
INTRODUCTION
Over the past few decades, significant advances have been made in the prevention, diagnosis, and treatment of cardiovascular diseases (CVDs). However, they remain the leading cause of death in both men and women. There are aspects of the pathophysiology, clinical presentation, and outcome of coronary artery disease (CAD) and peripheral vascular disease that are specifically linked to women and associated with pregnancy and hormone levels. Also, sociocultural factors influence gender concepts and their comprehensive impact on health. (1)
International and national registries show that the differences persist in the diagnosis, management, and outcome of women with acute myocardial infarction (AMI), which results in higher mortality in this group of patients.
Various studies evidence that women presenting with AMI are older, have a higher prevalence of risk factors such as hypertension (HTN), diabetes mellitus (DM), central obesity, and dyslipidemia (DLP). Women also experience atypical symptoms such as dyspnea, nausea, or epigastric pain, which can delay diagnosis and treatment initiation. (2) Furthermore, women are less likely to receive the recommended invasive and pharmacological therapies, thus contributing to higher in-hospital mortality and worse short- and long-term outcomes.
In recent years, there has been an increased focus on recognizing the significance of CVD in women and gender-related risk factors. This has led to a deeper understanding of these differences and greater visibility. Educational campaigns have been launched to raise awareness among the general population and the medical community, focused on promoting a more appropriate approach to these patients. It is imperative to properly understand the differences in the presentation of CVD in women to implement the most appropriate prevention, diagnosis, and treatment measures.
However, challenges persist. Women often delay seeking medical care during an AMI, partly due to a lack of awareness, downplaying of atypical symptoms, or sociocultural barriers.
The need to investigate this topic stems from the desire to reduce these disparities and improve patient outcomes. One way to delve deeper into this issue is to highlight the progress made over time and acknowledge what remains to be achieved. The aim of this study was to compare the clinical characteristics, management and in-hospital outcome of women with STEMI in Argentina over the past 20 years.
METHODS
This retrospective, observational, and multicenter study in Argentina was based on data from the 2005 Argentine Society of Cardiology (SAC) AMI registry (3) and the ARGEN-IAM-ST registries conducted in 2015 and 2024. (4,5) A total of 2620 ST-segment elevation myocardial infarction (STEMI) patients were included: 505 patients in 2005, 1739 patients in 2015, and 376 patients in 2024. Informed consent was not required due to the retrospective design of the study.
The clinical characteristics of the included patients, coronary risk factors, presentation and time patterns, treatment modalities, and in-hospital outcome were analyzed and compared according to sex. Changes that have occurred over the past 20 years were also analyzed.
Qualitative variables are presented as frequencies and percentages. Quantitative variables are expressed as mean ± standard deviation (SD), or median and interquartile range (IQR 25-75), according to their distribution.
Discrete variables were analyzed using contingency tables. For continuous variables, the t-test, the Kruskal-Wallis test for unmatched groups, or analysis of variance (ANOVA) were used, as appropriate. The chi-square test for trend was used to analyze changes across the three registries. A pvalue < 0.05 was considered statistically significant. All the calculations were performed using Epi-Info 7.2.2.6 software package. RESULTS
A total of 2620 patients were analyzed. The percentage of women in each group was 24.5%, 22.7%, and 20.7%, respectively (p = 0.182). The characteristics of the population by year are summarized in Table 1.
Table 1
General characteristics of the study population
| Year | 2005 | 2015 | 2024 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Total | 505 | 1739 | 376 | |||||||||
| Men | Women | Men | Women | Men | Women | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| N | 381 | 75.5 | 124 | 24.5 | 1344 | 77.3 | 395 | 22.7 | 298 | 79.3 | 78 | 20.7 |
| Age (years) | 60.5 ± 12.8 | 71.3 ± 13.4 | 59.8 ± 11.1 | 66.3 ± 13.3 | 60.0 ± 11.7 | 65.6 ± 13.2 | ||||||
| p<0.001 | p<0.001 | p<0.001 | ||||||||||
| HTN | 243 | 63.8 | 99 | 79.8 | 727 | 54.1 | 276 | 69.9 | 163 | 54.7 | 49 | 62.8 |
| p<0.001 | p<0.001 | p=0.191 | ||||||||||
| DM | 73 | 19.2 | 27 | 21.8 | 633 | 47.1 | 148 | 36.7 | 84 | 28.2 | 24 | 30.8 |
| p=0.523 | p<0.001 | p=0.652 | ||||||||||
| DLP | - | - | 501 | 37.3 | 168 | 42.5 | 126 | 42.3 | 33 | 42.3 | ||
| p=0.059 | p=1 | |||||||||||
| Tobacco | 191 | 50.1 | 37 | 29.8 | ND | ND | 169 | 56.7 | 38 | 48.7 | ||
| p<0.001 | p=0.205 | |||||||||||
| Prior CAD | 108 | 28.4 | 34 | 27.4 | 182 | 13.5 | 41 | 10.4 | 48 | 16.1 | 7 | 8.9 |
| p=0.847 | p=0.095 | p=0.113 | ||||||||||
CAD: coronary artery disease; DLP: dyslipidemia; DM: diabetes mellitus; HTN: hypertension; N/A: not available
The median age of women decreased over the years: 71.3 vs. 66.3 vs. 65.6 years, respectively (p = 0.049).
