
INTRODUCTION
Argentina estimates approximately 45 000 sudden deaths annually, most of which occur in out-of-hospital settings.
Out-of-hospital cardiac arrest is one of the leading causes of cardiovascular death worldwide. Survival depends largely on early recognition of the event and prompt defibrillation when the initial rhythm is shockable. (1)
Ventricular fibrillation is one of the most common rhythms in witnessed cardiac arrests and can be reversed through early defibrillation. Various international guidelines recommend the implementation of public defibrillation programs in high-traffic areas, such as airports, transport stations, and shopping centers.
The Autonomous City of Buenos Aires subway system is one of the country’s main modes of urban transportation and, under normal operating conditions, handles between 300 and 400 million trips per year, making it a particularly important setting for the implementation of cardioprotection and public defibrillation strategies.
The availability of automated external defibrillators (AEDs) in these settings allows non-medical personnel to initiate treatment before emergency services arrive.
In 2017, our group published a study on sudden death in rugby clubs, demonstrating the benefits of early intervention for victims of sudden death through the implementation of cardiopulmonary resuscitation (CPR) programs and the use of AEDs. (2) Continuing along these lines, the Buenos Aires subway system implemented a cardiac protection program that included the installation of AEDs and staff training on their use.
In this context of high passenger traffic, the implementation of cardioprotection programs takes on special relevance.
The objective of this study was to describe the activations of the response system and the effective use of AEDs in this context.
METHODS
A descriptive observational study was conducted based on operational registries from the cardiac protection program implemented in the Buenos Aires subway system.
All events recorded between 2018 and 2024 in which system personnel responded to retrieve an AED in response to a clinical situation potentially consistent with cardiac arrest were included.
System activation was defined as any situation in which an AED was requested or retrieved.
For each activation, the following data were recorded:
-
whether or not the device was used
-
rhythm detected by the AED
-
availability of information on subsequent outcomes, whenever possible.
No additional interventions were performed, nor was the patients’ usual clinical management altered.
The cardiac protection program also included training of subway system and railway workshop operating personnel in basic CPR and the use of AEDs. Overall, approximately 600 employees received specific training in recognizing a cardiac arrest, activating the emergency system, initiating CPR, and using the AED.
The statistical analysis was limited to descriptive statistics.
RESULTS
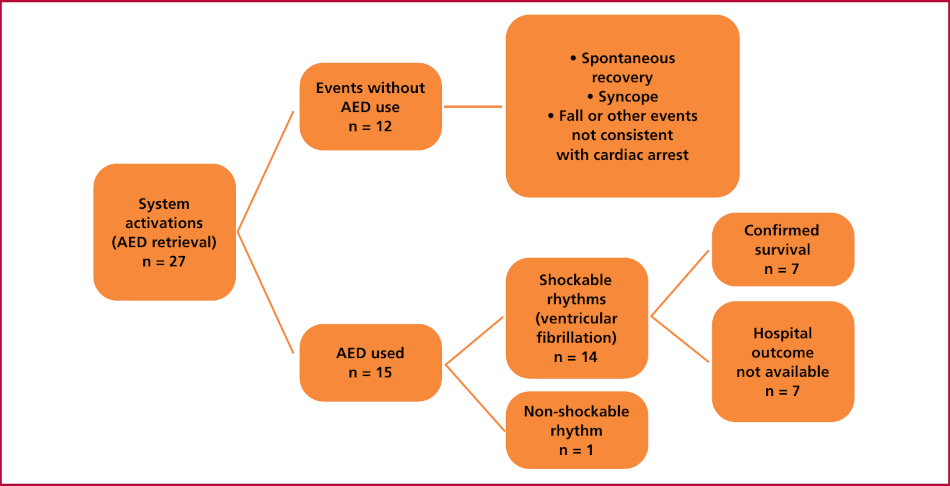
A total of 27 system activations were recorded, with 15 episodes of shockable rhythms treated (Table 1).
Of these activations:
-
15 cases (55.5%) required the use of the AED with electrode placement and rhythm analysis.
-
12 cases (44.5%) were resolved before the device was used, generally because the patient regained consciousness, exhibited spontaneous movements, or the event was due to syncope, a fall, or other situations not consistent with cardiac arrest.
