Mirza Rivero1 MTSAC, Mauro Gingins2, Valentín Roel3 MTSAC, Fabricio G. Procopio4, Ricardo A. Villarreal5 MTSAC, Rosina Arbucci6 MTSAC, Guillermo Pérez7, Juan P. Costabel8 MTSAC (En representación de los investigadores del registro RESCAR)
1 CEMIC
2 Hospital Británico de Buenos Aires
3 Hospital Durand
4 Fundación Favaloro
5 Sanatorio Güemes
6 Consejo de Emergencias Cardiovasculares y Cardiología Crítica "Dr. Rafael Bullrich" . Sociedad Argentina de Cardiología
7 Hospital Naval
8 ICBA
Address for reprints: Mirza Rivero. Galván 4102, 1er piso, Unidad Coronaria. Ciudad de Buenos Aires. CP 1430. Mail: mirzavrivero@gmail.com
Rev Argent Car diol 2024;92:108-116. http://dx.doi.org/10.7775/rac.v92.i2.20746
SEE RELATED ARTICLE : Rev Argent Car diol 2024;92:97-98. http://dx.doi.org/10.7775/rac.v92.i2.20750
ABSTRACT
Background: Myocardial infarction with non-obstructive coronary arteries (MINOCA) is a well-known condition that has been recently redefined after excluding non-ischemic myocardial injury. ReSCAR was a prospective, multicenter registry of patients hospitalized for acute coronary syndrome (ACS) from January to August 2022.
Objective: One of the main objectives of the registry was to define the prevalence of patients with MINOCA, their baseline clinical and paraclinical characteristics, and in-hospital outcome. This publication focuses on the results of the respective analysis.
Methods: We conducted a nationwide, multicenter, prospective study of patients with ACS. The diagnosis of MINOCA was made following the Fourth Universal Definition of Myocardial Infarction. The baseline characteristics of the patients wereanalyzed, as well as their outcome and significant differences with patients with obstructive coronary artery disease. The participating centers should have the availability to measure high-sensitivity cardiac troponin and perform coronary angiography.
Results: A total of 984 patients from 15 centers were included. Eighty-five patients (8.6%) had a final diagnosis of MINOCA at discharge. Median age was 65 years (53-63), 48 (51.8%) were women, 55 (64.7%) had hypertension, 44 (51.8%) had dyslipidemia, 9 (10.6%) were diabetics and 23 (27.1%) were smokers. Median high-sensitivity cardiac troponins on admission (expressed as multiples of the 99th percentile) were 2.42 times higher (0.85-10.21) and the ECG had no ischemic changes in 71.8% of the patients. Coronary angiography was normal in 72.9% of the patients and the rest of the cases had coronary artery stenoses < 50%. Sixteen patients underwent cardiac magnetic resonance imaging. The median GRACE score was 115 (98-139), which corresponds to intermediate risk. The event rate for the composite outcome of stroke/myocardial infarction or death was1.2%, and there were no bleeding events BARC ≥type 2. The discharge prescription rate was 72.9% for aspirin, 27.1% for clopidogrel, 88.2% for statins, 67.1% for beta-blockers, and 22.4% for calcium channel blockers.
In this registry, patients with MINOCA represent a significant proportion of those with ACS.
Conclusion: The rate of in-hospital complications, including mortality, was low. There seems to be a strong opportunity for further investigations to confirm the diagnosis, pathophysiological mechanisms, and treatment of MINOCA.
Key words: MINOCA - Myocardial Infarction with Non-obstructive Coronary Arteries - Acute Coronary Syndrome - Registry - Coronary Artery Disease
RESUMEN
Introducción: El infarto de miocardio sin obstrucciones coronarias significativas (MINOCA) es una conocida entidad que se ha redefinido recientemente al excluir la injuria miocárdica no isquémica. ReSCAR fue un registro prospectivo, multicéntrico de pacientes hospitalizados por síndrome coronario agudo (SCA) desde enero hasta agosto de 2022.
Objetivo: Un objetivo principal del registro fue definir la prevalencia de pacientes con MINOCA, sus características basales clínicas y paraclínicas y evolución intrahospitalaria. Los resultados del análisis respectivo son la base de esta publicación.
Material y métodos: Registro nacional prospectivo y multicéntrico de SCA. Diagnóstico de MINOCA de acuerdo con la Cuarta Definición Universal de Infarto de Miocardio. Análisis de las características basales, evolución y diferencias significativas respecto de los pacientes con coronariopatía obstructiva. Los centros participantes debían contar con determinación de troponina de alta sensibilidad y la posibilidad de realizar cinecoronariografía.
