
INTRODUCTION
Transthyretin cardiac amyloidosis (ATTR-CA) is a disease characterized by the deposition in the myocardium of misfolded fibrils derived from transthyretin, a protein produced primarily by the liver. (1,2) Transthyretin cardiac amyloidosis can be sporadic or hereditary. The non-hereditary wild-type form (ATTRwt-CA) is the most common; it presents in later stages of life and has a median survival of 3 to 5 years. The hereditary form (ATTRv-CA) is associated with mutations in the transthyretin gene and typically manifests at younger ages; it follows an autosomal dominant inheritance pattern with variable penetrance, while the course of the disease and survival vary among different families and among different genotypes. (3)
Historically, this condition was considered a rare disease; however, its diagnostic incidence has increased exponentially in recent years.(4) This increase is driven primarily by the availability of national and international diagnostic algorithms that enable the noninvasive diagnosis of the disease using imaging methods such as bone scintigraphy with bisphosphonates.(5,6) Moreover, the emergence of specific therapies that modify the natural course of the disease are likely to have contributed to the rise in diagnostic incidence.(7-9) Currently, the prevalence of ATTR-CA is high in very common cardiac conditions, such as heart failure with preserved ejection fraction and aortic stenosis, among others.(10-15)
It is well known that there is a clear male predominance in ATTR-CA. Various studies have reported that more than 85% of patients with ATTRwt-CA are men, (16) so the available information on the clinical characteristics of women with this condition is limited. On the other hand, although differences in clinical presentation and disease progression according to gender in ATTR-CA, have been reported, (17) the evidence in this regard is limited, and we lack local or regional data on these differences.
The objective of this study was to describe sexrelated differences in clinical presentation, electrocardiographic and imaging characteristics at the time of diagnosis, and the course of the disease in patients diagnosed with ATTR-CA.
METHODS
Study Design and Population
A retrospective, multicenter (two centers) cohort study was conducted in patients diagnosed with ATTR-CA between January 2010 and June 2025, enrolled in our Institutional Amyloidosis Registry (IAR). The IAR is an active registry that has been consecutively and retrospectively enrolling cases diagnosed with amyloidosis since 2010. It was approved by the Hospital Italiano de Buenos Aires Ethics Committee (CEPI 1675) and registered on ClinicalTrials.gov (NCT01347047).
The diagnosis of ATTR-CA was based on clinical suspicion by the patient’s attending physicians and was established as follows:
Positive bone scintigraphy with bisphosphonates (uptake grade ≥ 2 according to the Perugini visual scale) and confirmation of myocardial uptake via single-photon emission computed tomography (SPECT-CT), in the absence of hematological findings suggestive of light-chain amyloidosis.
In cases diagnosed before 2017 (the year in which pyrophosphate bone scintigraphy was introduced at our institution), the diagnosis was accepted in the presence of a positive endomyocardial or extracardiac biopsy with Congo red staining, along with typical findings on cardiac magnetic resonance imaging and negative hematological studies.
Although not all patients underwent transthyretin gene sequencing, in most cases genetic testing was performed to rule out ATTRv-CA. Patients with other forms of amyloidosis or who were not followed up at our center were excluded from the analysis.
Variables
Demographic information (sex and age at diagnosis) and associated comorbidities (hypertension, dyslipidemia, diabetes mellitus, atrial fibrillation and heart failure, among others) were collected. Laboratory data were also recorded, including serum creatinine, creatinine clearance calculated using the Cockcroft-Gault formula, N-terminal pro-B-type natriuretic peptide (NT-proBNP), and ultrasensitive cardiac troponin T.
Pre-diagnosis electrocardiograms were also reviewed, assessing the baseline rhythm (sinus or atrial fibrillation/flutter), the presence of microvoltage-defined as a QRS complex amplitude of less than 5 mm in all limb leads and/or less than 10 mm in the precordial leads- the pseudo-infarction pattern-defined as the presence of pathological Q waves or loss of R-wave progression, without clinical or angiographic evidence of prior infarction-and the presence of right bundle branch block.
