http://dx.doi.org/10.7775/rac.v91.i1.20591
ORIGINAL ARTICLE
Prognostic Value of NT-proBNP in
Asymptomatic Patients with Severe Aortic Stenosis and Preserved Left
Ventricular Ejection Fraction
Utilidad
del NT-proBNP en la evaluación pronóstica de pacientes con estenosis aórtica
grave asintomáticos, con fracción de eyección ventricular izquierda preservada
Cintia S. LaurenzanoMTSAC, 1,
Daniel A. Chirino NavartaMTSAC, 1, María F. Cerda Jorgi1,
Alejandra Diaz Casale1
1 Jonas Salk OSECAC Outpatient Center,
Buenos Aires, Argentina.
Address for reprints: Cintia S Laurenzano, Tte. Gral. Juan Domingo Perón 2354, CABA. Phone 011-52764100. E-mail: cintia_cda@hotmail.com
ABSTRACT
Background: The aortic valve replacement (AVR) indication in asymptomatic patients
with severe aortic stenosis (AS) and preserved function is being increasingly
discussed.
Objective: The aim of this study was to evaluate whether the elevation of
N-terminal fraction of the pro-B-type natriuretic peptide (NT-proBNP) predicts
the occurrence of symptoms and the AVR indication in patients with severe AS
and preserved left ventricular ejection fraction (LVEF), initially asymptomatic.
Methods: Asymptomatic patients with severe AS, preserved LVEF (≥55%) and
no initial AVR indication were prospectively included. All patients underwent
laboratory tests measuring NT-proBNP at baseline, and an echocardiogram with
tissue Doppler recording the lateral wall S wave (lat. S) and the E/e´ ratio.
The endpoint was the aortic valve replacement indication at follow-up.
Results: We included 133 patients aged 69 ± 8 years, 49% of which were women.
After a follow-up of 570 (interquartile range 380-680) days, 23.3% (n=31) of
them required aortic valve replacement. In the multivariate analysis, NT-proBNP
value and the E/e' ratio were independent predictors of surgery (HR 1.02, 95%
CI 1.001-1.03, p<0.001 and HR 1.42, 95% CI 1.21-2.45, p< 0.001, respectively).
NT-proBNP presented an area under the curve (AUC) greater than the E/e’ ratio
(0.88 versus 0.64, p=0.02). The best NT-proBNP cut-off point was determined as
>350 pg./mL (adjusted HR 1.55, 95% CI 1.38-2.01,
p<0.001).
Conclusion: NT-proBNP value and the E/e' ratio were independent predictors of AVR
requirement. NT-proBNP had a very good discrimination capacity, greater than
the E/e´ ratio.
Keywords: Aortic Valve Stenosis - Biomarkers - Natriuretic Peptide, Brain
RESUMEN
Introducción: La indicación de
reemplazo valvular aórtico (RVA) en pacientes con estenosis aórtica (EA) grave
asintomáticos con función conservada es motivo de creciente debate.
Objetivo: Evaluar si la
elevación del NT-proBNP predice la aparición de síntomas y la indicación de reemplazo
valvular en pacientes inicialmente asintomáticos, con EA grave y fracción de
eyección ventricular izquierda (FEVI) conservada.
Materiales y métodos: Se incluyeron en
forma prospectiva pacientes con EA grave, FEVI conservada (≥55%) que
fueron considerados asintomáticos, sin indicación inicial de RVA. A todos se
les realizó laboratorio con medición de NT-proBNP en forma basal y
ecocardiograma con Doppler tisular consignando la onda S de la pared lateral (S
lat) y la relación E/e´. Se consideró como punto final el requerimiento de
reemplazo valvular durante el seguimiento.