Resultados: Se incluyeron 984 pacientes de 15 centros. Ochenta y cinco pacientes (8,6 %) tuvieron diagnóstico final de MINOCA al alta. Cuarenta y cuatro pacientes (51,8 %) eran mujeres, la mediana de edad fue de 65 años (53-63), 55 (64,7 %) pacientes eran hipertensos, 44 (51,8 %) dislipidémicos, 9 (10,6 %) diabéticos y 23 (27,1 %) fumadores. La mediana de troponina al ingreso (expresada como múltiplo del percentilo 99) fue de 2,42 (0,85-10,21) y el 71,8 % se presentó con un ECG sin cambios isquémicos. La angiografía coronaria fue normal en el 72,9 % de los pacientes y con lesiones menores de 50 % en el resto. Se realizó resonancia cardíaca a 16 pacientes. La mediana del score GRACE fue de 115 puntos (98-139), lo cual perfila un riesgo intermedio; con una tasa de eventos combinados de accidente cerebrovascular/infarto o muerte de 1,2 %, sin haberse registrado sangrados BARC 2 o más. La prescripción al alta de aspirina fue del 72,9 %, clopidogrel 27,1 %, estatinas 88,2 %, beta bloqueantes 67,1 % y antagonistas cálcicos 22,4 %.
Conclusión: En este registro, los pacientes con MINOCA representan una proporción significativa de aquellos con SCA. La tasa de complicaciones intrahospitalarias, incluida la mortalidad, fue baja. Impresiona existir una fuerte oportunidad para profundizar los estudios para confirmar este diagnóstico, sus mecanismos fisiopatológicos y su tratamiento.
Palabras clave: MINOCA - Infarto de miocardio sin lesiones coronarias - Síndrome coronario agudo - Registro - Enfermedad coronaria
Received: 12/15/2023
Accepted: 01/27/2024
INTRODUCTION
Myocardial infarction with non-obstructive coronary arteries (MINOCA) is defined as a condition suggestive of myocardial infarction in the absence of obstructive coronary arteries on angiography (angiographically normal coronary arteries or coronary artery stenosis < 50%). This entity has gained renewed interest in recent years based on studies aimed at clarifying its pathophysiology and differentiating it from other causes of non-ischemic myocardial injury such as Takotsubo cardiomyopathy and myocarditis. (1) The diagnosis is often suspected during hospitalization and is confirmed later or not. Cardiology societies worldwide have agreed to use the term MINOCA to describe a working diagnosis for ischemic cardiomyopathy which encompasses various causes, including plaque rupture, coronary artery spasm, coronary embolism, spontaneous coronary artery dissection, and microvascular dysfunction. ((2)-5) The optimal treatment and prognosis for these patients are still uncertain.
Many studies that describe the characteristics of MINOCA are based on retrospective data and do not differentiate its diagnosis from other causes of non-ischemic myocardial injury. Therefore, the conclusions drawn from these studies may be erroneous. (6-8)
The aim of this study was to describe the characteristics and in-hospital outcome of MINOCA patients in high-complexity centers of Argentina.
METHODS
ReSCAR was a prospective cohort study conducted in high complexity medical centers in Argentina, mostly located in Buenos Aires metropolitan area. The study was conceived, designed and conducted by the Council on Cardiovascular Emergency Care of the Argentine Society of Cardiology to describe the spectrum of acute coronary syndromes (ACS), particularly the in-hospital features and one-year outcome. The protocol was designed with a focus on including variables for describing MINOCA.
The participating centers should have the availability to measure high-sensitivity cardiac troponins and perform coronary angiography in order to standardize the diagnosis of myocardial infarction according to the current criterion. (5)(5) The Argentine Society of Cardiology invited all centers in Argentina to participate in the study.
Diagnosis of MINOCA
The diagnosis of MINOCA was assigned by the principal investigator of the center when the patient was discharged. The definition used was the one suggested by the Fourth Universal Definition of Myocardial Infarction which is currently shared by the Consensus Statement of the Argentine Society of Cardiology. (4,5)
MINOCA was considered a clinical-angiographic syndrome characterized by:
- A rise and/or fall of high-sensitivity cardiac troponin values with at least one value above the 99th percentile upper reference limit and at least one of the following: symptoms of myocardial ischemia, new significant electrocardiographic changes, development of pathological Q waves, evidence of loss of viable myocardium or regional wall motion abnormality in imaging tests, or identification of intracoronary thrombus by angiography or autopsy.
