Rev Argent Cardiol 2024;92:183-188. http://dx.doi.org/10.7775/rac.v92.i3.20770
Received: 06/11/2023 Accepted: 04/04/2024
Correspondence: Federico Liberman. fliberman@icba.com.ar - Blanco Encalada 1543. Ciudad de Buenos Aires (C.P.1428), República Argentina.
MTSAC Miembro Titular de la Sociedad Argentina de Cardiología

INTRODUCTION
Currently, percutaneous coronary intervention (PCI) is the treatment of choice in cases of severe symptomatic coronary artery disease with favorable anatomy. (1,2) As a rule, patients undergoing elective PCI are monitored in a closed unit for at least 24 hours due to the risk of vascular access complications and acute events. (3) With advances in the angioplasty technique and new antithrombotic therapies, together with the new generation of stents and, fundamentally, the progressive and sustained shift from femoral to radial access, same-day discharge (SDD) is an increasing alternative. (4,5)
Multiple studies have demonstrated the safety of this strategy. (6,7) Both the American Society for Cardiovascular Angiography and Interventions Expert Consensus (updated in 2018) and the 2021 American College of Cardiology Expert Consensus have incorporated SDD as the standard of care for elective PCI. (8,9)
The implementation of SDD protocols following elective PCI has optimized the use of hospital resources by reducing the length and cost of hospital stay, while providing safe and effective patient care. (10) Early mobilization, along with early return to the home environment, represents a valuable strategy to mitigate physical deterioration and reduce the risk of infections and delirium associated with hospitalization. (11,12) In addition, a shorter hospital stay can have a positive impact on cost reduction by optimizing the use of limited medical resources, both in physical space and medical staff. (13) However, the lack of a model of care specifically designed for outpatient percutaneous procedures may affect the effectiveness of the program. (14)
In our center the PCI with SDD program was first implemented in the conventional inpatient area in 2015, and then, due to the increase in elective PCI volume and evidence support, an exclusive outpatient model of care was implemented in 2018 in a specific area, called Radial Lounge (RL). The RL is adjacent to a new cath lab with the highest standards of complexity and safety. It follows a defined medical program in terms of inclusion and exclusion criteria, and is prepared to treat a broad spectrum of cardiovascular diseases. This model has shown promising results in terms of operational efficiency and patient experience, but its impact on the outpatient PCI program has not been thoroughly studied.
The aim of this study was to evaluate the impact of the RL model in the PCI program with SDD, considering its safety, efficacy and patient experience.
METHODS
We conducted a retrospective observational cohort study in a high-complexity center, including patients undergoing elective PCI between 2018 and 2022 under the LR model of care.
Radial Lounge
The RL opened in July 2018 as an area dedicated to outpatient percutaneous procedures. It has 10 armchairs, a bed in a separate room (femoral box), a nursing office, an administrative area and a healthy snack bar. In all cases, patients are evaluated in a pre-procedure consultation with a cardiologist of the service, who reviews each case and considers the feasibility of SDD according to the pre-procedure checklist recommended by the 2021 ACC expert consensus. (8) In addition, the informed consent form specifying the risks of the procedure is explained and handed out on paper. Patients without exclusion criteria are received in the RL by a nurse who checks vital signs on admission, places an intravenous line and assigns them to a chair where they will wait until the procedure accompanied by a family member. Previous fasting is not required. (15) Subsequently, they are admitted to the hemodynamics room in their own clothes. In all cases, the operator chooses the access site. For radial (proximal or distal) or ulnar (left or right) access, hemostasis is performed using the Terumo™ TR Band radial compression device or compressive bandage for distal radial punctures. For femoral access, puncture is performed under ultrasound guidance and the Angio-Seal (Terumo™) arterial occluder device is used. After PCI, the patient remains in the LR chair for a minimum of 4 hours in case of radial or ulnar access and 6 hours in case of femoral access, except for those cases in which the interventional cardiologist in charge indicates hospitalization in a monitored unit due to some intercurrence during the procedure. The following complications of the procedure are considered: altered flow, side vessel compromise that generates precordial pain, untreated dissection, arterial perforation, vascular access complication or allergic reaction to the contrast medium. Observation in the RL ends with an evaluation by a clinical cardiologist and all patients are discharged with a follow-up appointment within 10 days after the procedure.
PCI program in the RL
All outpatients with an indication for a percutaneous procedure are previously evaluated in a consultation by a member of the Interventional Cardiology team. Clinical and social exclusion criteria have been developed for the admission of patients to the RL. In these cases, patients are referred to the conventional hospitalization area.