Resultados: Se incluyeron 133
pacientes con una edad de 69 ± 8 años, 49% mujeres. Luego de un seguimiento de
570 (rango intercuartilo 380-680) días, el 23,3 % (n=31) de los pacientes
presentaron requerimiento de reemplazo valvular. En el análisis multivariado,
el NT-proBNP y la relación E/e´ fueron predictores independientes de
requerimiento de cirugía (HR 1,02, IC95% 1,001-1,03, p<0,001; y HR 1,42,
IC95% 1,21-2,45, p<0,001, respectivamente). El NT-proBNP presentó un Área
Bajo la Curva (ABC) mayor que la relación E/e´ (0,88 versus 0,64, p=0,02). Se
estableció como mejor punto de corte de NT-proBNP un valor >350 pg/mL (HR
ajustado 1,55, IC95% 1,38 – 2,01, p<0,001).
Conclusiones: El NT-proBNP y la
relación E/e´ fueron predictores independientes de requerimiento de cirugía. El
NT-proBNP presentó una muy buena capacidad de discriminación, mayor que la
relación E/e´.
Palabras Clave: Estenosis de la
válvula aórtica - Biomarcadores - Péptido Natriurético Encefálico
Received: 09/22/2022
Accepted: 11/02/2022
INTRODUCTION
Aortic
stenosis (AS) is the most common valvular disease in Western countries.
Prevalence increases with age, reaching 4-7% in patients over 65. (1) The only
effective treatment is aortic valve replacement (AVR), either via surgery or
percutaneously. AVR indication is evident and recommended in symptomatic
patients with severe AS, as well as in patients with impaired ventricular
function despite absence of symptoms. (2-4)
While it is
recognized that symptoms are one of the main prognostic markers of severe AS, (5,6) some series show that natural
progress in asymptomatic patients is not exempt from complications. (7,8) In addition, surgical mortality has
reduced over the years, (9) and percutaneous aortic replacement
has advanced. (10) This makes the risk/benefit ratio of
early intervention increasingly favorable. It is also important to note that
symptoms, as defined, are subjective features which are highly variable
according to the patient. This makes them difficult
to identify, especially in elderly patients.
Therefore,
using biomarkers for risk stratification of patients with severe AS has become
more appealing. The N-terminal fraction of the pro-B-type natriuretic peptide
(NT-proBNP) is one of the most common biomarkers resulting in an adverse and
more fatal prognosis when increased. (11,12)
The objective
of this study is to assess whether increased NT-proBNP can predict symptoms and
AVR indication in patients with severe AS and preserved left ventricular
ejection fraction (LVEF), initially asymptomatic.
METHODS
An
observational, prospective, single-site study was conducted enrolling patients
with severe AS and preserved LVEF under outpatient follow-up in the site’s
Valvular Heart Disease Department, who were considered asymptomatic and had no
initial indication of aortic valve replacement. Patients were enrolled from
July 2017 to July 2021.
All the
patients had an echocardiogram performed with the Esaote MyLab Seven equipment
(Florence, Italy) with a multi-frequency probe (1.5 MHz to 2.6 MHz), and the
following parameters were evaluated: aortic valve peak velocity (V max), mean
pressure gradient (MG), aortic valve area (AVA) by continuity equation, LV
diastolic and systolic diameters (LVDD and LVSD, respectively), left
ventricular mass index (LVMI), pulmonary artery systolic pressure (PASP), and
LVEF using Simpson’s biplane formula. Furthermore, the lateral wall tissue S
wave (lat. S) and E/e’ ratio were determined.
Severe AS was
defined as a V max ≥4 m/s, MG ≥40 mmHg, and AVA ≤1 cm2.
Ventricular function
was considered preserved if LVEF was ≥55%.
Exclusion
criteria: Patients who were symptomatic upon assessment, or for whom the
physical examination showed clinical signs of heart failure. Patients with
suspected symptoms had an exercise stress test according to the Naughton
protocol. Patients with symptoms or a systolic pressure flat curve during
exercise were considered symptomatic and therefore excluded. Patients with
impaired ventricular function (LVEF ≤55%) and dilated left ventricle
(diastolic diameter >60 mm) were also excluded.
An NT-proBNP
assessment was required for all patients in the site’s laboratory using Vitros
5600 equipment after the first visit.
Follow-up was
performed by means of clinic visits. The primary endpoint was the AVR
requirement.
