
INTRODUCTION
The incidence and prevalence of diabetes mellitus (DM) is steadily increasing due to population aging, obesity, and physical inactivity (1) and is associated with the development of macro and microvascular coronary artery disease. (2) It has also been reported that type 2 DM may be associated with cardiomyopathy, particularly with heart failure regardless the presence of associated coronary artery disease, especially in women. (3,4) Heart failure is also related to a poorer prognosis in diabetic patients. (5) In this context, diastolic dysfunction often represents the first manifestation of structural and functional myocardial compromise and is considered more common than systolic dysfunction in diabetic patients without overt ischemic heart disease. (6,7) This pattern has led to the concept of diabetic cardiomyopathy, characterized in early stages by preserved left ventricular ejection fraction (LVEF) and early alterations in ventricular relaxation and distensibility. (8) In recent years, global longitudinal strain (GLS) assessed by echocardiography has emerged as a sensitive marker of subclinical systolic dysfunction, reflecting the involvement of longitudinal myocardial fibers. Several studies have shown that GLS may be reduced in diabetic patients even in the presence of preserved LVEF, suggesting early myocardial damage undetectable by conventional methods. (7,8)
OBJECTIVES
The objective of the present study was to assess differences in echocardiographic systolic and diastolic function and GLS parameters in elderly diabetic versus non-diabetic patients without evidence of ischemic heart disease. A secondary objective was to evaluate the prevalence of significant diastolic dysfunction and associated variables.
METHODS
An observational cohort study was conducted, including consecutive patients referred to the echocardiography service for resting and exercise stress echocardiography. Patients with a history of known coronary artery disease, peripheral vascular disease, stroke, and those unable to exercise were excluded from the study, as were patients with significant (moderate or severe) valvular heart disease. Additionally, patients with a positive test for myocardial ischemia were excluded. The population was divided into two groups based on the clinical history of DM: patients with treated diabetes (DM) and patients without diabetes (No DM). A Vinno E 35 ultrasound system with a 2.4 MHz phased-array transducer was used to perform the study.
The following measurements were acquired at baseline and immediately post-exercise: in the mitral flow graph obtained with pulsed-wave Doppler at the tips of the mitral valves: peak E velocity (E velocity) at rest and immediately post-exercise; in the tissue Doppler recording at the level of the basal septum: e’ velocity at rest and immediately post- exercise (e’ velocity); E/e’ ratio at rest and post-exercise ((Figures 1, 2 and 33); LVEF by the Simpson method in apical 4, and 2-chamber views, averaging both values at rest and immediately post-exercise; GLS (assessed by speckle tracking), averaging the apical 4-, 3-, and 2-chamber views at rest. Exercise testing was performed on a treadmill using the Bruce protocol. Measurements were acquired 1–2 minutes post-exercise when the A and E waves were no longer fused. Significant diastolic dysfunction was defined as moderate (grade 2) or severe (grade 3) diastolic dysfunction according to the definition of the American Society of Echocardiography (9) (Figures 1, 2 and 3) or an E/e’ ratio greater than 14.
Fig. 1.
A.Mild diastolic dysfunction (grade 1). Pulse Doppler mitral filling. The mitral Flow pattern shows peak “E” velocity of 44.86 cm/s and peak “A” velocity of 58.74 cm/s. The corresponding E/A ratio is 0.76. This is the most frequent filling pattern in our study and is very prevalent in subjects over 60 years of age and in initial stage of heart diseases. B. Mild diastolic dysfuntion (grade 1). Mitral annulus tissue Doppler. This image is related to (1) and shows “e’” velocity of 5.52 cm/s , corresponding to an E/e’ ratio of 8.12. These values are associated with low pumonary capillary pressure and absence of cardiac dyspnea
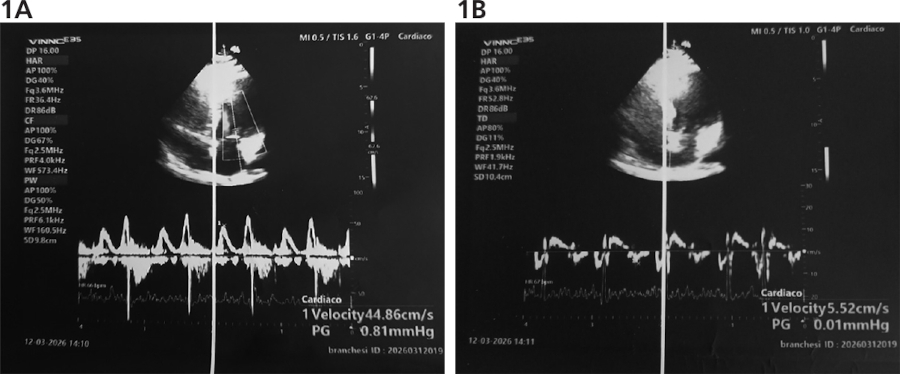
Fig. 2
A.Moderate cardiac dysfunction (grade 2). Pulsed Doppler mitral filling. The image shows peak E velocity of 78.21 cm/s and peak A velocity of 71.01 cm/s, with an E/A ratio of 1.10. This pattern is also called pseudonormal. B. Moderate diastolic dysfunction (grade 2). Mitral annulus tissue Doppler. This image is related to (2). The E/e’ ratio is 11.90. These patients usually have a slightly raised capillary pressure and occasional symptoms of stress dyspnea.