RL clinical exclusion criteria:
-
Requirement of permanent oxygen therapy (home oxygen).
-
Left ventricular ejection fraction <30%.
-
Weight >150 kg.
-
Need for dialysis or creatinine clearance <30 ml/min.
RL social exclusion criteria:
Complexity of the procedure
Procedural complexity is not part of the RL exclusion criteria. Therefore, patients with a complex anatomy can be admitted and treated in this setting. To assess the complexity of the procedures performed, the following criteria are taken into account: the Syntax score, use of rotational atherectomy (Rotablator), intravascular ultrasound (IVUS)-guided PCI, PCI for left main coronary artery (LMCA) and/or proximal left anterior descending artery and/or venous graft and/or bifurcation and/or chronic total occlusion.
Patient experience
Scores obtained from the Hospital Consumer Assessment of Healthcare Providers and Systems Survey (HCAHPS) are used to assess patient experience. (16 HCAHPS is a standardized survey tool that measures patients' perceptions of their hospital experience, including communication with healthcare providers, hospital environment hygiene and quietness, pain management, and overall hospital rating. We collected HCAHPS scores from patients who underwent elective PCI under the RL model and voluntarily completed the questionnaire.
Major adverse cardiovascular events (MACE)
To evaluate the safety of the RL model, in-hospital mortality, overall mortality, coronary reintervention and rate of 30-day rehospitalization were considered.
Data collection
Data were collected from the electronic medical records registration system and the digitized reporting system. Demographic data, clinical characteristics, procedure details, and outcomes were collected for all patients included in the study.
Ethics Committee
The present study was submitted to and approved by the institutional Ethics Committee.
Statistical analysis
Continuous variables are presented as mean ± standard deviation or median and interquartile range, as appropriate. Categorical variables are expressed as frequencies and percentages. The t test or Mann Whitney test were used to compare continuous variables, according to their distribution, and the chi-square test or Fisher's exact test were used to compare categorical variables between groups. A value of p<0.05 was considered statistically significant. All statistical analyses were performed with SPSS 25.0 (IBM Corp., Armonk, NY, USA).
RESULTS
A total of 2102 PCIs were included under the LR model of care. Among treated patients, 86.7% were male, and mean age was 67.1 ± 9 years. The mean number of vessels treated was 1.3 ± 0.5, and the mean number of stents implanted was 1.9 ± 1.0. Complexity criteria were identified in 46.7% of all the PCIs performed. The complete distribution of risk factors and complexity are presented in Table 1.
Table 1
Distribution according to risk factors and complexity of the procedure performed.
From 2018, when the RL program began, there was a sustained and progressive increase in the rate of PCIs with SDD over the years, and the number of hospitalizations for more than 24 hours in elective PCI procedures decreased (Figure 1). The RL SDD rate was 85.3% in the first year of implementation (2018) and reached 89% in 2022 (Figure 2).
Figure 1
Evolution of the elective percutaneous coronary intervention (PCI) program from 2015 to 2022. Implementation of the Radial Lounge (RL) model in 2018;

SDD: same-day discharge
Figure 2
Percentage of same-day discharge (SDD) vs. hospitalization for at least 24 hours in Radial Lounge.
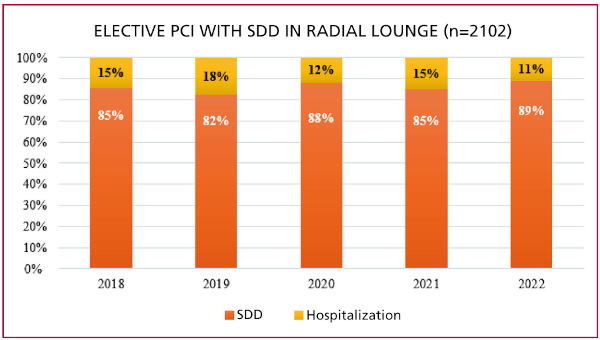
PCI: percutaneous coronary intervention; SDD: same-day discharge.
The voluntary response rate to the HCAHPS of patients undergoing elective PCI in the LR was 39.5%. The mean score received was 9.61/10.
Regarding PCI with SDD in the LR MACE, in-hospital and 30-day mortality was 0.1%; there was 0.4% coronary reinterventions and 0.5% rehospitalizations at 30 days (Table 2).