- Non-obstructive coronary artery disease: defined as absence of coronary artery stenosis ≥ 50%.
- Absence of alternative diagnoses of myocardial injury (sepsis, pulmonary embolism, aortic dissection, etc.).
Sample size estimation
Given that previous registries have reported a prevalence of around 10% for MINOCA, (6910) we planned to include 1000 ACS patients from January to August 2022. This would allow us to obtain approximately 100 patients with MINOCA for the analysis and comparison with other coronary syndromes.
Inclusion criteria
We included consecutive patients > 18 years of age who were admitted to the coronary care unit for an acute coronary syndrome (ACS) and a final diagnosis at discharge of ST-segment elevation myocardial infarction, non-ST-segment elevation myocardial infarction, unstable angina, type 2 myocardial infarction, or MINOCA. Patients with a diagnosis of ACS on admission and final diagnosis of myocarditis of Takotsubo were also included.
Data collection
Data were collected from the information recorded in an electronic case report form in the RedCap platform. (11) Access to the data was controlled by the group that organized the registry to ensure confidentiality.
The collected data included the patient's medical history, clinical information upon admission, laboratory tests, electrocardiogram, coronary angiography, and other tests conducted during hospitalization. In-hospital complications and medications on admission and discharge were recorded. For data analysis, high-sensitivity cardiac troponins (T and I) are expressed as multiples of the 99th percentile (99px) to separate the values of the different cut-off points for each center and make them comparable. Analysis of the data corresponding to the pre-specified 12-month follow-up period is ongoing and was collected through telephone contact and medical records. For further information on the protocol, please refer to the already published ReSCAR registry. (12)
Statistical analysis
All the statistical calculations were performed using IBM SPSS 25.0 software package. Discrete variables were expressed as frequencies and percentages. Continuous variables were expressed as mean ± standard deviation, or median and interquartile range, according to their distribution. The chi square test or Fisher's exact test were used to compare the categorical variables, and continuous variables were analyzed using the Student's t test or the Mann- Whitney test according to their distribution. A type I error < 5% (two-tailed p value < 0.05) was considered statistically significant.
Ethical considerations
All the patients gave their informed consent before participating in the study. The consent was submitted for approval by the institutional review board of each center, which is under the regulations of the Central Review Board of the Argentine Society of Cardiology.
The investigators implemented measures to protect the confidentiality of all the information according to the Argentine Law on Protection of Personal Data No. 25326, so that the identity of the patients and all their personal data will remain anonymous and only the researchers and the members of the learning, teaching and research ethics committee would have access to these data, if required.
The study was conducted following national ethical standards (Law No. 3301 of the city of Buenos Aires, National Law for Good Clinical Practice in Research on Human Subjects, and the Declaration of Helsinki, among others).
RESULTS
A total of 984 patients from 15 centers were included between January and August 2022. Of the 104 patients (10.6%) without significant coronary artery stenoses, 85 (8.6%) had a final diagnosis of MINOCA.
Median age of MINOCA patients was 65 years (53- 73) and 51.8% were women. The general characteristics of MINOCA patients are displayed in Table 1. Among coronary risk factors, 55 patients had hypertension (64.7%), 9 patients had diabetes (10.6%), 44 had dyslipidemia (51.8%), 23 were current smokers (27.1%), and 7 had a family history of cardiovascular disease (8.2%). Regarding women-specific risk factors (n= 43), 1 patient had a history of gestational diabetes (2.3%), 1 had a hypertensive disorder of pregnancy (2.3%), and median age of menopause was 52 years (48-55). Active or recent cancer was the most common comorbidity and was present in 5 patients (5.9%), while 4 patients had chronic kidney disease (4.7%). Almost a quarter (23.5%) of the patients had a history of coronary artery disease, which was associated with the presence of coronary artery stenoses <50% on coronary angiography. Ten patients had a history of myocardial infarction (11.8%) and 9 patients had undergone percutaneous coronary intervention (9.5%). Eight patients had a history of atrial fibrillation (9.4%) and 3 had heart failure (3.5%). Compared to patients with myocardial infarction and significant coronary artery obstructions, patients with MINOCA had a higher proportion of female gender (51.8% vs. 20.4%, p < 0.001), and lower prevalence of diabetes (10.6% vs. 26.8%, p<0.001), tobacco use (27.1% vs. 47.3%, p = 0.012) and previous myocardial infarction (11.8% vs. 24.7%, p = 0.006), but a a trend to higher prevalence of chronic angina (8.2 vs. 3.8%, p = 0.084).