Statistical
analysis
Continuous
variables are expressed as mean ± standard deviation,
or median and interquartile range (IQR) based on a normal or abnormal
distribution, and categories are expressed as percentages. For continuous
variables, group comparisons between AVR and non-AVR patients were performed
using Student’s t test for normal distributions and Mann-Whitney test for
abnormal distributions. Categorical variables were compared using the
chi-square test or the Fisher exact test when a variable showed an absolute
<5 frequency.
The
univariate analysis was performed using Cox regression, considering AVR as the
dependent variable, and both NT-proBNP and several echocardiographic parameters
as predictive variables. Those variables that were significant for the
univariate analysis (considering p<0.05) were analyzed using a multivariate
model through the proportional hazards regression method to assess variables
that are independently associated with the AVR requirement.
Then,
receiver operating characteristic (ROC) curves were developed, with the
corresponding area under the curve (AUC), and the best cutoff point was
established for significant variables in the multivariate analysis.
Finally, an
event-free survival test was performed using the Kaplan-Meier method.
Statistix 7
and Epidat 3.1 softwares were used for the analysis.
Ethical
considerations
This
observational study was approved by the ethics committee of the institution and
all the patients included, signed the informed consent.
RESULTS
One hundred
seventy-five patients were evaluated, 27 of whom were excluded as they were
considered symptomatic (19 upon the initial interview, and 8 after an exercise
stress test); 13 patients had impaired ventricular function, and 2 could not
have an NT-proBNP assessment. Therefore, 133 patients aged 69 ± 8 were
enrolled, 49% were female (n=65). The most common cause of AS was
sclerodegenerative aortic valve (70%, n=93), followed by bicuspid (25.5%, n=34)
and rheumatic (4.5%, n=6) aortic valve. Table 1 shows the
patients’ clinical and echocardiographic characteristics.
Table 1. Baseline demographics
|
Total (n=133) |
AVR requirement
(n=31) |
No AVR
requirement (n=102) |
P |
|
|
Age |
69 ± 8 |
69 ± 5 |
69 ± 8 |
0.45 |
|
Female |
65 (49.1) |
15 (48.3) |
50 (49) |
0.31 |
|
SBP (mmHg) |
130 ± 28 |
128 ± 32 |
130 ± 27 |
0.32 |
|
Medical history Hypertension Diabetes Atrial fibrillation |
95 (71.4) 29 (21.8) 13 (9.7) |
22 (70.9) 7 (22.5) 3 (9.6) |
73 (71.5) 22 (21.5) 10 (9.8) |
0.72 0.89 0.77 |
|
Echocardiogram LVEF (%) LVDD (mm) IVS (mm) LVMI (g/m2) LAA (cm2) |
64 ± 4 49 ± 5 12 ± 3 98 ± 38 26.9 ± 6.7 |
65 ± 3 49 ± 8 13 ± 3 99 ± 41 27.2 ± 6.9 |
64 ± 3 49 ± 7 12 ± 4 97 ± 39 26.5 ± 6.5 |
0.23 0.83 0.12 0.42 0.11 |
|
Doppler V max (m/sec) AVA index (cm2/m2) MG (mmHg) |
4.2 ± 0.4 0.58 ± 0.09 45 ± 5 |
4.5 ± 0.8 0.57 ± 0.1 46 ± 4 |
4.2 ± 0.5 0.58 ± 0.09 45 ± 4 |
0.11 0.62 0.32 |
|
Tissue Lateral S wave (m/s) E/e´ ratio |
0.08 ± 0.01 7.3 ± 1.5 |
0.07 ± 0.01 8.6 ± 2 |
0.08 ± 0.01 7.1 ± 1.3 |
0.07 0.04 |
|
NT-proBNP (pg/mL) |
110 (62.3-310) |
290 (75-450) |
85 (55-180) |
0.01 |
Categorical
variables are presented as n (%). Continuous variables are presented as mean ±
standard deviation or median (interquartile range)
AVA index:
aortic valvular area indexed according to body surface. IVS: intraventricular
septum. LAA: left atrium area. LVDD: left ventricular diastolic diameter LVEF:
left ventricular ejection fraction. LVMI: left ventricular mass index. MG: mean
gradient. SBP: systolic blood pressure. V max :
maximum aortic valve velocity.
