
INTRODUCTION
Aortic valve stenosis (AS) is one of the most prevalent valvular heart diseases worldwide, with an even higher prevalence among elderly patients, which is associated with a high burden of comorbidities and a poor clinical prognosis if timely and early treatment is not provided. (1,2) In recent decades, transcatheter aortic valve implantation (TAVI) has established itself as one of the primary therapeutic strategies for patients with severe symptomatic AS, encompassing various age groups and surgical risk subgroups. (3-5) Its adoption has expanded steadily, supported by robust evidence demonstrating its efficacy and safety compared with conventional surgical valve replacement.
However, despite its growing implementation, substantial differences have been documented across different regions and healthcare systems in terms of access to the procedure, financing challenges, and delays between the therapeutic decision and the actual performance of the implantation. (6,7) In this context, it is particularly relevant for our region to analyze in detail the duration of the different stages of the process leading to TAVI, with the aim of identifying optimization opportunities that can improve system efficiency and clinical outcomes for patients.
The purpose of this study was to analyze care intervals between key stages of the diagnostic-therapeutic process and TAVI in the real-world clinical practice of three centers in Argentina, comparing two time periods defined by a turning point, with the aim of identifying potential improvements in organizational efficiency and care delivery.
OBJECTIVE
We conducted this study with the aim of correlating by echocardiography the trigones and the CF with topographic anatomy to understand the anatomo- functional characteristics of cardiac mechanics.
METHODS
A retrospective, observational, multicenter cohort study was conducted, including the analysis consecutive patients with severe AS who underwent TAVI during the period from January 2022 to August 2025.
Demographic (age, gender), care-related (center, health insurance coverage), procedural (type of implanted prosthesis, need for prior coronary revascularization or valvuloplasty, use of a pacemaker, transesophageal echocardiography and in-procedure events), and clinical (periprocedural clinical complications and mortality during the 30-day follow-up period) variables were collected.
The clinical time points of interest were defined prospectively and analyzed as intervals in days between:
• First contact (FC) with the interventional cardiologist à implantation.
• Computed tomography (CT) à implantation.
• Valve request à implantation. These metrics reflect the diagnostic and administrative sequence of the pre-TAVI process, in line with the characterization of “waiting times” used in international studies. (7)
Statistical analysis
Continuous variables were expressed as mean and standard deviation (SD) or median and interquartile range (IQR) according to their distribution characteristics. The normality of the variables was assessed by graphical inspection and the Shapiro–Wilk test. Categorical variables were presented as absolute frequencies and percentages.For the comparative analysis of care intervals, two periods were defined based on the cutoff date of November 1, 2024, corresponding to an institutional reorganization of the medical-administrative care pathways at the participating centers.
Differences between periods were assessed using Welch’s t-test for independent means, given the possible heterogeneity of variances between groups. In cases of non-normal distributions, the robustness of the results was verified using the nonparametric Mann–Whitney U test.
The data were analyzed using an exploratory approach with no corrections for multiple comparisons. All comparisons were two-sided, and a p-value <0.05 was considered statistically significant. Statistical analysis was performed using standard statistical software for biomedical research (Stata®, version BE, StataCorp, College Station, TX, USA).
Ethical considerations
The study was conducted in accordance with the principles of the Declaration of Helsinki, (8) and was approved by the institutional ethics committees of the participating centers. The individual informed consent was waived given the retrospective nature of the study and the use of anonymized data.
