
We present the case of a 54-year-old female patient with a history of tobacco use, depression, and sedentary lifestyle who had previously consulted with a neurologist for chronic migraine without aura. The patient was referred by a psychiatrist for cardiological evaluation due to a panic disorder characterized by precordial pain and anxiety. She presented to consultation asymptomatic and alert. Blood pressure was normal, no murmurs were heard over the precordium or carotid arteries, and the neurological examination was normal.
Given the history of headaches, a computed tomography (CT) scan of the brain without contrast media was performed. A space-occupying lesion measuring 18 x 16 mm was observed, projecting above and to the left of the sella turcica. Peripheral calcifications were present, which could be indicative of a pituitary adenoma or a calcified aneurysm. For this reason, a multi-detector-row helical computed tomography angiography of the intracranial vessels was performed. At the level of the cervical region, the right internal carotid artery (ICA) presented a pronounced type-C kinking prior to its intrapetrous segment, along with a 7-mm neckless saccular aneurysm on its rostral aspect. On the internal surface of the supraclinoid segment of the left carotid artery, close to the origin of the ophthalmic artery, on its caudal aspect and extending posteriorly, there was an extensive giant saccular aneurysm measuring 18 x 13 mm. This aneurysm had a well-defined neck, isolated wall calcifications, and produced central displacement of the circle of Willis, predominantly affecting the A1 and M1 segments.
As the patient evolved with headache and decreased visual acuity a digital subtraction angiography was ordered. The right internal carotid artery (ICA) presented a saccular aneurysm without a neck on the C4 segment, and a giant M1 segment aneurysm with a well-defined neck was identified in the intracerebral left ICA. Given these findings, a selective angiography of both carotid and vertebral arteries, cerebral angiography, and 3D angiography of the left ICA were performed. Images consistent with fibromuscular dysplasia (FMD) were observed, along with dissection of both ICAs and the right vertebral artery in its cervical segment. A fusiform C1 segment pseudoaneurysm of the right ICA was also present. A 20-mm dissecting aneurysm was observed in the posterior communicating segment of the left ICA, with posterior direction.
After evaluating the therapeutic options, endovascular treatment was decided. The occlusion test showed opening of the anterior communicating artery, with adequate parenchymography in the left middle cerebral artery territory. The giant left ICA aneurysm was occluded using six detachable coils in the giant left posterior-segment ICA aneurysm, while preserving the wide aneurysm neck.
The patient was discharged free of symptoms. On follow-up imaging, selective catheterization of the left ICA revealed partial exclusion of the giant aneurysm in the posterior segment. Microcatheterization of the artery distal to the aneurysm was challenging due to the segment's pronounced curvatures and severe aneurysmal dysplasia. A 3.5 × 30-mm flow diverter was placed in the M2 segment of the left middle cerebral artery. The device was well-positioned against the arterial wall, completely covering the neck while preserving the carotid termination. Final angiograms showed a crescent sign within the aneurysmal remnant, with preservation of all normal arterial branches and a normal parenchymal phase. Regarding the right ICA pseudoaneurysm, surgery is indicated for symptomatic patients with high risk of morbidity and mortality. The possibility of placing a stent plus coils or a flow diverter was considered. However, given the presence of kinking and the challenges associated with passing the guidewire in an asymptomatic patient, medical treatment with aspirin and clopidogrel was chosen.
Internal carotid artery aneurysms, defined as a 50% or greater increase in the normal diameter of the vessel, are rare, accounting for 0.1% to 2% of all carotid procedures. When the traditional triad of neck pain, ipsilateral oculosympathetic paresis, and hemispheric ischemic symptoms is absent, the condition is underdiagnosed. Internal carotid artery aneurysms can be classified by pathophysiology or etiology. The pathophysiological classification divides these aneurysms into true aneurysms—which may be symptomatic or asymptomatic—and false aneurysms or pseudoaneurysms. According to their etiology, they may be post-traumatic (the most common etiology), associated with an underlying primary arteriopathy or connective tissue disorders (as Ehlers-Danlos syndrome type IV, Marfan syndrome, cystic medial degeneration, fibromuscular dysplasia), or atherosclerotic.