The median
follow-up was 570 days (IQR 380-680), and 23.3% (n=31) of patients required an
AVR. As observed in Table 1, the group requiring AVR had a
higher baseline NT-proBNP: 290 (IQR 75-450) vs. 85 (IQR 55-180) pg/mL , p=0.01,
with a higher E/e’ ratio (8.6 ± 2 vs. 7.1 ± 1.3, p=0.04), a tendency towards a
lower tissue S wave (0.07 ± 0.01 m/s vs. 0.08 ± 0.01 m/s, p=0.07), and no difference
for the remaining parameters.
Table 2 shows the
univariate and multivariate analysis. In the univariate analysis, NT-proBNP,
the E/e´ ratio and lat. S were predictors of the AVR requirement. In the
multivariate analysis, NT-proBNP and E/e´ ratio were independent predictors of
the surgery requirement: HR 1.02 (95% CI 1.001-1.03), p<0.001,
and HR 1.42 (95% CI 1.21-2.45), p<0.001, respectively.
Table 2. Univariate and multivariate analysis
|
|
Univariate analysis |
Multivariate analysis |
||
|
|
HR (95% CI) |
p |
HR (95% CI) |
P |
|
SBP |
1.00 (0.96-1.04) |
0.33 |
-- |
|
|
LVEF |
0.98 (0.97-1.12) |
0.56 |
-- |
|
|
LVMI |
1.01 (0.93-1.05) |
0.22 |
-- |
|
|
V max |
1.03 (0.99-1.12) |
0.11 |
-- |
|
|
MG |
1.02 (0.89-1.23) |
0.23 |
-- |
|
|
LAA |
1.32 (0.99-1.98) |
0.09 |
-- |
|
|
Lateral S wave |
1.21 (1.115-1.88) |
0.01 |
1.18 (0.97-1.72) |
0.09 |
|
E/e´ ratio |
1.52 (1.22-2.63) |
<0.001 |
1.42 (1.21-2.45) |
<0.001 |
|
NT-proBNP |
1.04 (1.01-1.04) |
<0.001 |
1.02 (1.001-1.03) |
<0.001 |
LAA: left
atrium area. LVEF: left ventricular ejection fraction. LVMI: left ventricular
mass index. MG: mean gradient. SBP: systolic blood pressure.
V max : maximum aortic valve velocity
The AUC for
NT-ProBNP was 0.88 (95% CI 0.81- 0.91), and the best cut-off point was 350 pg./mL, while the AUC for the E/e´ ratio was 0.64 (95% CI
0.52- 0.68), significantly lower than that of the NT-proBNP (p=0.02). See Figure 1.
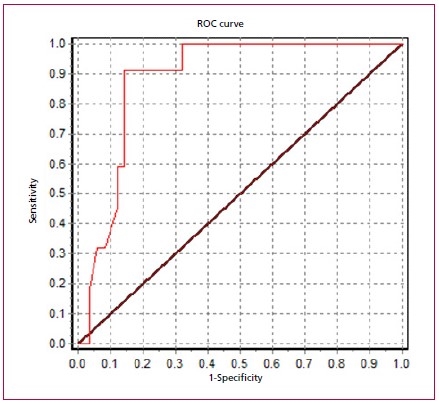
Fig. 1. ROC curve for the NT-proBNP.
The NT-proBNP
>350 pg./mL showed an adjusted HR of 1.55 (95% CI
1.38-2.01), p<0.001. Figure 2 shows the corresponding Kaplan-Meier
curve.
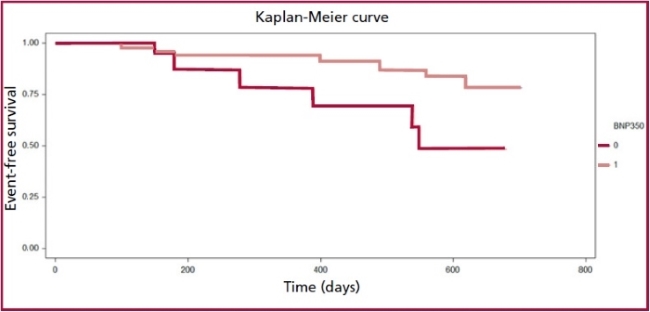
AVR: aortic
valve replacement. BNP350: 0: ≤350 pg/mL. 1: >350
pg/mL
Fig. 2. AVR prediction based on the NT-proBNP value.
