Valve-in-valve (ViV) transcatheter aortic valve replacement (TAVR) in small surgical bioprostheses presents a double challenge: the high risk of coronary obstruction and the potential for poor hemodynamic results. Coronary obstruction remains a critical threat during ViV-TAVR, with 30-day mortality rates of approximately 41%. (1) Small rings with high-profile struts require a strategy that ensures coronary patency while optimizing the effective orifice area (EOA). (2)
We present the case of a 72-year-old female with a failing 19-mm Biocor EPIC surgical bioprosthesis. Pre-procedural multislice computed tomography (MSCT) revealed extreme anatomical risk, which included 1.7-mm bilateral coronary heights and virtual narrow valve-to-coronary (VTC) distances: 2.2 mm (left) and 2.4 mm (right) (Figure 1). Furthermore, a narrow 22.5-mm mean diameter of sinotubular junction (STJ) indicated a high risk of sinus sequestration (Figure 2).
Given the ultra-high risk, a dual-protection strategy was planned. First, the LLAMACORN (Leaflet Laceration with Balloon-mediated Annihilation to Prevent Coronary Obstruction with Radiofrequency Needle) technique was performed on the left coronary cusp. This modification of electrosurgical techniques allows for controlled leaflet laceration, facilitating subsequent coronary access. (3) Simultaneously, bilateral chimney stents were positioned in the left main and right coronary arteries as a second safety net.
A 23-mm Evolut Pro+ self-expanding valve was successfully implanted. Self-expanding valves have shown superior hemodynamic performance in small
bioprostheses compared to balloon-expandable valves. (4) Following deployment, bioprosthetic ring fracture was performed using a high-pressure balloon to further optimize the EOA and minimize residual gradients. (5,6)
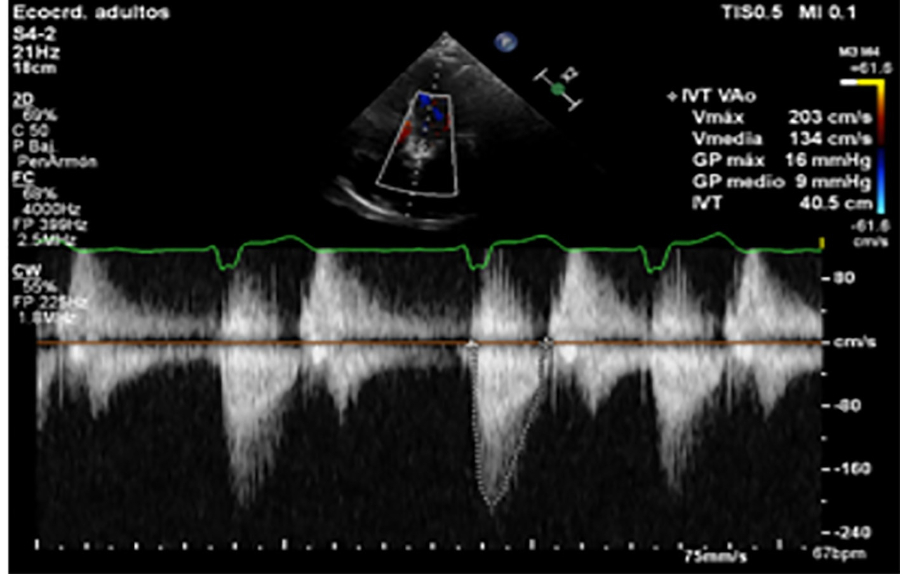
Final angiography confirmed coronary patency (TIMI 3 flow) without the need for chimney stent expansion on the right side, while the left chimney stent was optimized. Postprocedural echocardiography showed significant hemodynamic improvement, with a 9-mmHg final mean transvalvular gradient (Figure 3).
This case demonstrates that combining leaflet modification (LLAMACORN) with chimney stenting is a feasible and synergistic strategy for ultra-highrisk ViV-TAVR. While chimney stenting provides immediate protection, LLAMACORN ensures long-term coronary access, which is particularly vital when using supraannular selfexpanding valves in narrow aortic roots.
In conclusion, the "dual protection" workflow addresses both the immediate risk of coronary obstruction and the longterm need for coronary access. This approach appears to be safe and reproducible, offering a reliable strategy for procedural success and optimal hemodynamics in patients with failing small surgical bioprostheses and extreme anatomical risk.