Imaging study variables were also analyzed, including classic echocardiographic and cardiac magnetic resonance imaging (MRI) parameters, using the studies closest to the diagnosis of ATTR-CA (within six months for echocardiography and within one year for MRI). Finally, hospitalizations for heart failure and all-cause mortality during follow-up were recorded.
Statistical Analysis
Continuous variables were expressed as mean ± standard deviation (SD) or as median and interquartile range (IQR), depending on their distribution. Categorical variables were expressed as percentages. Baseline characteristics were compared between men and women using appropriate statistical tests, employing the chi-square test for categorical variables and Student’s t-test or the Mann-Whitney test for continuous variables, according to their parametric or nonparametric distribution, respectively.
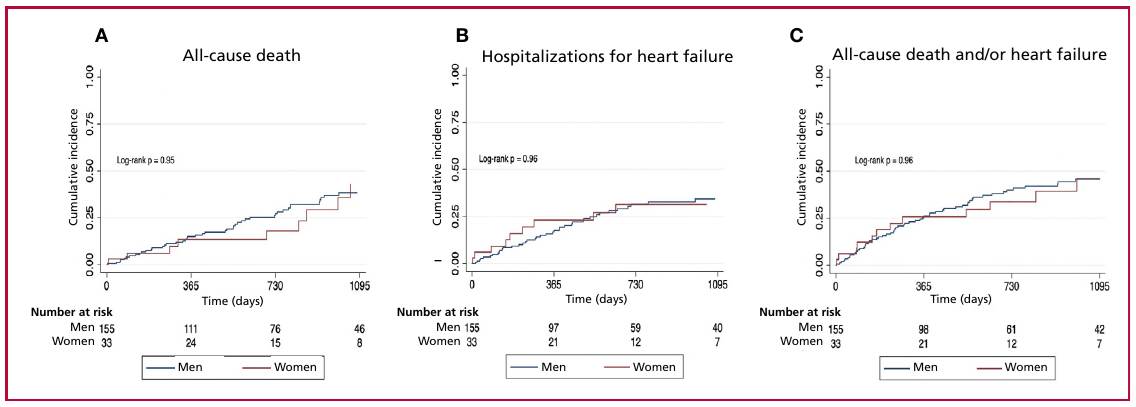
Finally, Kaplan-Meier curves were constructed to estimate the incidence of all-cause mortality, hospitalizations for heart failure, and the combined event of both outcomes during follow-up, stratified by sex. A two-sided p-value <0.05 was considered statistically significant. All analyses were performed using STATA software version 13.1 (Stata Corp LP, College Station, TX).
Ethical Considerations
The study protocol complied with the ethical principles of the Declaration of Helsinki. (18) The Institutional Amyloidosis Registry (IAR) was approved by the institutional ethics committee, and all participants provided informed consent prior to inclusion in the registry.