DISCUSSION
The main finding of our analysis was a significant increase in the volume of elective PCI with SDD since the introduction of the RL, currently reaching almost 80 % of all elective PCIs. The PCI program in the RL did not affect safety in terms of adverse events during hospitalization or at 30 days. These results are in line with the current approach of healthcare institutions that seeks to optimize resource utilization, and improve patients’ satisfaction without affecting their safety. (17,18,19)
Reducing the length of stay is essential to prevent the development of complications associated with hospitalization and the time to social reintegration of patients. This is especially beneficial in elderly populations, as it decreases the potential harms associated with hospitalization, such as infections, falls or cognitive impairment. (20 ) Many reports have estimated that each additional night in the hospital increases the risk of adverse drug reactions by 0.5% and the risk of infections by 1.6%. (21,22) In addition, this has had a significant impact on hospital resources by avoiding unnecessary bed occupancy, especially in light of the latest COVID-19 pandemic. In our study, out of the total number of elective PCIs performed in the RL during the 5 years analyzed, 1812 were with SDD, resulting in an average of 362 free beds per year. In a study conducted at the London Chest Hospital, similar results to those mentioned above were observed. Specifically, there was a 48.9% increase in the SDD rate following the implementation of an area specifically designed for outpatient procedures, resulting in an estimated savings of 595 bed-days due to decreased overnight admissions in this patient group. (23)
Patient experience was also assessed in a study conducted in Switzerland, where a 97% "complete satisfaction" rate was observed with the use of a five-item questionnaire after elective PCI with SDD in an LR model. (24) This demonstrates a clear improvement of patient experience by avoiding admission to a common area of the hospital for an outpatient procedure that in itself can be very stressful for the patient and family.
Finally, SDD after elective PCI has proven to be a safe strategy. Recently, the largest case series of SDD after elective PCI was published. This study included 819 091 patients from 1716 centers, and when SDD vs. hospitalization for at least 24 hours groups were compared, 30-day mortality was identical throughout the follow-up period. (25) Multiple studies have been performed on safety in SDD, but few have been published so far performed under a different than conventional model of care. (23,26,27,28,29) As in the work published by Brewster et al., the RL model of care did not affect outcomes in terms of MACE during a 30-day follow-up. (23)
Limitations of this study include the retrospective design, which may be subject to selection bias and confounding by indication. In addition, the study was conducted in a single high-complexity center, which may limit the generalization of the findings. Finally, the satisfaction surveys were answered voluntarily by a percentage of the total number of patients, so there may be response bias .
In conclusion, the implementation of a specially designed care model such as RL proved to be safe and effective, with evidence of impact on the SDD rate. In addition, the reported patient experience was higher than 9.5/10 points in this model of care.
Conflicts of interest
None declared. (See authors conflicts of interest forms in the website).
Financing
None
REFERENCES
3. Rangé G, Hakim R, Etienne CS, Deballon R, Dechery T, Souteyrand G, et al. Thrombose de stent : une bataille gagnée ? (Données du registre France PCI) [stent thrombosis : A won battle ? (data from the France PCI registry)]. Ann Cardiol Angeiol (Paris). 2021;70:388-94. French. https://doi.org/10.1016/j.ancard.2021.10.001
5. Valgimigli M, Gagnor A, Calabró P, Frigoli E, Leonardi S, Zaro T, et al; MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: a randomised multicentre trial. Lancet. 2015;385:2465-76. https://doi.org/10.1016/S0140-6736(15)60292-6
8. Seto AH, Shroff A, Abu-Fadel M, Blankenship JC, Boudoulas KD, Cigarroa JE, et al. Length of stay following percutaneous coronary intervention: An expert consensus document update from the society for cardiovascular angiography and interventions. Catheter Cardiovasc Interv. 2018;92:717-31. https://doi.org/10.1002/ccd.27637.
