Lisandro Pérez Valega1, 2, Tomás Mullins2, 3, Luciana Olivera, Sebastián Caravagio
1Cardiology, Clínica Privada Monte Grande
2Canning Health Institute
3Coronary Care Unit, Clínica Privada Monte Grande
4Intensive Care Unit, Clínica Privada Monte Grande
Correspondence: Lisandro Pérez Valega. E-mail: lisandroperezvalega@gmail.com
Rev Argent Cardiol 2024;92:163-165. http://dx.doi.org/10.7775/rac.v92.i2.20764
Dengue is a viral disease caused by an arbovirus transmitted by arthropods, specifically by the bite of the female Aedes aegypti mosquito. It predominates in tropical and subtropical areas, and is one of the main public health problems in Central and South America. There are 4 serotypes of the virus: DEN-1, DEN-2, DEN-3 and DEN-4.
Most infections are benign or oligosymptomatic. Other cases may present with fever, headache, retro-ocular pain, myalgia, arthralgia and marked asthenia. Only on very few occasions are serious symptoms seen. This occurs when the patient had a previous infection with a serotype, and is reinfected with a different serotype. It is in these situations that the symptoms of dengue syndrome with shock, or hemorrhagic shock appear, presenting with thrombocytopenia, increased vascular permeability and in very few situations fulminant organ dysfunction (myocarditis or hepatitis).
In Argentina and countries in the region, especially Brazil, there is currently a dengue epidemic with alarming numbers of new infections. That is why we decided to present this clinical case, given the importance of this disease in endemic areas.
This is an 18-year-old patient, with no relevant pathological history, who reports starting on February 16 of this year with fever, general malaise and watery diarrhea without mucus, pus or blood. He progresses with marked asthenia in the following days, and on February 21 he adds mucous membranes and skin pallor, sweating, precordial pain and a presyncopal episode, so he is taken to the emergency room of a nearby hospital. Upon admission, they describe a patient frankly hypotensive, with blood pressure 60/40 mmHg, heart rate 60 bpm, temperature 38ºC, O2 saturation 99% at room air, and glucometer assessment 87 mg/dL. Figure 1 presents the admission ECG.
A few hours after being admitted to that institution he presents a sudden loss of consciousness with a tonic-clonic seizure. Electrocardiographic changes of Brugada type 1 syndrome are reported, which leads to request a referral to our clinic.
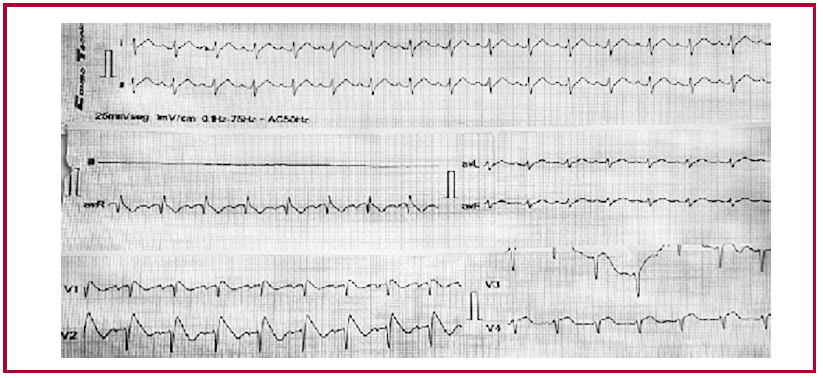
He is admitted to the coronary care unit with hypotension that does not improve with expansion with crystalloids, precordial pain and slowed capillary filling (greater than 3 seconds) with ECG evidencing a Brugada type 1 pattern, (Figure 2). Laboratory tests reveals ultrasensitive troponin T at 1532 pg./mL, CPK 1178 U/L; B peptide (BNP) 218 pg./mL; metabolic acidosis with pH 7.18, pCO2 58 mmHg, pO299 mmHg, bicarbonate 21 mEq/L, base excess 7.1 mmol/L, O2 saturation at room air 96%, lactic acid 9.3 mmol/L; hematocrit 55%, leukocytes 7260/mm3, platelets 131.000/mm3, blood glucose 167 mg/dL, urea 38 mg/dL, creatinine 1 mg/dL, KPTT 36 sec, prothrombin 47%, and SGOT 108 U/L. The rest of the hepatogram is normal.
The echocardiogram shows severe global hypokinesis, with left ventricular ejection fraction estimated at 10%, mild pericardial effusion without chamber collapse, and no evidence of valvular disease.
The condition is interpreted as cardiogenic shock in a young patient without previous diseases and a 5-day persistent fever. Our first suspicion is myocarditis of viral origin, so we request serologies for multiple viruses that can cause this entity. Infusion of noradrenaline and dobutamine is started with poor response, and mechanical ventilatory assistance is decided. Four hours after admission to the coronary care unit, the patient develops refractory hypotension and pulseless electrical activity, and despite advanced cardiopulmonary resuscitation maneuvers, he dies.
Five days after death, a positive dengue result is received, both for the NS1 antigen and the PCR for DEN-2.
We present a case of fulminant myocarditis due to dengue, with fatal outcome, in a young patient with no pathological history, who was admitted with a pre viously unknown Brugada type 1 pattern. There was no history of sudden death or diagnosis of this syndrome in the family. For all this, we considered that it could be an expression of Brugada type 1 pattern in the context of fever. We did not find in the literature any report of Brugada and dengue association.