RESULTS
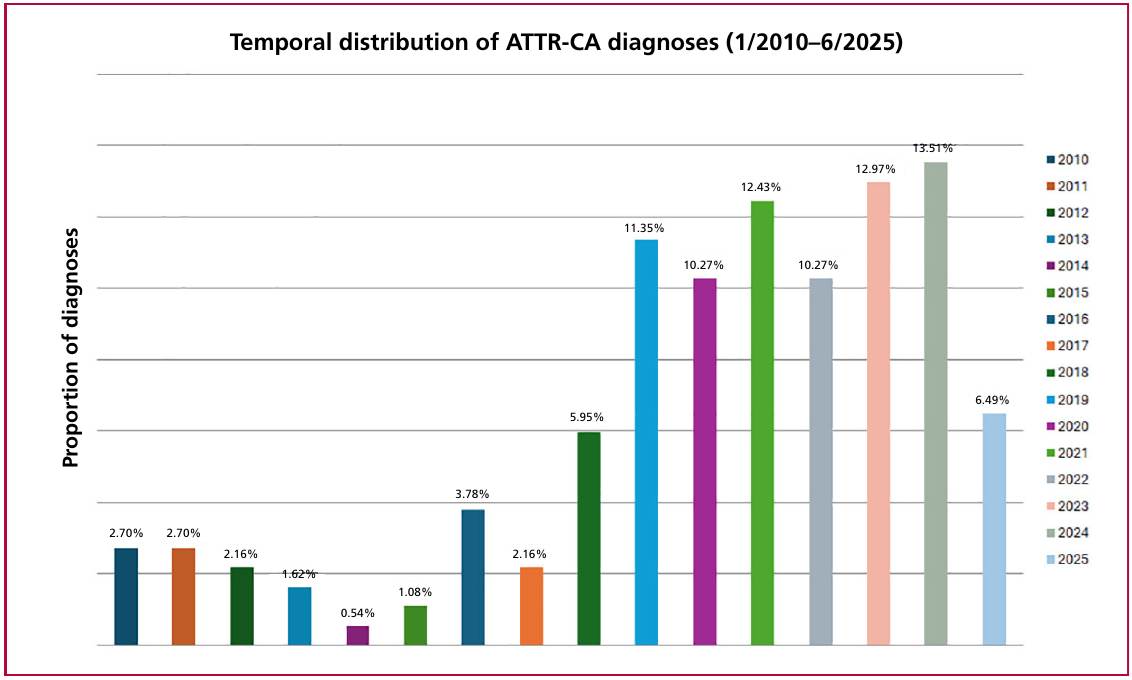
A total of 186 patients were included in the study, among whom 15 (8%) had a diagnosis of ATTRv-CA. Since the introduction of bone scintigraphy with bisphosphonates in 2017, 159 of the 186 patients (85.5%) included in the cohort were diagnosed, with a clear increase in disease incidence observed in recent years (Figure 1). Of the total number of patients diagnosed by scintigraphy (n=159), 92.4% (n=147) had a Perugini visual score of 3 points, 6.9% (n=11) had a score of 2 points, and only 1 patient had a Perugini score of 1; the latter was diagnosed with ATTRv-CA due to Val50Met, with advanced cardiac and neurological involvement.
Population mean age was 80±8 years; 82.2% were men (n=153, 142 ATTRwt-CA and 11 ATTRvCA), and 17.8% were female (n=33, 29 ATTRwtCA and 4 ATTRv-CA). Clinical differences between men and women at the time of diagnosis evidenced that women were diagnosed at an older age (83 vs. 80 years; p=0.042), and more frequently presented with dyslipidemia (69.7% vs. 45.1%; p=0.012). They had poorer creatinine clearance (46 mL/min vs. 56 mL/min; p=0.024) compared with men, with no significant differences in NT-ProBNP and ultrasensitive cardiac troponin T levels. The differences in clinical and laboratory variables between men and women are presented in Table 1.
Table 1
Differences in clinical history and laboratory variables between men and women with ATTR-CA at the time of diagnosis.
| Hombres (n=153) | Mujeres (n=33) | p | |
|---|---|---|---|
| Edad, años, media ± DE | 80 ±7 | 83 ±9 | 0,042 |
| Hipertensión arterial, n (%) | 117 (76,5) | 28 (84,8) | 0,292 |
| Dislipidemia, n (%) | 69 (45,1) | 23 (69,7) | 0,012 |
| Diabetes Mellitus, n (%) | 30 (19,6) | 5 (15,2 ) | 0,554 |
| IRC (ClCr < 60 mL/min), n (%) | 29 (19,0) | 8 (24,2) | 0,493 |
| Coronariopatía, n (%) | 29 (19,0) | 4 (12,1) | 0,350 |
| ACV/AIT, n (%) | 13 (8,5) | 12 (36,4) | 0,512 |
| Insuficiencia cardiaca, n (%) | 94 (61,4) | 20 (60,6) | 0,921 |
| CF III/IV NYHA, n (%) | 53 (34,6) | 12 (36,4) | 0.633 |
| Antecedente de fibrilación/aleteo auricular, n (%) | 80 (52,3) | 14 (42,4) | 0,302 |
| Hipotensión arterial, n (%) | 13 (8,5) | 6 (18,2) | 0,092 |
| Túnel carpiano, n (%) | 65 (42,5) | 15 (45,5) | 0,753 |
| Canal estrecho lumbar, n (%) | 31 (20,3) | 6 (18,2) | 0,861 |
| ClCr, ml/min, media ± DE | 56 ±21 | 46 ±20 | 0,024 |
| NT-proBNP, pg/mL, mediana (RIC) | 2412 (988-5336) | 3249 (2065-5464) | 0,192 |
| TTUS, pg/mL, mediana (RIC) | 51 (35-77) | 45 (29-58) | 0,164 |
CKD: chronic kidney disease; CrCl: creatinine clearance; IQR: interquartile range; NT-proBNP: N-terminal pro-B-type natriuretic peptide; NYHA FC: New York Heart Association functional class; SD: standard deviation; TIA: transient ischemic attack; US-TT: ultrasensitive cardiac troponin T.