DISCUSSION
Our study
found that an elevated NT-proBNP was associated with the AVR requirement in
asymptomatic patients with severe AS and preserved ventricular function after a
1-year follow-up. The biomarker had a very good discrimination capacity (AUC
0.88), and a value higher than 350 pg./mL was
associated with an increased AVR requirement higher than 50% (HR: 1.55). As
acknowledged, NT-proBNP and the active BNP hormone are released in response to
ventricular and/or atrial cardiomyocyte stretch, mainly as a result of
increased filling pressures. (13) Several studies have previously
evaluated the prognostic value of natriuretic peptides in AS. Recently, White
et al. (12) published a meta-analysis to assess
the prognostic role of several biomarkers in AS. They considered 33 studies
evaluating the NT-proBNP in 8597 patients. In the combined analysis, an
elevated NT-proBNP predicted mortality at follow-up (HR 1.73). All studies
included both asymptomatic and symptomatic patients, as well as AVR and non-AVR
patients.
In addition,
several studies have shown that elevated BNP and NT-proBNP are associated with
symptoms and a higher V max in patients with severe AS and preserved function.
(14-16)
As regards AS
without symptoms, in 2014 Clavel et al. (11) published an
observational study of nearly 2000 patients with moderate or severe AS, 560 of
whom were asymptomatic at baseline. In this subgroup, an increased BNP was an
independent predictor of mortality at follow-up. BNP values ≥3 times the
reference value represented an adjusted risk of event nearly 4 times higher
than normal BNP. In this sense, a Spanish study including 237 asymptomatic
patients with moderate and severe AS evidenced that an increased NT-proBNP was
an independent predictor of events (AVR requirement, mortality) at follow-up. (17) Unlike our
study, they found a mild discrimination capacity (AUC 0.62). More recently,
Henri et al. evaluated the purpose of a serial BNP measurement to predict
events in asymptomatic patients with severe AS. (18) An annual 20
pg./mL increase in BNP was independently associated
with a growing number of events at 3-year follow-up. A retrospective study of
74 patients found that NT-proBNP and the interventricular septum thickness were
independent predictors of events (mortality and AVR requirement) at 4-year
follow-up. (19) Previously, Monin et al. (20) found that
BNP was associated with increased events and mortality in asymptomatic patients
with severe AS and an AUC 0.74. They proposed a risk score considering the BNP
value, the V max, and the female sex, leading to better event prediction. This
score was later validated by Farre et al., (17) using
NT-proBNP instead of BNP. Based on these observations, the latest guidelines
propose AVR as a Class IIA indication in patients with elevated natriuretic
peptides. (3)
In our
population, 23% of patients developed symptoms and required AVR during
follow-up. This rate of events is lower than the rate reported in previous
studies, where about half of the patients required AVR. The Spanish group (17) reported
that 110 out of 237 patients required AVR in a follow-up similar to ours. In
addition, they recorded a 12% mortality. This is
remarkable, since they included a group with moderate AS. Our population was a
little younger (69 versus 74 years old) and had a lower baseline NT-proBNP
level (110 versus 490 pg./mL). This may partly explain
the difference in events. Our patients were probably in an earlier stage of AS.
We also found
that the E/e´ ratio was an independent predictor of AVR, with a mild predictive
capacity (AUC 0.64). This is consistent with previous studies evaluating
diastolic dysfunction parameters in AS. Especially the left atrium area (LAA)
and the E/e´ ratio have been found to be independent markers of events in
severe asymptomatic AS. (21,22) In our
study, patients requiring AVR had a higher LAA than those who didn’t; however,
in the multivariate analysis, LAA lost independent predictive value, due to the
E/e´ ratio and NT-proBNP. Something similar happened with the tissue S wave,
which was significant in the univariate but not in the multivariate analysis.