Among the 15 patients evaluated using an AED, the rhythms detected were:
-
14 shockable rhythms (ventricular tachycardia (VT), or ventricular fibrillation (VF)
-
1 nonshockable rhythm.
Mean patient age was 53.3 ± 15.4 years, and 80% were male. Thirteen patients had ischemic heart disease. In all cases of ventricular fibrillation, the device indicated and delivered defibrillation following the device’s automatic algorithm.
Table 1
Patients treated with AED in the CABA subway system. Source: SAME intervention reports
| Patient | Gender | Age (years) | Type of arrhythmia recorded | Number of shocks | Hospital diagnosis |
|---|---|---|---|---|---|
| 1 | Female | 31 | Ventricular fibrillation | 1 | Brugada syndrome |
| 2 | Male | 58 | Ventricular fibrillation | 2 | Ischemic heart disease |
| 3 | Male | 66 | Ventricular tachycardia and ventricular fibrilla- tion | 1 | Ischemic heart disease |
| 4 | Male | 24 | Ventricular tachycardia and ventricular fibrilla- tion | 1 | Long QT syndrome |
| 5 | Male | 71 | Ventricular fibrillation | 3 | Ischemic heart disease |
| 6 | Male | 58 | Ventricular tachycardia and ventricular fibrilla- tion | 2 | Heart failure Ischemic heart disease |
| 7 | Female | 63 | Ventricular fibrillation | 2 | Ischemic heart disease |
| 8 | Male | 44 | Ventricular fibrillation | 2 | Ischemic heart disease |
| 9 | Male | 80 | Ventricular fibrillation | 2 | Ischemic heart disease with pacemaker |
| 10 | Male | 47 | Ventricular fibrillation | 1 | Ischemic heart disease and drug abuse |
| 11 | Female | 47 | Ventricular fibrillation | 1 | Multivessel ischemic heart disease |
| 12 | Male | 39 | Ventricular fibrillation | 2 | Ischemic heart disease and drug abuse |
| 13 | Male | 57 | Ventricular fibrillation | 2 | Multivessel ischemic heart disease with new PCR and pacemaker implantation |
| 14 | Male | 46 | Ventricular tachycardia | 3 | Ischemic heart disease |
| 15 | Male | 68 | Ventricular fibrillation | 1 | Ischemic heart disease |
Regarding subsequent outcomes, survival was confirmed in 7 patients. In 7 additional cases, it was not possible to obtain hospital information after transfer, so the final outcome could not be determined. (Figure 1)
Fig. 1
Results of the cardiac protection program in the Buenos Aires subway system between 2018 and 2024
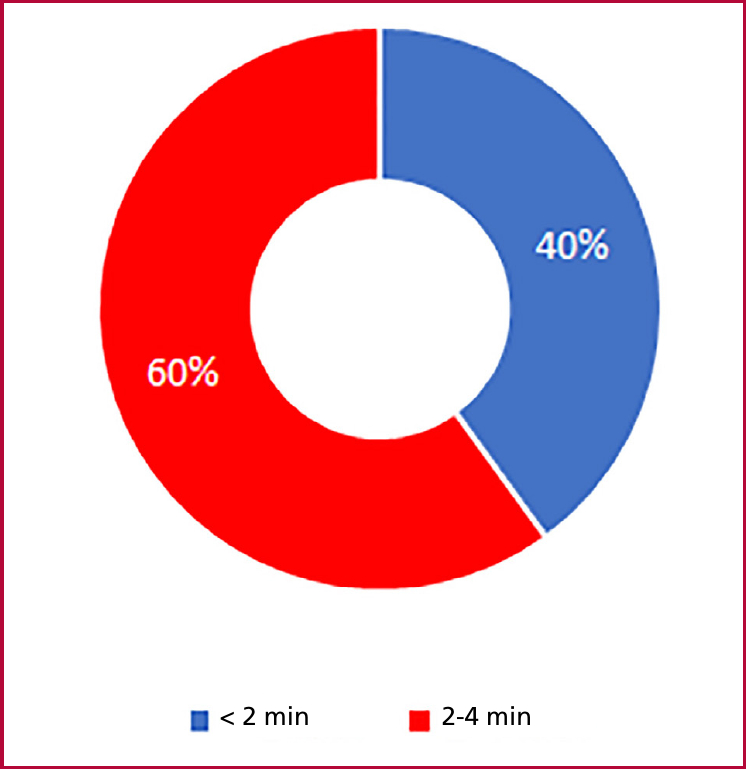
The time recorded until the first shock was less than 4 minutes in all cases and less than 2 minutes in 40%. (Figure 2) Subsequent hospital diagnoses primarily included ischemic heart disease and channelopathies. All initial interventions were performed by trained nonmedical personnel.