Regarding the baseline electrocardiogram at the time of diagnosis, 62% (33.3%) of patients presented with atrial fibrillation or flutter, with no significant differences observed between men and women (64.7% vs 51.5%, p=0.162). Among other electrocardiographic features, the most common finding was the pseudo-infarction pattern, observed in 67.2% of patients (67.9% in men vs. 60.6% in women, p=0.445), followed by microvoltage, present in 39.8% of cases, with a tendency to be more frequent in men (44.2% vs. 27.2%, p=0.063). Finally, right bundle branch block was present in 37.1% of patients, with no significant differences between men and women (39.1% vs. 24.2%, p=0.161).
On the baseline echocardiogram, women had a larger end-diastolic diameter normalized by body surface area (25 mm/m² vs. 23 mm/m²; p=0.002) and lower septal and posterior wall thickness (14.8 vs. 16.9 mm; p=0.020 and 12.7 vs. 14.3 mm; p=0.005, respectively) compared with men. On the other hand, a higher proportion of women had septal thickness <12 mm at the time of ATTR-CA diagnosis (12.1% vs. 1.9%; p=0.005) Moreover, women tended to have better myocardial fiber function with higher global longitudinal strain values (-14.1% vs. -11.1%; p=0.072), with no significant differences in left ventricular ejection fraction calculated using the Simpson method (Table 2).
Table 2
Differences in echocardiographic variables between men and women with ATTR-CA at the time of diagnosis.
| Hombres (n=153) | Mujeres (n=33) | p | |
|---|---|---|---|
| DFDVI, mm, media ± DE | 45 ±6 | 41 ±5 | 0,006 |
| DFDVIi, mm/m2, media ± DE | 23 ±3 | 25 ±3 | 0,002 |
| DFSVI, mm, media ± DE | 28 ±7 | 26 ±7 | 0,072 |
| DFSVIi, mm/m2 , media ± DE | 15 ±3 | 16 ±4 | 0,143 |
| Espesor septal, mm, media ± DE | 16,9 ±3,5 | 14,8 ±3,5 | 0,020 |
| Espesor septal indexado, mm/m2 , media ± DE | 9 ±2 | 9 ±2 | 0,562 |
| Pared posterior, mm, media ± DE | 14,3 ±2,9 | 12,7 ±2,3 | 0,005 |
| Pared posterior indexada, mm/m2 , media ± DE | 7,5 ±1,8 | 7,9 ±1,7 | 0,271 |
| FEVI, %, media ± DE | 53 ±11 | 55 ±9 | 0,342 |
| Volumen AI, ml/m2, mediana (RIC) | 56 (47-68) | 56 (46-69) | 0,932 |
| Relación E/e' septal, mediana (RIC) | 19 (16-24) | 22 (14-26) | 0,401 |
| TAPSE, mm, media ± DE | 19 ±4 | 20 ±4 | 0,762 |
| Disfunción VD, n (%) | 43 (28,1) | 8 (24,2) | 0,613 |
| PSAP, mmHg, mediana (RIC) | 39 (31-49) | 39 (32-53) | 0,333 |
| EA moderada o grave, n (%) | 23 (15,0) | 3 (9,1) | 0,345 |
| SLG, %, mediana (RIC) (n=82) | -11,1 (-9,1 - -14,1) | -14,1 (-10,1 - -18) | 0,072 |
AS: aortic stenosis; GLS: global longitudinal strain; IQR: interquartile range; LA: left atrial; LVEDD: left ventricular end-diastolic diameter; LVEDDi: left ventricular end-diastolic diameter indexed to body surface area; LVEF: left ventricular ejection fraction; LVESD: left ventricular end-systolic diameter; LVESDi: left ventricular end-systolic diameter indexed to body surface area; PASP: pulmonary artery systolic pressure; PW: posterior wall; PWi: posterior wall indexed to body surface area; RV: right ventricular; SD: standard deviation; ST: septal thickness; STi: septal thickness indexed to body surface area; TAPSE: tricuspid annular plane systolic excursion
A total of 108 patients (93 men and 15 women) underwent cardiac MRI within the year of diagnosis. In this study, women had higher left and right ventricular ejection fractions (62% vs. 50%; p=0.031 and 56% vs. 47%; p=0.011, respectively) and lower maximum wall thickness (16.4 mm vs. 18.7 mm; p=0.013) compared with men (Table 3). No differences were observed in T1 mapping and extracellular volume sequences between men and women. In the subgroup of patients with cardiac MRI, no differences were either observed in ejection fraction and global longitudinal strain by echocardiography.
Table 3
Differences in magnetic resonance imaging variables between men and women with ATTR-CA at the time of diagnosis.
| Resonancia cardiaca (n=108) | Hombres (n=93) | Mujeres (n=15) | p |