The V max is another parameter associated with worse AS progress. V max >5
m/sec indicates a very severe AS, and AVR is recommended in the absence of
symptoms. (2,3) We have not
found an association with the primary endpoint, probably because the average V
max was 4.2 m/sec, and very few patients had a V max >5 m/sec.
The natural
progress of severe AS and the time when AVR should be indicated while the
disease is asymptomatic, is being increasingly
discussed. The recommendation in the absence of adverse prognosis features is
careful surveillance and immediate intervention as soon as symptoms occur. (2-4) The basis for this consensus is that the benefit of avoiding
sudden death (1% per year in asymptomatic AS) may not be higher than AVR mortality.
However, a recent retrospective study compared progress in patients with
asymptomatic AS under a conservative treatment against a group of patients who
had received AVR. Asymptomatic patients with no AVR at the beginning had higher
mortality at 5-year follow-up than AVR patients. (23) Recently,
the results of the RECOVERY study were published; (24) this study
randomly assigned 145 asymptomatic patients with severe AS to early AVR versus
a conservative treatment. The early AVR group had reduced events (death at
surgery or within 30 days after surgery, or cardiovascular death during
follow-up) versus the conservative treatment (1% vs. 15%, HR 0.09 and a large
95% CI, 0.01-0.67). However, this population was carefully picked, relatively
young (aged 64), predominantly had a bicuspid etiology,
and an average V max of 5.1 m/sec. Several randomized studies are currently
being conducted to evaluate the early AVR strategy for asymptomatic AS: EARLY
TAVR (NCT03042104), EASY-AS (NCT04204915), EVOLVED (NCT03094143) (clinicalstrials.gob).
As we have said, the value of natriuretic peptides
increases with higher filling pressures. The increase in these and other
biomarkers may serve to identify a subgroup of patients who, even if they are
asymptomatic, are not so well adjusted to a higher afterload caused by AS, and
therefore, have worse progress. This subgroup could benefit from early
intervention. (25,26) In this sense, the study by
Nakatsuma et al. (27) included 380 asymptomatic patients
with severe AS and ventricular function that were divided based on their
baseline BNP levels. The rate of events in the group with BNP <100 pg/mL was
low both after a year and after 3 years (2.1% and 6.2 %, respectively), while
in the group with BNP >300 pg./mL, the rate of
events was considerably higher (22% and 42% after 1 and 3 years, respectively).
The results of our study contribute to the hypothesis that natriuretic peptides
may be a major factor when making decisions about asymptomatic patients with
severe AS and preserved function.
Limitations
Our study has
several limitations. It is a single-site study, so it is difficult to
extrapolate results to other populations. Follow-up was relatively short;
therefore, the impact of baseline NT-proBNP cannot be assessed in the long
term, and the discrimination capacity of events might be overestimated.
Nevertheless, one of the objectives was to evaluate factors helping to identify
patients with a higher risk that might benefit from early intervention. As a
result, we believe that a 36-month follow-up is sufficient for the study objectives.
Lastly, as this is an observational prospective study, the NT-proBNP value may
have affected the medical decision to perform an AVR, which may also help to
overestimate the event discrimination capacity of the biomarker.
CONCLUSIONS
At follow-up,
more than 20% of patients developed symptoms and required valvular replacement.
The NT-proBNP and E/e´ ratio were independent predictors of the AVR
requirement. The NT-proBNP had a very good discrimination
capacity, higher than the E/e’ ratio.
Conflicts of
interest
None
declared.