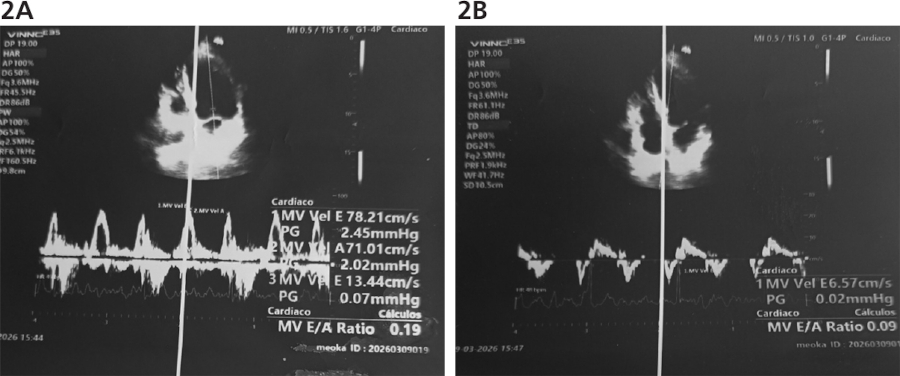
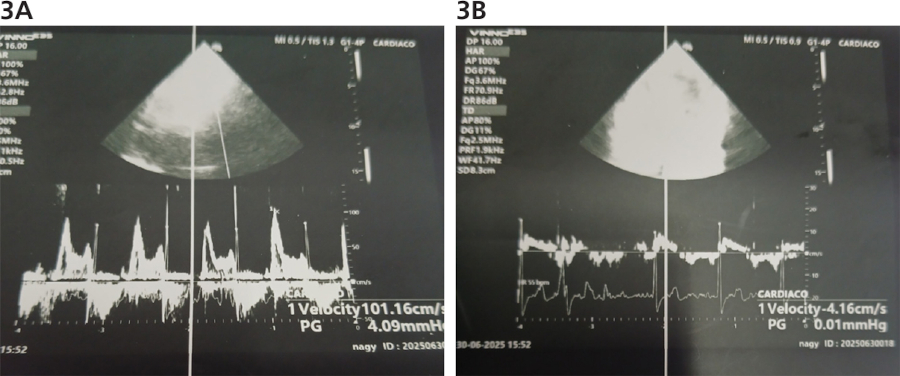
Fig. 3.
A.Severe diastolic dysfunction (grade 3). Altered ventricular compliance. The mitral flow pattern shows peak “E” velocity of 101 cm/s and peak A velocity of 33 cm/s, with an E/A ratio of 3.06. This pattern is observed in advanced or decompensated heart diseases. B. Severe diastolic dysfunction (grade 3). Mitral annulus tissue Doppler. e’ velocity is 4.16 cm/s and the E/e’ ratio is 24 , indicating high pulmonary capillary pressure. This pattern is observed in frequently symptomatic patients.
Statistical analysis
For descriptive statistics, quantitative data are presented as mean ± standard deviation (SD), and categorical data as frequency and percentage. Means in both groups were compared using Student’s t-test, and proportions were compared using the chi-square test. A p-value <0.05 was considered statistically significant. Univariate associations are expressed as odds ratios (OR) with their respective 95% confidence intervals (95% CI). A multiple logistic regression analysis was performed in which significant diastolic dysfunction (moderate or severe) was the dependent variable, and the following predefined variables were included in the model: advanced age (over 73 years), male sex, diabetes, hypertension, dyslipidemia, and smoking. A multiple regression analysis was also performed in which GLS was the dependent variable and diabetes, hypertension, male sex, age, dyslipidemia, and smoking were the independent variables.
RESULTS
A total of 1384 patients were evaluated in the stress echocardiography unit between March 2023 and December 2025; of these, 437 were excluded from the analysis due to oronary artery disease. A total of 947 patients with a mean age of 73 ± 6 years were included, 176 of which had diabetes (18.5%). The demographic characteristics and risk factors of patients with and without DM are presented in Table 1.