On admission, 95.3% of the patients were hemodynamically stable and without heart failure. There were no ischemic changes in the electrocardiogram in 71.8% of the cases. Among abnormal electrocardiograms, T-wave changes were the most common (12.9%), followed by ST-segment depression (8.2%), and only 2.4% presented with ST-segment elevation. Median high-sensitivity cardiac troponin levels on admission were 2.42 times above the 99th percentile of the reference values (0.85-10.21). Median left ventricular ejection fraction was 60% (55-64%). Median GRACE score was 115 (98-138) and median CRUSADE score was 23 (14-31). Compared to patients with myocardial infarction with obstructive coronary arteries, patients with MINOCA presented with lower GRACE score (115 vs. 135, p < 0.001) (Table 2).
When the angiographic characteristics were analyzed, 62 patients (72.9%) had normal coronary arteries and 23 patients (27%) had coronary stenoses < 50%. Although the median troponin level was higher in patients with coronary artery obstructions than in those with normal coronary arteries, this difference was not statistically significant. Additionally, the proportion of patients with normal electrocardiograms was not statistically different between the two groups (Table 3).
The additional tests performed to patients with suspected MINOCA included cardiac magnetic resonance imaging in 16 patients (18.8%) during hospitalization and computed tomography coronary angiography in 8 (9.4%). Intracoronary spasm provocation test was performed in only one patient. Intravascular ultrasound (IVUS) or optical coherence tomography (OCT) were not performed in any patient. One patient underwent non-invasive assessment of endothelial dysfunction, and another patient underwent myocardial perfusion SPECT imaging.
The final diagnosis of the MINOCA mechanism assigned by the principal investigator of each center was microvascular dysfunction in 52 patients (61.2%), coronary spasm in 18 patients (21.5%), plaque accident in 6 patients (7.1%), coronary artery dissection in 3 patients (3.5%), and coronary embolism in 1 patient (1.2%). The mechanism was not assigned in 5 patients.
Median length of hospital stay was 3 days (2-4). Atrial fibrillation was the most common complica tion (4 patients). Two patients had recurrent angina or reinfarction, 1 patient had ventricular tachycardia/ fibrillation (VT/VF) and 3 patients had signs of heart failure. There were no bleeding events BARC ≥ type 2. No deaths were reported. Compared to patients with myocardial infarction with obstructive coronary arteries, MINOCA patients had fewer ischemic events (death/infarction/stroke 1.2% vs. 7.9%, p=0,021) and a trend to fewer bleeding events BARC ≥ type 2 (0 vs. 4.2%, p = 0.061) during hospitalization (Table 4).
At hospital discharge, aspirin was prescribed to 62 patients (72.9%) and P2Y12 receptor inhibitors to 23 (27.1%) patients. Dual antiplatelet therapy was prescribed to 22 patients (22.9%) (Table 5).
Table 1. General characteristics of the population with MINOCA

BMI: body mass index; CKD: chronic kidney disease; COPD: chronic obstructive pulmonary disease; IQR: interquartile range; MINOCA: myocardial infarction with non-obstructive coronary arteries; TIA: transient ischemic attack
DISCUSSION
Our study shows a prevalence of MINOCA of 8.6% in hospitalized patients with suspected ACS. We would like to highlight some of our findings.
First, in our registry, the prevalence of non-obstructive coronary arteries on coronary angiography among all patients hospitalized for ACS was 10.6%, which is similar to the one reported in other registries. Gehrie et al. found a prevalence of 10% in patients with non-ST-segment elevation ACS in a retrospective analysis of the CRUSADE registry. (13) In the analysis of MINOCA in the retrospective ACTION registry- GWTG (9) and the extensive meta-analysis of MINOCA by Pasupathy et al., the incidence reported was 6%. (6) In Argentina, the CONAREC XVII Registry on ACS found that 2.8% of patients had no coronary artery stenoses on angiography and 7.7% had moderate obstructions. (14) In all these registries, the term MINOCA is used as a working diagnosis, which means that it does not exclude conditions such as Takotsubo or myocarditis, but rather includes them as possible causes of MINOCA. In our registry, we attempted to exclude non-ischemic injuries and found a prevalence of MINOCA of 8.6%.