In most cases, dengue is a self-limited disease and resolves in 5 to 7 days. However, a low percentage of patients experience the severe form, with cardiovascular impact evidenced by arrhythmias and myocarditis. (1)
According to Sud et al. the prevalence of myocarditis due to non-severe dengue without alarm symptoms is 9.7%, in non-severe dengue but with alarm symptoms it is 21%, and for severe dengue it is 46.6%. (2)
A meta-analysis of 12 studies and 2795 patients on the incidence of myocarditis in dengue defined it at around 21%. It should be noted that the patients were hospitalized, the mortality rate was low, and the sample was very heterogeneous. (3)
In another review carried out by the InterAmerican Society of Cardiology (NET-Heart Project) in 120 patients hospitalized for dengue in India, 12.5% had cardiovascular manifestations, the most frequent being bradyarrhythmias (6.6%), with sinus bradycardia as the most prevalent. In 3.3% of cases, echocardiography reported systolic dysfunction, 1.6% had pericardial effusion and 1% had atrial fibrillation. In this same review it was seen that between 3.3% and up to 24% of patients hospitalized for dengue may have changes on the echocardiogram that suggest myocarditis. (4)
An extensive review of the literature showed that up to 87% of dengue cases may have ECG changes (negative T waves, ST segment depression, T wave inversion, bundle branch blocks, etc.). It is interesting to note that the Brugada pattern is not described. (5) The appearance of Brugada pattern has traditionally been linked to febrile symptoms, but, we repeat, there is no description of its appearance in the context of dengue fever. (6)
Since we are going through a serious dengue epidemic, we consider it is very appropriate to know the cardiovascular damage caused by this virus. At the same time, we present a novel and extremely rare association of fulminant myocarditis due to dengue that presents with a Brugada type 1 ECG pattern. At no time did the patient present arrhythmias, and the arrest rhythm was not tachycardia or ventricular fibrillation, but rather pulseless electrical activity, so we do not believe that the Brugada pattern had a role in the fatal outcome.
Fig. 1 Admission ECG in the Hospital that referred the patient
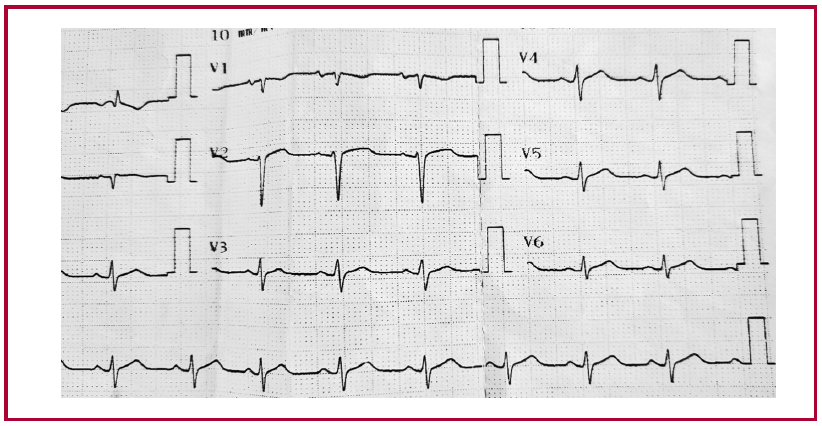
Fig. 2 ECG upon admission to our clinic showing Brugada type I pattern.
Ethical considerations
Not applicable.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Financing
None.
https://creativecommons.org/licenses/by-nc-sa/4.0/

©Revista Argentina de Cardiología
REFERENCES
- Khan MB, Yang ZS, Lin CY, Hsu MC, Urbina AN, Assavalapsakul W, et al. Dengue overview: An updated systemic review. J Infect Public Health 2023;16:1625-42. https://doi.org/10.1016/j.jiph.2023.08.001
- Sud R, Agarwal N, Aishwarya V, Aggarwal A, S Y, Kalawatia M, Sangoi R, et al. A Case Series of Dengue Myocarditis: A Complication Observed in Dengue Patients. Cureus 2023;15:e48285. https://doi.org/10.7759/cureus.48285
- Sandeep M, Padhi BK, Yella SST, Sruthi KG, Venkatesan RG, Krishna Sasanka KB, et al. Myocarditis manifestations in dengue cases: A systematic review and meta-analysis. J Infect Public Health 2023;16:1761-8. https://doi.org/10.1016/j.jiph.2023.08.005.
- Araiza-Garaygordobil D, García-Martínez CE, Burgos LM, Saldarriaga C, Liblik K, Mendoza I, et al. Neglected Tropical Diseases and other Infectious Diseases affecting the Heart (the NET-Heart) project. Dengue and the heart. Cardiovasc J Afr. 2023 32:276-283. https://doi.org/10.5830/CVJA-2021-033.
- Parchani A, Krishnan Vs G, Kumar VS. Electrocardiographic Changes in Dengue Fever: A Review of Literature. Int J Gen Med. 2021;14:5607-5614. https://doi.org10.2147/IJGM.S328755.
- Roomi SS, Ullah W, Abbas H, Abdullah H, Talib U, Figueredo V. Brugada syndrome unmasked by fever: a comprehensive review of literature. J Community Hosp Intern Med Perspect. 2020;10:224-28. https://doi.org/10.1080/20009666.2020./1767278.