Table 1
Population characteristics
| Variables | DM (n=176, 18,5%) | No DM (n=771, 81,5%) | p |
|---|---|---|---|
| Age, years, mean ± SD | 72 ± 7 | 73 ± 6 | 0.270 |
| Male sex, n (%) | 73 (41.5) | 208 (27.0) | <0.001 |
| Hypertension, n (%) | 147 (83.5) | 521 (67.6) | <0.001 |
| DLP, n (%) | 83 (47,2) | 301 (39,0) | 0,047 |
| TS or ex-TS, n (%) | 87 (49,4) | 245 (31,8) | 0,001 |
DLP: dyslipidemia; DM: diabetes; TS: tobacco smoker.
The group with DM consisted of a higher number of male patients and a greater incidence of hypertension, dyslipidemia, and smokers. The prevalence of moderate or severe diastolic dysfunction was significantly higher in the diabetic group, both at rest and immediately post-exercise. In addition, patients with DM had a significantly higher E/e’ ratio both at rest and post-exercise due to a lower e’. There were no significant differences in LVEF at rest or immediately after exercise, and the GLS at rest was significantly lower in diabetic patients. (Table 2).
Table 2
Echocardiographic parameters of systolic function, diastolic function, and strain in diabetic and non-diabetic patients
| Parameters | DM (n=176, 18.5%) | No-DM (n=771, 81.5%) | p |
|---|---|---|---|
| Resting LVEF, % | 59 ± 8 | 60 ± 7 | 0.255 |
| Exercise LVEF, % | 68 ± 9 | 69 ± 7 | 0.240 |
| Resting peak E velocity, m/s | 0.69 ± 0.20 | 0.67 ± 0.20 | 0.318 |
| Resting peak e´ velocity, m/s | 0.061 ± 0.011 | 0.065 ± 0.012 | <0.001 |
| Resting E/e´ ratio | 12.4 ± 1.1 | 10.9 ± 5.5 | <0.001 |
| Exercise peak stress E velocity, m/s | 0.88 ± 0.2 | 0.85 ± 0.2 | 0.018 |
| Exercise peak stress e' velocity, m/s | 0.071 ± 0.03 | 0.074 ± 0.02 | 0.640 |
| Exercise E/e´ ratio | 13.9 ± 8 | 12.1 ± 5 | <0.001 |
| Global longitudinal strain, % | -15.20 | -16.21 | <0.001 |
| Resting diastolic dysfunction, n (%) | 22 (12.5) | 55 (7.1) | <0.001 |
| Exercise-induced diastolic dysfunction, n (%) | 62 (35) | 177 (23) | <0.001 |
LVEF: Left ventricular ejection fraction; DM: Diabetes mellitus
In a logistic regression model (in which diastolic dysfunction was the dependent variable and the independent variables were advanced age, male sex, diabetes, hypertension, dyslipidemia, and smoking), advanced age, diabetes, and male sex independently predicted moderate or severe diastolic dysfunction at rest. Advanced age, diabetes, and male sex also independently predicted moderate or severe diastolic dysfunction during exercise. (Tables 3 and 4)
Table 3
Prediction of resting diastolic dysfunction. Univariate and multivariate analysis.
| Independent variables | Univariate OR (95% CI) | p | Multivariate OR (95% CI) | p |
|---|---|---|---|---|
| Male | 2.28 (1.6–3.2) | 0.001 | 2.24 (1.54–3.26) | <0.001 |
| Advanced age | 1.48 (1.04–2.10) | 0.025 | 1.44 (1.00–2.05) | 0.045 |
| Diabetes | 1.90 (1.27–2.85) | <0.001 | 1.70 (1.11–2.59) | 0.013 |
| Hypertension | 1.56 (1.04–2.33) | 0.029 | 1.33 (0.87–2.01) | 0.177 |
| Dyslipidemia | 1.05 (0.73–1.49) | 0.658 | 1.11 (0.77–1.60) | 0.562 |
| Smoking | 0.94 (0.65–1.36) | 0.524 | 0.76 (0.52–1.13) | 0.188 |
Table 4
Prediction of moderate-to-severe exercise-induced diastolic dysfunction. Univariate and multivariate analysis.