Second, half of the MINOCA patients in this registry are women. The proportion of women in this registry is similar to that of other registries, but differs from registries of myocardial infarction with significant epicardial lesions, where the proportion of women is lower. (6, 15, 16) The age found in our registry is similar to that of patients with myocardial infarction with obstructive coronary arteries but differs from that described in other registries, where the age of MINOCA patients was lower than that of patients with significant coronary artery disease. (9, 17)
Table 2. Characteristics on admission

HR: heart rate; IQR: interquartile range; LBBB: left bundle branch block; LVEF: left ventricular ejection fraction; MINOCA: myocardial infarction with non-obstructive coronary arteries; RDW: red cell distribution width; SBP: systolic blood pressure.
Table 3. Comparison of troponin levels and ECG in MINOCA patients with or without coronary artery disease on angiography.

*High-sensitive cardiac troponins expressed as multiples of p99. Median (P25-75) CAD: coronary artery disease; ECG: electrocardiogram; MINOCA: myocardial infarction with non-obstructive coronary arteries; NS: non-significant.
Third, in our registry the prevalence of traditional coronary risk factors is lower than the one found in myocardial infarctions with epicardial coronary artery disease. It is worth noting that the prevalence of diabetes is lower, which is consistent with other MINOCA registries. (7, 18) This registry also collected data on women-specific risk factors, such as hypertensive disorders of pregnancy, gestational diabetes, and menopause-related factors. The prevalence of these risk factors was lower than that described in other registries such as the VIRGO study, a registry of coronary syndromes in patients < 55 years with a special focus on nontraditional risk factors. (18) There may be a data collection bias related to the lack of routine asking about women-specific risk factors.
Fourth, most MINOCA patients presented as non- ST-segment elevation ACS with moderate elevation of cardiac troponins on admission and clinical stability. Although the risk estimated by the GRACE score was moderate, the rate of in-hospital events was low and there were no in-hospital deaths. Similarly, we could not confirm in our registry that the presence of cor onary artery disease is associated with a worse outcome during hospitalization, as some registries have previously described. (19) The question of long-term outcomes remains, and we hope to answer it when we complete the analysis of the one-year follow-up.
Fifth, most MINOCA patients did not undergo additional tests during hospitalization to determine the etiology. This is particularly striking for cardiac magnetic resonance imaging, considered essential for the diagnosis of MINOCA, which was performed in only 18.8% of patients. It is possible that cardiac magnetic resonance imaging was not performed during hospitalization due to unavailability at the center or to avoid prolonging hospitalization for low-risk patients. It is also possible that the test was performed after discharge. Furthermore, it can be hypothesized that intravascular diagnostic tests or intracoronary spasm provocation tests are not widely available in our setting, and noninvasive methods for diagnosing coronary artery spasm or microvascular dysfunction are not widely used or known. Nevertheless, it is also true that the etiologic diagnosis of MINOCA begins during hospitalization and is often completed in the outpatient setting. The Argentine Consensus Statement on MINOCA, recently published, can assist in the initial management and diagnosis of these patients. (4) Due to the low rate of tests performed during hospitalization, the population described in this registry may be more indicative of a working diagnosis than of a confirmed diagnosis of MINOCA.
However, the main etiologic diagnosis ascribed by the investigator of each center was microvascular dysfunction in 62.1% of the cases. According to several studies that further investigate the etiology of MINOCA using a combination of cardiac magnetic resonance imaging and intravascular imaging, at least half of MINOCA cases are due to plaque injury, followed by coronary artery spasm and cases of undetermined etiology, while spontaneous coronary artery dissection and embolism are less common. (19, 20) The possible causes of MINOCA may still be unknown or confused with INOCA (ischemia without obstructive coronary artery disease), a condition in which microvascular dysfunction is very common.
Finally, there is little evidence on the optimal treatment for MINOCA after discharge from the index hospitalization. Dual antiplatelet therapy has not been shown to reduce events, and the use of statins, renin-angiotensin-aldosterone system antagonists, and beta-blockers may have a protective effect. (21-24) In our registry, the use of dual antiplatelet therapy at discharge was significantly higher than at admission, but was used in only 22.9% of patients, which is related to the etiologic diagnosis assigned. Secondary prevention with statins was high and, together with beta blockers, prescription was greater than on admission
The strength of our registry lies in its prospective description of MINOCA, providing data that are hard to obtain from retrospective analyses of registries designed with different objectives. Post-discharge monitoring of patients will provide data on long-term outcome. We expect that this study will help to generate hypotheses for future research to clarify the prognosis and optimal treatment of patients with MINOCA.