(See authors
conflicts of interest forms in the website/ Supplementary material)
1. Dweck MR, Boon NA, Newby DE. Calcific aortic stenosis: a disease
of the valve and the myocardium. J
Am Coll Cardiol 2012;60:1854- 63. https://doi.org/10.1016/10.1016/j.jacc.2012.02.093
2. Otto CM, Nishimura RA, Bonow RO,
Carabello BA, Erwin JP 3rd, Gentile F, et al. 2020 ACC/AHA Guideline for the
Management of Patients With Valvular Heart Disease: A Report of the American
College of Cardiology/American Heart Association Joint Committee on Clinical
Practice Guidelines. Circulation
2021;143:e72-e227. https://doi.org/10.1016/10.1161/CIR.0000000000000923
3. Vahanian A, Beyersdorf F, Praz F,
Milojevic M, Baldus S, Bauersachs J, et al. ESC/EACTS
Scientific Document Group. 2021 ESC/ EACTS Guidelines for the
management of valvular heart disease. Eur Heart J 2022;43:561-632.
https://doi.org/10.1016/10.1093/eurheartj/ehab395
4. Stutzbach P, Lax J, Ciancuilli T,
Granceli H, Piñeiro D, Prezioso D y cols. Sociedad
Argentina de Cardiología. Consenso de Valvulopatías. Rev Argent Cardiol.
2015;83(supl 2). Disponible en: https://www.sac.org.ar/wp-content/uploads/2015/06/consenso-valvulopatias-suplemento-2-2015.pdf
5. Ross J Jr, Braunwald E. Aortic
stenosis. Circulation 1968;38(1 Suppl):61-7. https://doi.org/10.1016/10.1161/01.cir.38.1s5.v-61
6. Bach DS, Cimino N, Deeb GM.
Unoperated patients with severe aortic stenosis. J Am Coll Cardiol 2007;50:2018-9. https://doi.org/10.1016/10.1016/j.jacc.2007.08.011
7. Kitai T, Honda S, Okada Y, Tani T,
Kim K, Kaji S et al. Clinical outcomes in non-surgically managed patients with
very severe versus severe aortic stenosis. Heart. 2011;97:2029-32. https://doi.org/10.1016/10.1136/heartjnl-2011-300137
8. Rosenhek R, Zilberszac R, Schemper
M, Czerny M, Mundigler G, Graf S, et al. Natural history of very severe aortic
stenosis. Circulation 2010;121(1):151-6. doi: 10.1161/CIRCULATIONAHA.109.894170.
9. Malaisrie SC, McCarthy PM, McGee
EC, Lee R, Rigolin VH, Davidson CJ et al. Contemporary perioperative results of
isolated aortic valve replacement for aortic stenosis. Ann Thorac Surg. 2010;89(3):751-6. doi:
10.1016/j.athoracsur.2009.11.024
10. Durko AP, Osnabrugge RL, Van
Mieghem NM, Milojevic M, Mylotte D, Nkomo VT, et al. Annual number of
candidates for transcatheter aortic valve implantation per country: current
estimates and future projections. Eur Heart J 2018;39:2635-42.
https://doi.org/10.1016/10.1093/eurheartj/ehy107
11. Clavel MA, Malouf J, Michelena
HI, Suri RM, Jaffe AS, Mahoney DW, et al. B-type natriuretic peptide clinical
activation in aortic stenosis: impact on long-term survival. J Am Coll
Cardiol. 2014;63(19):2016-25. https://doi.org/10.1016/10.1016/j. jacc.2014.02.581
12. White M, Baral R, Ryding A,
Tsampasian V, Ravindrarajah T, Garg P et al. Biomarkers Associated with
Mortality in Aortic Stenosis: A Systematic Review and Meta-Analysis. Med Sci (Basel) 2021;9:29. https://doi.org/10.1016/10.3390/medsci9020029
13. Steadman CD, Ray S, Ng LL, McCann
GP. Natriuretic peptides in common valvular heart disease.
J Am Coll Cardiol. 2010;55:2034- 48. https://doi.org/10.1016/j.jacc.2010.02.021
14. Gerber IL, Stewart RA, Legget ME,
West TM, French RL, Sutton TM, et al. Increased plasma natriuretic peptide
levels reflect symptom onset in aortic stenosis. Circulation.