RESULTS
Dissection and topographic anatomy of the cardiac fulcrum
A total of 71 patients who underwent TAVI between January 2022 and August 2025 were included in the analysis. Mean age of the study population was 80.9 ± 5.2 years, with female predominance . In terms of the procedure’s financiers, health coverage was provided primarily by the Comprehensive Medical Care Program (PAMI), while the Institute of Medical Assistance (IOMA) accounted for only a minority of cases, approximately 1%. (Table 1)
Table 1
Baseline characteristics of the study population
| Variable | n=71 |
|---|---|
| Age, years | 80.9 ± 5.2 |
| Male gender | 44 (62.4) |
| BMI, kg/m² | 26.8 ± 3.4 |
| Hypertension | 59 (83.3) |
| Dyslipidemia | 37 (52.6) |
| Diabetes mellitus | 23 (32.1) |
| Smoking | 11 (15.9) |
| Chronic kidney disease | 9 (13.3) |
| Peripheral vascular disease | 8 (11.7) |
| Atrial fibrillation | 16 (23.2) |
| Cancer | 6 (8.1) |
| COPD | 10 (14.7) |
| Previous pacemaker | 2 (3.1) |
| LVEF, % | 57 ± 9 |
| Financier | |
| PAMI | 70 (98.6) |
| IOMA | 1 (1.4) |
| Other | 0 (0) |
* Data expressed as mean ± standard deviation or absolute value (percentage)BMI: body mass index; COPD: chronic obstructive pulmonary disease; IOMA: Institute of Medical Assistance; LVEF: left ventricular ejection fraction; PAMI: National Institute of Social Services for Retirees and Pensioners
Regarding the technologies used for TAVI, the most commonly implanted valve prostheses were Evolut R/PRO (Medtronic Inc., Minneapolis, MN, USA), followed by Sapien 3 (Edwards Lifesciences LLC, Irvine, CA, USA), ACURATE neo2 (Boston Scientific Corporation, Marlborough, MA, USA), and Myval (Meril Life Sciences Pvt. Ltd., Vapi, Gujarat, India), respectively. (Table 2)
Table 2
Type of implanted valve prosthesis and periprocedural adverse clinical events
| Variable | n=71 |
|---|---|
| Type of prosthesis implanted | |
| Evolut R/PRO | 51 (71.8) |
| Sapien 3 | 17 (23.9) |
| ACURATE neo2 | 2 (2.8) |
| Myval | 1 (1.4) |
| Pre-TAVI PCI | 18 (25.3) |
| Aortic balloon valvuloplasty | 3 (2.8) |
| Permanent pacemaker implantation | 3 (4.2) |
| Intraprocedural adverse clinical events | 3 (4.2) |
| Immediate post-implantation events (before discharge) | 5 (7.0) |
| Mid-term post-discharge events | 2 (2.8) |
| Overall 30-day mortality | 3 (4.2) |
* Data expressed as absolute values (percentage). PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation
No valve requests were rejected by the financiers, although in some cases, the amount of supporting documentation required for device provision was greater than for the rest of the patients.
Preoperative evaluation was complete in all patients, including electrocardiogram, transthoracic echocardiogram, coronary angiography, CT scan with TAVI protocol, and conventional surgical risk scores.
Procedures and adverse clinical events
Regarding the cardiovascular interventional procedures performed during pre-TAVI preparation, onequarter of patients required percutaneous coronary intervention (PCI) prior to TAVI, while approximately 3% underwent balloon aortic valvuloplasty (BAV) as a bridge to the intended therapeutic procedure. Among the total number of patients included, only two had a history of permanent pacemaker implantation, while three required a permanent pacemaker postimplantation.
Intraprocedural adverse clinical events were recorded in only three patients: two required emergency pacemaker implantation, and one developed congestive heart failure. In the immediate postimplantation period, complications were observed in five patients: one emergency pacemaker, one vascular access complication, two deaths, and one case of acute cholecystitis unrelated to TAVI. In the mid term, two patients experienced clinical events (one case of congestive heart failure and one case of infectious endocarditis of a native valve with a fatal outcome). An overall mortality rate of 4.2% was observed during the 30-day followup period following the index procedure.
Analysis of care intervals
Analysis of delays in each of the care intervals showed that the median time between the FC with an interventional cardiologist and TAVI was 165 days (IQR 118–258); the median interval between CT and implantation was 145 days (IQR 98–216), and the median time from valve request to implantation was 67 days (IQR 45–112).
When comparing the periods defined by the cutoff date of November 1, 2024—corresponding to an institutional reorganization of medical and administrative workflows—a significant reduction was observed in all three intervals analyzed. Among the specific measures implemented as part of this reorganization, the following stand out: the designation of a fixed weekly day dedicated exclusively to TAVI ; the creation of a stable and dedicated team, always composed of the same physicians, technicians, and nurses from the hemodynamic department; the appointment of a single person responsible for the structural management of the program, avoiding the rotation of responsibilities among different professionals; the personalization of followup for each patient through direct communication via WhatsApp with the head of the structural pathology team; and, the systematic learning of the administrative processes of the financiers, in order to understand their internal logic and optimize the management of authorization requests.