Ethical considerations
Not aplicable.
Fig. 1
Pre-procedural MSCT Assessment of Coronary Risk. (A) Annulus perimeter (60.9 mm) and area (293 mm²). (B) VTC distances: 2.2 mm (left) and 2.4 mm (right). (C–D) Bilateral 1.7-mm coronary artery height.
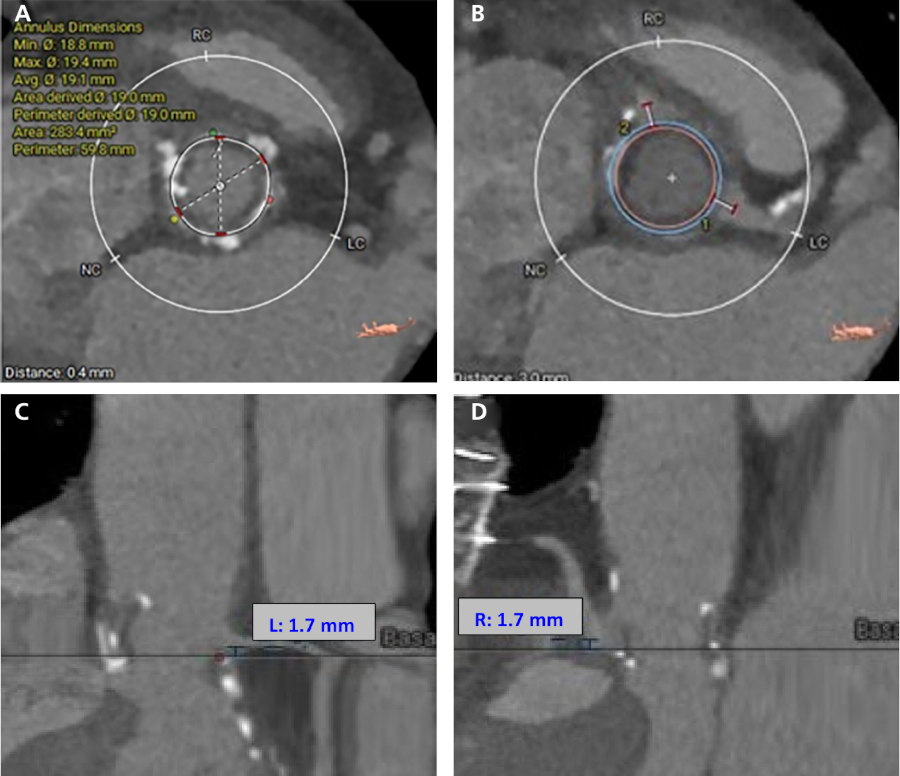
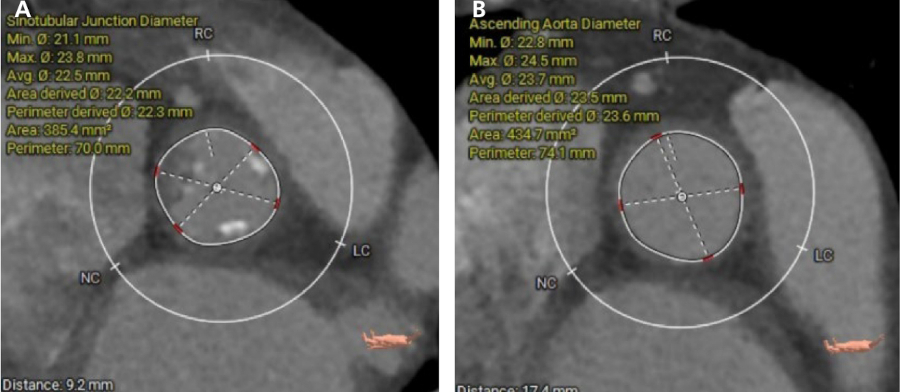
Fig. 2
MSCT Assessment of the aortic root architecture. (A) Measurement of the sinotubular junction (STJ) showing a narrow 22.5-mm mean diameter and a 9.2-mm height from the annulus plane. (B) Measurement of the ascending aorta: 23.7 mm. Note: The narrow STJ relative to the surgical ring highlights the high risk of sinus sequestration.