|---|---|---|---|
| FEVD, % , mediana (RIC) | 50 (42-61) | 62 (48-71) | 0,031 |
| Máximo espesor, mm, media ± DE | 18,7 ±3,1 | 16,4 ±3,4 | 0,013 |
| FEVD, %, media ± DE | 47 ±13 | 56 ±13 | 0,011 |
| T1 mapping, mseg, media ± DE | 1118 ±50) | 1108 ±72 | 0,582 |
| VEC, %, mediana (RIC) | 48 (41-53) | 48 (33-58) | 0,913 |
ECV: extracellular volume; IQR: interquartile range; LVEF: left ventricular ejection fraction; RVEF: right ventricular ejection fraction;
MRI: magnetic resonance imaging; SD: standard deviation
During follow-up, only 34 patients received specific disease-modifying treatment (transthyretin stabilizers); among these, 29 were men and 5 were women (p=0.462) Finally, during a median follow-up of 725.5 days (IQR 342.5-1220), no statistically significant differences were observed in mortality or hospitalizations for heart failure between the two sexes (Figure 2 A, B, and C).
DISCUSSION
In this observational cohort, using local data, we describe the differences in clinical presentation, imaging characteristics at diagnosis, and clinical course of patients diagnosed with ATTR-CA according to sex. The first point to highlight is the marked male predominance (82%) observed in our cohort. This finding is consistent with previously reported epidemiological data for this condition. Studies conducted in European and North American populations have reported similar proportions (19-24), with some variability across series. The lowest prevalence among women was reported in 2022 in the international THAOS registry, where, out of a total of 1386 patients, only 6% were female. (20) On the other hand, the highest prevalence was recently reported in January 2026, using data from the ATTR-CA registry in Galicia, Spain, where, out of a total of 385 patients, 24.7% were women. (22)
In our population, women were diagnosed at a significantly older age than men, a finding that has also been consistently reported in previous international series. (19-21,24) There are hypotheses suggesting that the lower proportion of women and the later age at diagnosis could be explained by hormonal factors, particularly the protective role of estrogens on the myocardium and transthyretin metabolism. Experimental studies have suggested that estrogens may stabilize the transthyretin tetramer and reduce its propensity for dissociation and subsequent amyloid deposition, which would delay the onset of clinical manifestations in women. (25) In this context, it has been proposed that the decrease in estrogen levels following menopause could contribute to greater susceptibility to cardiac involvement and disease progression, which could explain, at least partially, the diagnosis at older ages in this group. (17)
In turn, both echocardiography and cardiac magnetic resonance imaging showed that women exhibited a lower degree of wall thickening compared with men. These findings could also suggest that women present, at the time of diagnosis, with a “less infiltrative” phenotype, which could be interpreted as an earlier manifestation or a slower progression of the disease. However, several groups, including the National Amyloidosis Centre in London, have emphasized the importance of reviewing traditional diagnostic algorithms, where diagnostic suspicion is based on septal thicknesses greater than 12 mm on echocardiography. (26) In this regard, they highlight the importance of indexing septal thickness values to body surface area to avoid underdiagnosis in women. (21,27) Supporting this theory, in our cohort there were no differences in septal and posterior wall thickness values after indexing these values to the patients’ body surface area. However, the indexing of septal thickness values is not yet included in the recommendations of the most widely recognized global echocardiographic clinical practice guidelines. (28) As an additional finding, in our cohort, 12% of women had a septal thickness <12 mm, which supports the theory that diagnostic algorithms and classic echocardiographic criteria may contribute to some underdiagnosis of the condition in women.
