectively, rescuing the same bacteria.
In conjunction with the Division of Infectious Diseases, a new MRI of the spine with gadolinium was performed due to suspicion of spondylodiscitis. Signal increase was observed in the prevertebral plane with fine laminar collections, which are initial signs of inflammatory changes compatible with incipient spondylodiscitis. As it was not a drainable collection, medical treatment was decided. Dentistry performed exodontia of tooth 4.5 due to the presence of penetrating caries.
The patient evolved with signs of heart failure for which he received intravenous treatment with loop diuretics. With negative water balance the clinical response was favorable. The patient evolved without leukocytosis or fever and with negative control blood cultures one week after starting antibiotic therapy.
As relevant intercurrences, after 15 days of treatment he presented thrombocytopenia that was interpreted as secondary to medullary toxicity of linezolid, so antibiotic therapy was rotated to daptomycin and minocycline. Once the infectious foci were controlled, coronary angiography was performed and no angiographically significant lesions were observed. Two hours after the procedure, the patient presented a febrile and clinical record compatible with acute cerebellar syndrome, which was interpreted as septic embolization associated with the procedure. Maintaining the antibiotic regimen, the symptoms subsided spontaneously after 48 hours. Hemodialysis was restarted due to an increase in nitrogen products. After multidisciplinary evaluation, surgery was decided. (4)
On the 53rd day of hospitalization, the Cardiovascular Surgery team performed aortic valve replacement with biological prosthesis number 23, subaortic repair and vegetectomy of the anterior leaflet of the tricuspid valve. There were no relevant postoperative intercurrences.
Methicillin-sensitive Staphylococcus aureus was recovered from the tricuspid valve, so antibiotic therapy was continued for two weeks after surgery, with negative control blood cultures, and control echocardiogram with no evidence of vegetations. It was decided to discharge him and he is currently under outpatient follow-up, with good therapeutic adherence and no new complications.
Patients diagnosed with HIV who present IE have a higher percentage of comorbidities and complications. (5) It is of utmost importance for these patients to have a close multidisciplinary approach and followup to help make quick and effective medical-surgical decisions, especially during the first days of hospitalization, which conditions the prognosis. Surgical resolution in this case is indicated once the non-valvular infectious foci are controlled, except in the case of hemodynamic complications, according to the guidelines.
Ethical considerations
Not applicable
Conflicts of interest
None declared. (See conflicts of interest forms on the website).