| Independent variables | Univariate OR (95% CI) | p | Multivariate OR (95% CI) | p |
|---|---|---|---|---|
| Male | 3.5 (1.75–7) | <0.001 | 3.03 (1.45–6.32) | 0.003 |
| Advanced age | 2.45 (1.18–5.07) | 0.015 | 2.42 (1.15–5.10) | 0.019 |
| Diabetes | 3.93 (1.97–7.84) | <0.001 | 3.31 (1.60–6.85) | 0.001 |
| Hypertension | 1.78 (0.77–4.14) | 0.280 | 1.27 (0.53–3.04) | 0.590 |
| Dyslipidemia | 1.16 (0.58–2.31) | 0.781 | 1.23 (0.60–2.52) | 0.555 |
| Smoking | 1.25 (0.62–2.50) | 0.765 | 0.86 (0.41–1.82) | 0.700 |
Global longitudinal strain was significantly reduced in diabetic patients (Table 2), and in a multiple regression analysis, diabetes (p=0.031), hypertension (p<0.001), and male sex (p=0.013) were independent predictors of GLS, whereas age, dyslipidemia, and smoking were not.
DISCUSSION
Our case series includes a group of elderly patients with type 2 DM and without coronary artery disease. Although there were no inclusion or exclusion criteria in the study that specifically addressed age, it is justified to consider the population as elderly given their mean age of 73 years and the fact that 95% of patients were over 60 years of age.
We found that these patients did not have significant abnormalities in left ventricular systolic function as assessed by LVEF at rest and during exercise, although in some studies the LVEF of diabetic patients is found to be slightly reduced. (10) On the other hand, several parameters of diastolic function were consistently significantly altered in this group of diabetic patients, and there was also a significant reduction in GLS, indicating an abnormal myocardial fiber function. (11)
The pathophysiological mechanisms implicated in diabetic cardiomyopathy (3–12) include impaired cardiac insulin signaling, mitochondrial dysfunction, increased oxidative stress, reduced nitric oxide availability, elevated advanced glycation end products, impaired myocardial calcium handling, inflammation, activation of the renin-angiotensin-aldosterone system, cardiac autonomic neuropathy, and microvascular dysfunction. (13,14)
Although there was a difference in the prevalence of other risk factors in the group of diabetic patients (more hypertension, dyslipidemia, and smoking), the multivariate analysis showed that DM is independently associated with diastolic function, as are advanced age and male sex, but not the other factors mentioned. Diabetes mellitus was also independently associated with GLS.
Moderate or severe diastolic dysfunction at rest was found in 12.5% of diabetic patients, and moderate to severe diastolic dysfunction during exercise in 35%. It is known that exercise can reveal greater degrees of diastolic dysfunction, that is, a lower functional reserve of diastolic function.
Based on these findings, we conclude that our observations support the existence of cardiomyopathy with diastolic dysfunction in a small but statistically significant group of diabetic patients studied, and that diabetes is a determinant of this condition. This finding is consistent with several previously published series. (15)
In our study, this cardiomyopathy is characterized by preserved LVEF at rest and during exercise, and a mild but significant decrease in GLS, in addition to altered diastolic parameters on Doppler, consistent with several published series. (16)
In contrast, only one diabetic patient in our series presented with a low LVEF (systolic dysfunction), demonstrating a very low prevalence of diabetic-related systolic dysfunction in our series (it should be noted that patients with ischemic heart disease were excluded). The term “diabetic cardiomyopathy” was initially introduced based on postmortem findings in four diabetic adults with heart failure in the absence of coronary artery disease. (17) This condition —diabetic dilated cardiomyopathy in the absence of coronary artery disease— is described in case series, but its existence is more controversial. (18)
In summary, based on previous publications and the results of our study, we can conclude that diabetic cardiomyopathy with isolated diastolic dysfunction is relatively common in asymptomatic elderly diabetics, but that the prevalence of diabetic dilated cardiomyopathy, whose existence is controversial, is very low, if it exists at all. This diastolic dysfunction in diabetic patients, beyond the presence of coronary artery disease, is associated with a higher incidence of heart failure in this population. Although the risk of heart failure is thought to be higher in diabetic women, in our study, male sex was associated with the presence of significant diastolic dysfunction. The significance of this finding is unclear, but it could be explained by the fact that diastolic dysfunction is not synonymous with diastolic heart failure.
Limitations
Our case series was limited to elderly patients with type 2 diabetes. Moreover, cardiomyopathy as a complication of type 1 diabetes is a condition of very low prevalence. (19)
The cross-sectional nature of our study does not allow us to draw conclusions regarding the development of heart failure during the course of this diastolic dysfunction, which is evident at rest and during exercise in a subgroup of diabetic patients. It has been described that more than one factor is involved in the development of heart failure in diabetics, some of which are extra myocardial, such as the phenomenon of hyperfiltration and increased blood volume in these patients. (20) Prospective follow-up of these patients would be necessary to clarify the prognostic significance of diastolic dysfunction in elderly diabetic patients.