Table 4. Complications during hospitalization

IQR: interquartile range; MV: mechanical ventilation; TIA: transient ischemic attack; VF: ventricular fibrillation; VT: ventricular tachycardia.
Table 5. Medication on admission and discharge
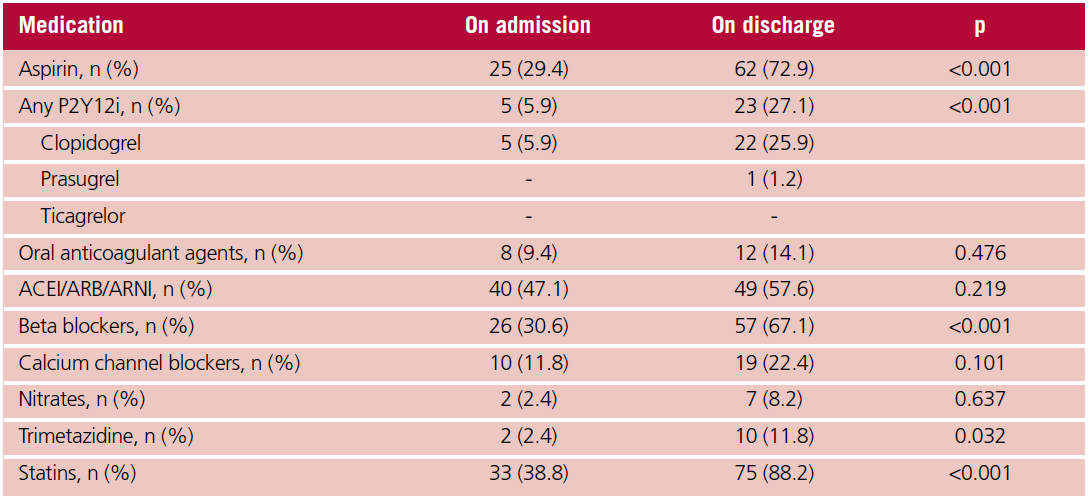
ACEI: angiotensin-converting enzyme inhibitor; ARB: Angiotensin II receptor blocker; ARNI: angiotensin receptor neprilysin inhibitor; P2Y12i: P2Y12 receptor inhibitor
STUDY LIMITATIONS
Due to the requirement of signing an informed consent form and the nature of this registry, we cannot guarantee the consecutive inclusion of patients. Therefore, the prevalence found in our study may not accurately reflect reality. The involvement of centers primarily located in the Buenos Aires metropolitan area may result in data not representative of the entirety of Argentina. In addition, the interpretation of the coronary angiograms was the responsibility of the investigators at each center and not of a central group. In any case, we believe that the registry represents the characteristics of hospitalized patients in "real life".
CONCLUSIONS
In this registry, patients with MINOCA represent a significant proportion of those with ACS. The rate of in-hospital complications, including mortality, was low. There seems to be a strong opportunity for further investigations to confirm the diagnosis, pathophysiological mechanisms, and treatment of MINOCA.
Conflicts of interest
None declared.
(See conflicts of interest forms on the website).
Sources of funding
None.
https://creativecommons.org/licenses/by-nc-sa/4.0/

©Revista Argentina de Cardiología
REFERENCES
- Beltrame JF. Assessing patients with myocardial infarction and nonobstructed coronary arteries (MINOCA). J Intern Med. 2013;273:182-5. https://doi.org/10.1111/j.1365-2796.2012.02591.x
- Agewall S, Beltrame JF, Reynolds HR, Niessner A, Rosano G, Caforio AL, et al; WG on Cardiovascular Pharmacotherapy. ESC working group position paper on myocardial infarction with non-obstructive coronary arteries. Eur Heart J. 2017;38:143-53. https://doi.org/10.1093/eurheartj/ehw149
- Tamis-Holland JE, Jneid H, Reynolds HR, Agewall S, Brilakis ES, Brown TM, et al; American Heart Association Interventional Cardiovascular Care Committee of the Council on Clinical Cardiology; Council on Cardiovascular and Stroke Nursing; Council on Epidemiology and Prevention; and Council on Quality of Care and Outcomes Research. Contemporary Diagnosis and Management of Patients With Myocardial Infarction in the Absence of Obstructive Coronary Artery Disease: A Scientific Statement From the American Heart Association. Circulation. 2019;139:e891-e908. https://doi.org/10.1161/CIR.0000000000000670
- Charask A, Cohen Arazi H, Rivero M, Allin J, Álvarez J, Campisi R. Consenso de Minoca. Sociedad Argentina de Cardiología. Infarto Agudo de Miocardio sin Enfermedad Coronaria Obstructiva. Rev Argent Cardiol 2022;90:1-34.
- Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, et al; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). J Am Coll Cardiol. 2018;72:2231-64. https://doi.org/10.1016/j.jacc.2018.08.1038
- Pasupathy S, Air T, Dreyer RP, Tavella R, Beltrame JF. Systematic review of patients presenting with suspected myocardial infarction and nonobstructive coronary arteries. Circulation. 2015;131:861-70. https://doi.org/10.1161/CIRCULATIONAHA.114.011201
- Rakowski T, De Luca G, Siudak Z, Plens K, Dziewierz A, Kleczyński P, et al. Characteristics of patients presenting with myocardial infarction with non-obstructive coronary arteries (MINOCA) in Poland: data from the ORPKI national registry. J Thromb Thrombolysis. 2019;47:462-6. https://doi.org/10.1007/s11239-018-1794-z
- Ciliberti G, Coiro S, Tritto I, Benedetti M, Guerra F, Del Pinto M, et al. Predictors of poor clinical outcomes in patients with acute myocardial infarction and non-obstructed coronary arteries (MINOCA). Int J Cardiol. 2018;267:41-5. https://doi.org/10.1016/j.ijcard.2018.03.092
- Smilowitz NR, Mahajan AM, Roe MT, Hellkamp AS, Chiswell K, Gulati M, et al. Mortality of Myocardial Infarction by Sex, Age, and Obstructive Coronary Artery Disease Status in the ACTION Registry-GWTG (Acute Coronary Treatment and Intervention Outcomes Network Registry-Get With the Guidelines). Circ Cardiovasc Qual Outcomes. 2017;10:e003443. https://doi.org/10.1161/CIRCOUTCOMES.116.003443
- Bainey KR, Welsh RC, Alemayehu W, Westerhout CM, Traboulsi D, Anderson T, Brass N, et al. Population-level incidence and outcomes of myocardial infarction with non-obstructive coronary arteries (MINOCA): Insights from the Alberta contemporary acute coronary syndrome patients invasive treatment strategies (COAPT) study. Int J Cardiol. 2018;264:12-7. https://doi.org/10.1016/j.ijcard.2018.04.004
- Harris PA, Taylor R, Minor BL, Elliott V, Fernandez M, O’Neal L, et al; REDCap Consortium. The REDCap consortium: Building an international community of software platform partners. J Biomed Inform. 2019;95:103208. https://doi.org/10.1016/j.jbi.2019.103208
- Rivero M, Feder J, Procopio G, Gingins M, Souto JM, Villarreal R, y cols. Registro de síndromes coronarios agudos en centros de Argentina. ReSCAR 2022. Rev Argent Cardiol 2023;91:205-11. http://dx.doi.org/10.7775/rac.es.v91.i3.20631.
- Gehrie ER, Reynolds HR, Chen AY, Neelon BH, Roe MT, Gibler WB, et al. Characterization and outcomes of women and men with non-ST-segment elevation myocardial infarction and nonobstructive coronary artery disease: results from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement initiative. Am Heart J. 2009;158:688-94. https://doi.org/10.1016/j.ahj.2009.08.004
- Rossler C, Morbidoni J, Santillán ME, Sigal A, Ocampos R, Cattaneo JP, et al. Infarto de miocardio sin lesiones coronarias. Subanálisis del Registro CONAREC XVII [Myocardial infarction without coronary arteries lesions. Insights from the CONAREC XVII Registry]. Medicina (B Aires). 2021;81:375-81.