Cervical artery dissection (CeAD) is a frequent stroke etiology in young patients and accounts for 20% of strokes in patients < 45 years of age. Of all carotid artery diseases, extracranial ICA dissections account for 70–80%, while extracranial vertebral artery dissections constitute 15% of cases. Doppler ultrasound, magnetic resonance angiography, and computed tomography angiography are useful noninvasive diagnostic tests. The prognosis for extracranial carotid artery disease is better than that for intracranial disease. (1)
Fig. 1
A. Multidetectorrow helical computed tomography angiography of the intracranial vessels. Giant saccular aneurysm measuring 18 x 13 mm with a welldefined neck, on the internal surface of the supraclinoid segment of the left internal carotid artery (ICA), caudal aspect, in a posterior direction and close to the origin of the ophthalmic artery. B. Pseudoaneurysm of the right ICA. C. Dissection of the ICA

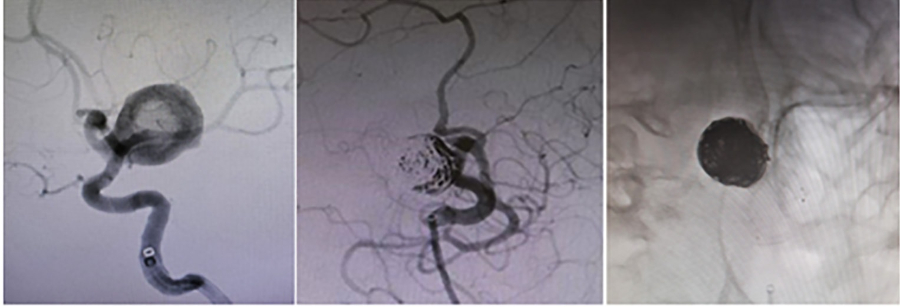
Fig. 2
A. Digital subtraction angiography. Giant M1 segment aneurysm of the left internal carotid artery (ICA) with a welldefined neck. B. Left ICA aneurysm was occluded using six controlledrelease coils, leaving the wide neck unembolized. C. A 3.5-mm SILK flow diverter placed in the M2 segment of the left middle cerebral artery. The device is wellpositioned against the arterial wall, completely covering the neck.
In a multicenter study of internal carotid and vertebral artery dissections, Bassi et al. reported that 63.2% were spontaneous dissections; in the remaining patients, trauma was the most common etiology. An ticoagulation was the treatment of choice in most patients. In patients with spontaneous ICA dissections, primary arteriopathy is generally suspected; however, angiographic changes consistent with fibromuscular dysplasia are found in 10% to 20% of cases. Schievink et al. reported the case of a patient with Marfan syndrome and bilateral carotid artery dissection without underlying arteriopathy, in whom microscopic examination revealed medial cystic necrosis of the aorta, and the left ICA displayed the typical features of fibromuscular dysplasia. (3)
Internal carotid artery dissection is a common cause of ischemic stroke, whether of embolic or hemodynamic origin; the therapeutic approach should be determined based on the mechanism of cerebral ischemia. (4)
The treatment of choice is anticoagulation or antiplatelet therapy; other procedures are used when medical treatment has failed. Endovascular treatment involves direct aneurysm embolization, sustainedrelease coil embolization, or coil embolization with stenting. Surgery is reserved for complex lesions. In the multicenter study by Byrne et al. (6), flow diverters were used to treat ICA aneurysms, including saccular, fusiform, wideneck, ruptured, or giant ventral aneurysms. Surgery was used only for complex lesions, large aneurysms with high risk of rupture, or radiological signs of expansion.
In asymptomatic patients, the size of a carotid aneurysm requiring intervention remains controversial, with experts recommending repair for diameters ranging from 15 to 30 mm, although it is generally accepted that aneurysms with a diameter >20 mm should be treated.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Ethical considerations
Not aplicable.