Thus, prior to the preestablished turning point, the medians were 338 days (IQR 220–512) for the FC–implantation interval, 320 days (IQR 185–455) for CT scanimplantation, and 131 days (IQR 78–205) for requestimplantation.
In contrast, in the subsequent period, these were reduced to 138 days (IQR 110–180), 117 days (IQR 88–165), and 56 days (IQR 39–82), respectively, showing a statistically significant difference in all cases (p <0.001 for all three intervals). (1)
DISCUSSION
To the best of our knowledge, this study constitutes the first multicenter analysis conducted in Argentina that systematically evaluates care intervals in the diagnostictherapeutic process prior to TAVI in the Argentine healthcare system. Our findings show that delays between the different stages of the care circuit are considerable and that, following the implementation of an institutional reorganization of administrative and clinical workflows, a significant and sustained reduction in times to the procedure was achieved.
These results are consistent with international reports indicating that prolonged waiting times between the therapeutic decision and implantation constitute a growing challenge in realworld TAVI practice, particularly in healthcare systems with coverage limitations or partial government funding. (7-9) Recent
studies have shown that socioeconomic and structural factors within healthcare systems directly influence access to and timing of the procedure, leading to inequalities across regions and types of coverage. (10-13) In this regard, data from our cohort confirm that logistical and administrative barriers can be a major determinant of delays, even in settings with established experience in structural intervention.
The marked decrease observed in the FC–implantation, CT–implantation, and valve requestimplantation intervals following institutional reorganization suggests that optimizing internal processes can have an immediate impact on the efficiency of care. In particular, closer coordination between clinical and administrative and financing teams (primarily PAMI and IOMA) allowed for a significant shortening of the authorization, provision, and scheduling stages of the procedure. This finding underscores the importance of integrated healthcare management strategies, which do not necessarily require additional technological investments, but rather an improvement in interinstitutional coordination and the definition of operational responsibilities. (14)
This set of lowcost, highly effective strategies demonstrates that institutional reorganization focused on people and processes can have the same or even greater impact than the incorporation of new technologies.
Furthermore, the study provides valuable information concerning the reality of access to TAVI in the Argentine healthcare area, where reliance on state coverage mechanisms and administrative bureaucracy often dictates the timing of therapeutic resolution. In this context, identifying the critical points in the process—from the initial indication to the actual availability of the valve prosthesis—can guide health policies aimed at accelerating equitable access to highly complex therapies.
Fig. 1. Analysis of prespecified time intervals prior to TAVI, and differences relative to the inflection point
Figura 1
Analysis of prespecified time intervals prior to TAVI, and differences relative to the inflection point
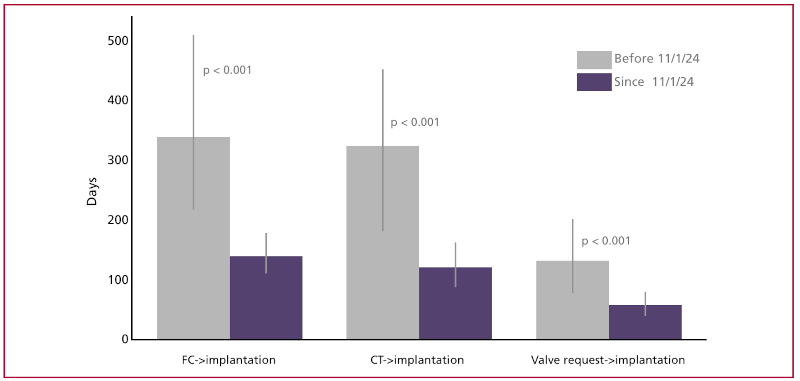
FC: first contact with interventional cardiologist, CT: computed tomography
Data expressed as median (interquartile range)
The process from the therapeutic decision to the actual implantation involves multiple stages of high administrative complexity, which often results in prolonged delays. In this regard, it has been demonstrated that the presence of a coordinator to lead the TAVI program at the institutional level can be associated with greater organizational efficiency, a significant reduction in care times, and better patient satisfaction indicators, who would also potentially benefit from more structured followup during the postprocedurural period. (15)