2003;107:1884-90. https://doi.org/10.1016/10.1161/01.CIR.0000060533.79248.0C
15. Bergler-Klein J, Klaar U, Heger
M, Rosenhek R, Mundigler G, Gabriel H, et al. Natriuretic peptides predict
symptom-free survival and postoperative outcome in severe aortic stenosis. Circulation. 2004;109:2302-8. https://doi.org/10.1161/01.CIR.0000126825.50903.18
16. Nessmith MG, Fukuta H, Brucks S,
Little WC. Usefulness of an elevated B-type natriuretic peptide in predicting
survival in patients with aortic stenosis treated without surgery. Am J Cardiol. 2005;96:1445-8. https://doi.org/10.1016/j.amjcard.2005.06.092
17.
Farré N, Gómez M, Molina L, Cladellas M, Blé M, Roqueta C, et al. Prognostic value of NT-proBNP and an
adapted monin score in patients with asymptomatic aortic stenosis. Rev Esp Cardiol (Engl Ed). 2014;67:52-7.
https://doi.org/10.1016/j.rec.2013.06.020
18. Henri C, Dulgheru R, Magne J,
Caballero L, Laaraibi S, Davin L, et al. Impact of Serial B-Type Natriuretic
Peptide Changes for Predicting Outcome in Asymptomatic Patients With Aortic
Stenosis. Can J Cardiol. 2016;32:183-9. https://doi.org/10.1016/j.cjca.2015.06.007
19.
Campos I, Pereira J, Salome N, Pereira VH, Oliveira C, Marques Pires C, et al. Asymptomatic severe aortic stenosis:
what is the current role of exercise stress test and NT-proBNP in patient risk
stratification, Eur Heart J CardiovasC Imag 2021;22(Supplement
1) https://doi.org/10.1093/ehjci/jeaa356.053
20. Monin JL, Lancellotti P, Monchi
M, Lim P, Weiss E, Piérard L, et al. Risk score for predicting outcome in
patients with asymptomatic aortic stenosis. Circulation.
2009;120:69-75. https://doi.org/10.1161/CIRCULATIONAHA.108.808857
21. Lancellotti P, Moonen M, Magne J,
O'Connor K, Cosyns B, Attena E, et al. Prognostic effect of long-axis left
ventricular dysfunction and B-type natriuretic peptide levels in asymptomatic
aortic stenosis. Am J Cardiol 2010;105:383-8. https://doi.org/10.1016/j.amjcard.2009.09.043
22. Lancellotti P, Donal E, Magne J,
Moonen M, O'Connor K, Daubert JC, et al. Risk stratification in asymptomatic
moderate to severe aortic stenosis: the importance of the valvular, arterial and
ventricular interplay. Heart 2010;96:1364-71. https://doi.org/10.1136/hrt.2009.190942
23. Kvaslerud AB, Santic K, Hussain
AI, Auensen A, Fiane A, Skulstad H, et al. Outcomes in asymptomatic, severe
aortic stenosis. PLoS One 2021;16:e0249610. https://doi.org/10.1371/journal. pone.0249610
24. Kang DH, Park SJ, Lee SA, Lee S,
Kim DH, Kim HK, et al. Early Surgery or Conservative Care for
Asymptomatic Aortic Stenosis. N Engl J Med. 2020;382:111-9.
https://doi.org/10.1056/NEJMoa1912846
25. Lindman BR, Dweck MR, Lancellotti
P, Généreux P, Piérard LA, O'Gara PT, et al. Management of Asymptomatic Severe
Aortic Stenosis: Evolving Concepts in Timing of Valve Replacement. JACC Cardiovasc Imaging 2020;13(2 Pt 1):481-93. https://doi.org/10.1016/j.
jcmg.2019.01.036
26.
Généreux P, Stone GW, O'Gara PT, Marquis-Gravel G, Redfors B, Giustino G, et
al. Natural
History, Diagnostic Approaches, and Therapeutic Strategies for Patients With Asymptomatic Severe Aortic Stenosis. J Am Coll Cardiol. 2016;67:2263-88. https://doi.org/10.1016/j.jacc.2016.02.057
27.
Nakatsuma K, Taniguchi T, Morimoto T, Shiomi H, Ando K, Kanamori N, et al. CURRENT AS Registry Investigators. B-type natriuretic
peptide in patients with asymptomatic severe aortic stenosis. Heart. 2019;105:384-90.
https://doi.org/10.1136/heartjnl-2018-313746