9. Writing Committee; Rao SV, Vidovich MI, Gilchrist IC, Gulati R, Gutierrez JA, Hess CN, et al. 2021 ACC Expert Consensus Decision Pathway on Same-Day Discharge After Percutaneous Coronary Intervention: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2021;77:811-25. https://doi.org/10.1016/j.jacc.2020.11.013
12. Kim M, Muntner P, Sharma S, Choi JW, Stoler RC, Woodward M, et al. Assessing patient-reported outcomes and preferences for same-day discharge after percutaneous coronary intervention: results from a pilot randomized, controlled trial. Circ Cardiovasc Qual Outcomes. 2013;6:186-92. https://doi.org/10.1161/CIRCOUTCOMES.111.000069
16. Milligan G. An Introduction to the HCAHPS Survey. Nurse Educ. 2021;46:E89. https://doi.org/10.1097/NNE.0000000000000981
17. Amin AP, Patterson M, House JA, Giersiefen H, Spertus JA, Baklanov DV, et al. Costs Associated With Access Site and Same-Day Discharge Among Medicare Beneficiaries Undergoing Percutaneous Coronary Intervention: An Evaluation of the Current Percutaneous Coronary Intervention Care Pathways in the United States. JACC Cardiovasc Interv. 2017;10:342-51. https://doi.org/10.1016/j.jcin.2016.11.049
18. Alharbi S, Alasmari A, Hanafy E, Ellawindy A. Reduction of hospital bed cost for inpatient overstay through optimisation of patient flow. BMJ Open Qual. 2023;12:e002142. https://doi.org/10.1136/bmjoq-2022-002142
19. Rinfret S, Kennedy WA, Lachaine J, Lemay A, Rodés-Cabau J, Cohen DJ, et al. Economic impact of same-day home discharge after uncomplicated transradial percutaneous coronary intervention and bolus-only abciximab regimen. JACC Cardiovasc Interv. 2010;3:1011-9. https://doi.org/10.1016/j.jcin.2010.07.011
20. Smith TO, Sreekanta A, Walkeden S, Penhale B, Hanson S. Interventions for reducing hospital-associated deconditioning: A systematic review and meta-analysis. Arch Gerontol Geriatr. 2020;90:104176. https://doi.org/10.1016/j.archger.2020.104176
21. Eggli Y, Halfon P, Piaget-Rossel R, Bischoff T. Measuring medically unjustified hospitalizations in Switzerland. BMC Health Serv Res. 2022;22:158. https://doi.org/10.1186/s12913-022-07569-3
22. Damiani G, Pinnarelli L, Sommella L, Vena V, Magrini P, Ricciardi W. The Short Stay Unit as a new option for hospitals: a review of the scientific literature. Med Sci Monit. 2011;17:SR15-9. https://doi.org/10.12659/msm.881791
23. Brewster S, Khimdas K, Cleary N, Penswick A, Cliffe S, Weerackody R, et al. Impact of a dedicated "radial lounge" for percutaneous coronary procedures on same-day discharge rates and bed utilization. Am Heart J. 2013;165:299-302. https://doi.org/10.1016/j.ahj.2012.10.003
24. Biasco L, Pedrazzini GB, Araco M, Petracca F, Del Monte D, Sürder D, et al. Evaluation of a protocol for same-day discharge after radial lounge monitoring in a southern Swiss referral percutaneous coronary intervention centre. J Cardiovasc Med (Hagerstown). 2017;18:590-5. https://doi.org/10.2459/JCM.0000000000000519
25. Bradley SM, Kaltenbach LA, Xiang K, Amin AP, Hess PL, Maddox TM, et al. Trends in Use and Outcomes of Same-Day Discharge Following Elective Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2021;14:1655-66. https://doi.org/10.1016/j.jcin.2021.05.043
26. Bertrand OF, De Larochellière R, Rodés-Cabau J, Proulx G, Gleeton O, Nguyen CM, et al; Early Discharge After Transradial Stenting of Coronary Arteries Study Investigators. A randomized study comparing same-day home discharge and abciximab bolus only to overnight hospitalization and abciximab bolus and infusion after transradial coronary stent implantation. Circulation. 2006;114:2636-43. https://doi.org/10.1161/CIRCULATIONAHA.106.638627
27. Heyde GS, Koch KT, de Winter RJ, Dijkgraaf MG, Klees MI, Dijksman LM, et al. Randomized trial comparing same-day discharge with overnight hospital stay after percutaneous coronary intervention: results of the Elective PCI in Outpatient Study (EPOS). Circulation. 2007;115:2299-306. https://doi.org/10.1161/CIRCULATIONAHA.105.591495
28. Abdelaal E, Rao SV, Gilchrist IC, Bernat I, Shroff A, Caputo R, et al. Same-day discharge compared with overnight hospitalization after uncomplicated percutaneous coronary intervention: a systematic review and meta-analysis. JACC Cardiovasc Interv. 2013;6:99-112. https://doi.org/10.1016/j.jcin.2012.10.008
29. Rao SV, Kaltenbach LA, Weintraub WS, Roe MT, Brindis RG, Rumsfeld JS, et al. Prevalence and outcomes of same-day discharge after elective percutaneous coronary intervention among older patients. JAMA. 2011;306:1461-7. https://doi.org/10.1001/jama.2011.1409