Although the present work did not aim to assess the clinical impact of delays in care at different stages of the process, several studies have suggested that prolonged waiting times may be associated with increased morbidity and mortality, both due to the progression of AS and to the decompensation of comorbidities during the preprocedurural period. (16) Within the analyzed cohort, five patients with severe AS who had initiated the evaluation process for TAVI experienced adverse events during the delay period: one suffered a disabling stroke, two died from cardiovascular causes, and two discontinued the administrative process before its completion. For this reason, the reduction in waiting times observed in our cohort could have favorable clinical implications, which deserve further exploration in future prospective studies. It is worth noting that in the analyzed cohort, the use of BAV as a bridging strategy to TAVI was recorded in a minority of cases. Its implementation in some of these patients was a direct consequence of prolonged administrative delays, which in itself constitutes a limitation of the system, considering that BAV entails known procedural risks and offers only a temporary clinical benefit; therefore, its use as a bridge forced by avoidable delays is inappropriate and should be described as a manifestation of the healthcare system dysfunction. Internationally, its indication is restricted to specific clinical situations and is not a standard practice in response to administrative delays. (17-20)
The causes that could explain these observed delays are multifactorial. These include referrals arriving with incomplete or insufficient diagnostic studies for therapeutic decisionmaking, delays in scheduling outpatient appointments and obtaining administrative authorizations, frail patients’ dependence on caregivers, as well as socioeconomic and logistical barriers related to transportation and geographic distances. Moreover, holdups within the facility—common in units not exclusively dedicated to TAVI—are exacerbated by limited resource availability, such as a single angiography machine, and by the need to coordinate the simultaneous presence of anesthesiology and vascular surgery teams to perform the procedure.
Finally, the findings presented here reinforce the need to develop specific quality indicators for the pre-TAVI process, to allow for continuous monitoring of access times and facilitate comparisons between institutions. The incorporation of these indicators into national or regional TAVI registries could serve as a key tool for promoting efficiency, equity, and transparency in access to this treatment within the Argentine and Latin American healthcare systems.
Limitations
This study has a number of limitations, which must be taken into account when interpreting the results. First, this is a retrospective cohort analysis based on a relatively small sample limited to three healthcare centers in the Buenos Aires Metropolitan Area, which might limit the extrapolation of the findings to other institutional settings or regions of the country with different healthcare infrastructure.
Second, all patients included were from public and social medicine healthcare centers, with coverage primarily provided by PAMI (National Institute of Social Services for Retirees and Pensioners) and IOMA (Institute of Medical Assistance). The population characteristic constitutes a significant limitation for generalizing the findings: the care timelines described reflect the specific dynamics of these financing institutions, whose administrative bureaucracy and documentation requirements for authorizing and providing the device differ substantially from those of private or prepaid health insurance. In Argentina, it is likely that in centers with predominantly private coverage, the intervals between the therapeutic decision and the implantation are significantly shorter, given that approval processes tend to be more streamlined and less documentintensive. On the other hand, while the predominance of PAMI in the cohort accurately reflects the epidemiological reality of severe AS in Argentina -a disease prevalent among older adults with statefunded coverage- it would be desirable to compare these results with data from centers with a greater diversity of coverage schemes, in order to more precisely determine the relative weight of administrative factors dependent on the financier versus institutional factors specific to each center.
Finally, the study was not designed to evaluate the direct clinical impact of care delays on post-TAVI outcomes, so the findings should be interpreted primarily as an organizational and efficiency assessment of the system rather than as an analysis of adverse clinical outcomes.
Despite these limitations, the present study provides novel and representative information on realworld clinical practice in the Argentine healthcare system, identifying concrete opportunities for improvement in the management of the preprocedural process.
CONCLUSION
This observational study of patients from our region demonstrated that pre-TAVI care times exhibit notable variability, with significant delays between the different stages of the process. The implementation of an institutional reorganization of care pathways, established in November 2024, was associated with a substantial and statistically significant reduction in the three intervals analyzed, suggesting a progressive improvement in the operational and administrative efficiency of the participating centers.