DISCUSSION
This study describes the experience of a cardioprotection program implemented in the Buenos Aires subway system, based on the availability of AEDs and staff training on their use.
More than half of the system’s activations resulted in the effective use of the AEDs suggesting that trained personnel was able to recognize situations potentially consistent with cardiac arrest and activate the corresponding protocol. All events were managed by nonmedical personnel trained through brief but systematic training programs. This had a direct impact on patient survival. (3)
Another notable finding was the high incidence of sudden cardiac death in men under 60 years of age. This pattern is consistent with regional data describing a higher prevalence of premature ischemic heart disease in Latin America, likely linked to a higher burden of poorly controlled classical risk factors. (4)
Moreover, a significant proportion of activations ultimately did not require the use of the device. This is consistent with international registries of public defibrillation programs, where situations such as syncope or transient loss of consciousness can initially mimic a cardiac arrest. (5)
Public defibrillation programs have shown favorable results in various hightraffic settings. (Table 2). At Chicago’s O’Hare Airport, one of the first structured public access defibrillator programs, a 56% survival rate was reported among patients treated with an AED following witnessed cardiac arrest. (6)
Tabla 2
Comparison between international public defibrillation programs and the experience of the cardiac protection program implemented in the Buenos Aires subway system
| Study | Setting | Cases analyzed | Shockable rhythms | Reported survival |
|---|---|---|---|---|
| Caffrey SL et al., NEJM 2002 (6) | O'Hare Airport, Chicago | 21 | Predominance of ventricular fibrillation | 56% |
| Hallstrom AP et al., NEJM 2004 (Public Access Defibrillation Trial) (7) | Public space in the U.S. | s 235 | Prevalence of ventricular fibrillation | Higher survival rate than CPR alone |
| Weisfeldt ML et al., Circulation 2011 (8) | U.S. OHCA Registry | >10 000 | Variable | Better in shockable rhythms |
| Present study | Buenos Aires Subway | 27 shocks | 14 cases of ventricular fibrilla- tion | Partial hospital follow-up |
CPR: cardiopulmonary resuscitation
CPR: cardiopulmonary resuscitation
Similarly, the Public Access Defibrillation Trial demonstrated that the availability of defibrillators in public spaces significantly increases survival rates compared with programs based solely on cardiopulmonary resuscitation. (7)
Furthermore, the Japanese experience in train stations has shown that survival rates can reach nearly 50% when the time to intervention is reduced to less than 3 minutes. In our case, the time recorded until the first shock was less than 4 minutes in all cases, and less than 2 minutes in 40% of cases. (9,10)
The experience observed in the Buenos Aires subway system aligns with this approach of public defibrillation strategies implemented in urban settings with high foot traffic.
Limitations
This study has several limitations.
The sample size is relatively small, and the analysis is limited to describing activations and device use.
In addition, complete hospital followup is not available for all patients, which prevents an accurate assessment of postevent clinical outcomes.
It was not possible to analyze neurological outcomes following cardiac arrest.
Finally, the period analyzed included the time corresponding to the COVID-19 pandemic, during which the use of public transportation experienced a marked reduction. During 2020, the number of subway passengers decreased significantly due to traffic restrictions and limited use of the system by essential workers, with a gradual recovery during 2021.
CONCLUSION
The implementation of a cardiac protection program in the Buenos Aires City subway system enabled registering multiple activations of the response system and the effective use of AEDs in a hightraffic public transportation setting.
These findings reinforce the importance of AED availability and staff training in public spaces as part of early response strategies for out-of-hospital cardiac arrest.
Such programs could be replicated in other urban transit systems in Latin America.