- Costabel JP, Zaidel E, Rivero M, Gómez I, Pérez GE, Garmendia C, et al. Registro multicéntrico prospectivo de pacientes hospitalizados por síndrome coronario agudo sin elevación del segmento STen centros de alta complejidad. Resultados intrahospitalarios y evolución a 6 meses (Buenos Aires I ). Rev Argent Cardiol 2020;88:308-16. http://dx.doi.org/10.7775/rac.es.v88.i4.18501
- Gagliardi J, Charask A, Perna E, D’Imperio H, Bono J, Castillo Costa Y, et al. . Encuesta nacional de infarto agudo de miocardio con elevación del segmento ST en la República Argentina (ARGEN-IAM-ST). Rev Argent Cardiol 2016;84:548-57. http://dx.doi.org/10.7775/rac.es.v84.i6.9508
- Montenegro Sá F, Ruivo C, Santos LG, Antunes A, Saraiva F, Soares F, et al. Myocardial infarction with nonobstructive coronary arteries: a single-center retrospective study. Coron Artery Dis. 2018;29:511-5. https://doi.org/10.1097/MCA.0000000000000619
- Safdar B, Spatz ES, Dreyer RP, Beltrame JF, Lichtman JH, Spertus JA, et al. Presentation, Clinical Profile, and Prognosis of Young Patients With Myocardial Infarction With Nonobstructive Coronary Arteries (MINOCA): Results From the VIRGO Study. J Am Heart Assoc. 2018;7:e009174. https://doi.org/10.1161/JAHA.118.009174
- Zeng M, Zhao C, Bao X, Liu M, He L, Xu Y, et al. Clinical Characteristics and Prognosis of MINOCA Caused by Atherosclerotic and Nonatherosclerotic Mechanisms Assessed by OCT. JACC Cardiovasc Imaging. 2023;16:521-32. https://doi.org/10.1016/j.jcmg.2022.10.023
- Reynolds HR, Maehara A, Kwong RY, Sedlak T, Saw J, Smilowitz NR, et al. Coronary Optical Coherence Tomography and Cardiac Magnetic Resonance Imaging to Determine Underlying Causes of Myocardial Infarction With Nonobstructive Coronary Arteries in Women. Circulation. 2021;143:624-40. https://doi.org/10.1161/CIRCULATIONAHA.120.052008
- Lindahl B, Baron T, Erlinge D, Hadziosmanovic N, Nordenskjöld A, Gard A, et al. Medical Therapy for Secondary Prevention and Long-Term Outcome in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. Circulation. 2017;135:1481- 9. https://doi.org/10.1161/CIRCULATIONAHA.116.026336
- Abdu FA, Liu L, Mohammed AQ, Xu B, Yin G, Xu S, et al. Effect of Secondary Prevention Medication on the Prognosis in Patients With Myocardial Infarction With Nonobstructive Coronary Artery Disease. J Cardiovasc Pharmacol. 2020;76:678-83. https://doi.org/10.1097/FJC.0000000000000918
- De Filippo O, Russo C, Manai R, Borzillo I, Savoca F, Gallone G, et al. Impact of secondary prevention medical therapies on outcomes of patients suffering from Myocardial Infarction with NonObstructive Coronary Artery disease (MINOCA): A meta-analysis. Int J Cardiol. 2022;368:1-9. https://doi.org/10.1016/j.ijcard.2022.08.034
- Bossard M, Gao P, Boden W, Steg G, Tanguay JF, Joyner C, et al. Antiplatelet therapy in patients with myocardial infarction without obstructive coronary artery disease. Heart. 2021;107:1739-47. https://doi.org/10.1136/heartjnl-2020-318045
LISTADO DE CENTROS PARTICIPANTES E INVESTIGADORES, ORDENADOS ALFABÉTICAMENTE
CEMIC: Mirza Rivero, Mayra Meza, Sol Kersten, Carlos Boissonnet.
CEMEP: Gerardo Filippa.
Clínica Olivos: Fernando Guardiani, Sebastian Nani.
Fundación Favaloro: Ernesto Duronto, Gastón Procopio, Camila Marian Abud, Santiago Andrés Ahuad Calvelo.
Hospital Austral: Jorge Bilbao, Nicolás Torres.
Hospital Británico: Mauro Gingins, Gisela Gomez, Federico Deveter.
Hospital de Clínicas: Sandra Swieszkowski, Martin Aladio, Maia Matsudo.
Hospital Durand: Valentín Roel.
Hospital Naval: Guillermo Perez.
ICBA: Juan P Costabel, Julian Feder, Alan Sigal.
Instituto Médico de la Ribera: Valerio Pessano, Juan Pablo Larralde
Sanatorio Anchorena San Martín: Leandro Rodriguez. Juan Manuel Souto.
Sanatorio Finochietto: Diego Crippa.
Sanatorio Güemes: Ricardo Villareal, Joaquín Perea, Agustina Saucedo, Elena Vargas.
Sanatorio Trinidad de Palermo: Federico Cardone.