Regarding myocardial function at the time of diagnosis, in contrast to other studies in which women had a higher left ventricular ejection fraction on echocardiography, (20,27,29) in our cohort we did not observe statistically significant differences between sexes, probably due to the study’s lack of statistical power. However, there was a trend towards better-preserved global longitudinal strain values in women, a tool recognized as more sensitive for the early detection of myocardial dysfunction, particularly in this condition. (30) On the other hand, cardiac MRI showed significantly higher left and right ventricular ejection fractions in women, which reinforces the hypothesis of less advanced functional impairment at the time of diagnosis. Cardiac MRI is the gold standard for assessing systolic ventricular function and may be more accurate for characterizing ventricular function in this population of patients with ATTR-CA. In the subgroup of patients who underwent cardiac MRI, no differences were observed in left ventricular ejection fraction and global longitudinal strain measured by echocardiography, ruling out the possibility that the observed findings were due to a particular patient selection. To date, available information regarding sex differences in cardiac MRI findings is scarce; therefore, our study provides useful insights in this regard.
In our cohort, only a small proportion of patients received specific disease-modifying treatment, with no significant differences observed between men and women. This can be explained, first, by the fact that this is a historical cohort, in which the first patients were diagnosed starting in 2010, while specific therapies for ATTR-CA have only become available in our country in recent years. Second, this is an elderly population, in which the indication for high-cost treatments must be evaluated on an individual basis and, in many cases, is not cost-effective. Furthermore, the economic constraints inherent in our healthcare system constitute an additional factor limiting access to these types of therapies.
Despite differences in age at diagnosis and in the imaging characteristics described, no significant differences were observed in mortality or hospitalizations for heart failure during follow-up between men and women. This finding could be explained by the small number of women included in the cohort and the low proportion of patients who received specific disease-modifying treatment, which limits the statistical power to detect differences in clinical outcomes. The available evidence regarding the impact of sex on the prognosis of ATTR-CA remains contradictory, with some studies reporting worse outcomes in men and others, more recent ones, finding no significant differences between the two sexes, (17) consistent with our results.
Finally, our study has several limitations. First, it is an observational, retrospective study, with the limitations inherent to this type of design. Second, the number of women was low, which limits the interpretation of comparative analyses between sexes. Furthermore, not all patients had a complete genetic characterization, which could have affected the classification of the ATTR-CA subtype in some cases. Lastly, the proportion of patients receiving specific treatment was low, and, as previously mentioned, many patients were diagnosed in the era prior to specific treatments, which prevents an adequate assessment of the impact of sex on the therapeutic response.
CONCLUSIONS
In this national cohort of patients with ATTR-CA, women were diagnosed at an older age and had less structural and functional myocardial involvement at the time of diagnosis. However, these differences did not translate into a significant impact on the clinical course during follow-up.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).
Funding
None.