Among women, HTN was the most prevalent coronary risk factor, with a reduction over the years (79.8% vs 69.9% vs 62.8%, respectively; p = 0.006).
The prevalence of DM exhibited a marked upward trend, with percentages of 21.8%, 36.7%, and 30.8%, respectively (p = 0.063).
The prevalence of tobacco use also increased significantly, from 29.8% to 48.7% (p = 0.007).
A history of CAD decreased from 27.4% to 10.4% and 8.9%, respectively (p < 0.001), likely related to changes in the age of AMI presentation.
Delays in consultation exhibited a marked improvement, with a reduction from 320 minutes to 180 minutes and 190 minutes. respectively (p < 0.001) (Table 2).
Table 2
Characteristics of AMI, treatment modality, and in-hospital outcome
| Year | 2005 | 2015 | 2024 | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Men | Women | Men | Women | Men | Women | |||||||
| n | % | n | % | n | % | n | % | n | % | n | % | |
| Delay (min) | 240 (120-630) | 320 (180-720) | 168 (60-420) | 180 (75-420) | 225 (90-490) | 190 (95-424) | ||||||
| p=0.101 | p=0.402 | p=0.602 | ||||||||||
| Anteriro wall AMI | 157 | 44.2 | 43 | 37.7 | 654 | 52.2 | 197 | 52.0 | 148 | 49.6 | 45 | 57.7 |
| p=0.221 | p=0.929 | p=0.206 | ||||||||||
| Inferior wall AMI | 100 | 28.2 | 34 | 29.8 | 595 | 47.5 | 180 | 47.5 | 137 | 46 | 30 | 38.5 |
| p=0.733 | p=0.992 | p=0.234 | ||||||||||
| Reporfusion YES | 216 | 56.7 | 55 | 44.4 | 1145 | 85.5 | 316 | 80 | 287 | 96.3 | 74 | 94.9 |
| p=0.017 | p=0.013 | p=0.568 | ||||||||||
| Primary PCI | 135 | 35.4 | 30 | 24.2 | 851 | 74.3 | 250 | 79.1 | 230 | 80.1 | 60 | 81.1 |
| p=0.023 | p=0.076 | p=0.857 | ||||||||||
| FBL | 89 | 23.4 | 26 | 21 | 253 | 22.1 | 61 | 19.3 | 50 | 17.4 | 9 | 12.2 |
| p=0.581 | p=0.284 | p=0.271 | ||||||||||
| KK I | 295 | 78.5 | 90 | 75.6 | 1005 | 77.7 | 276 | 72.1 | 242 | 81.2 | 51 | 65.4 |
| KK II | 56 | 14.9 | 15 | 12.6 | 183 | 14.1 | 68 | 17.8 | 25 | 8.4 | 8 | 10.3 |
| KK III | 12 | 3.2 | 8 | 6.7 | 25 | 1.9 | 14 | 3.7 | 9 | 3 | 3 | 3.8 |
| KK IV | 13 | 3.5 | 6 | 5 | 81 | 6.3 | 25 | 3.5 | 22 | 7.4 | 16 | 20.5 |
| p=0.276 | p=0.055 | p=0.004 | ||||||||||
| HF on admission | 81 | 21.5 | 29 | 24.4 | 289 | 22.3 | 107 | 27.9 | 56 | 18.8 | 27 | 34.6 |
| p=0.525 | p=0.023 | p=0.003 | ||||||||||
| IH mort | 46 | 12.1 | 19 | 15.3 | 106 | 7.9 | 43 | 10.9 | 22 | 7.4 | 5 | 6.4 |
| p=0.342 | p=0.061 | p=0.774 | ||||||||||
AMI: acute myocardial infarction; FBL: fibrinolysis; HF: heart failure; IH mort.: in-hospital mortality; KK: Killip and Kimball; PCI: percutaneous coronary intervention
The prevalence of anterior wall infarctions increased significantly, rising from 37.7% to 51.9% and 57.7%, respectively (p < 0.001).
There was a significant increase in reperfusion therapy in women: 44.4% vs. 80% vs. 94.9%, respectively (p trend < 0.001). The rate of primary percutaneous coronary intervention was 24.2% vs 79.1% vs 81.1%, respectively (p < 0.001).
There was a non-significant decrease in the rate of Killip and Kimball (KK) class I (75.6%, 72.1%, and 65.4%, respectively) patients and a significant increase in KK class IV patients (5%, 3.5%, and 20.5%, respectively; p < 0.001).
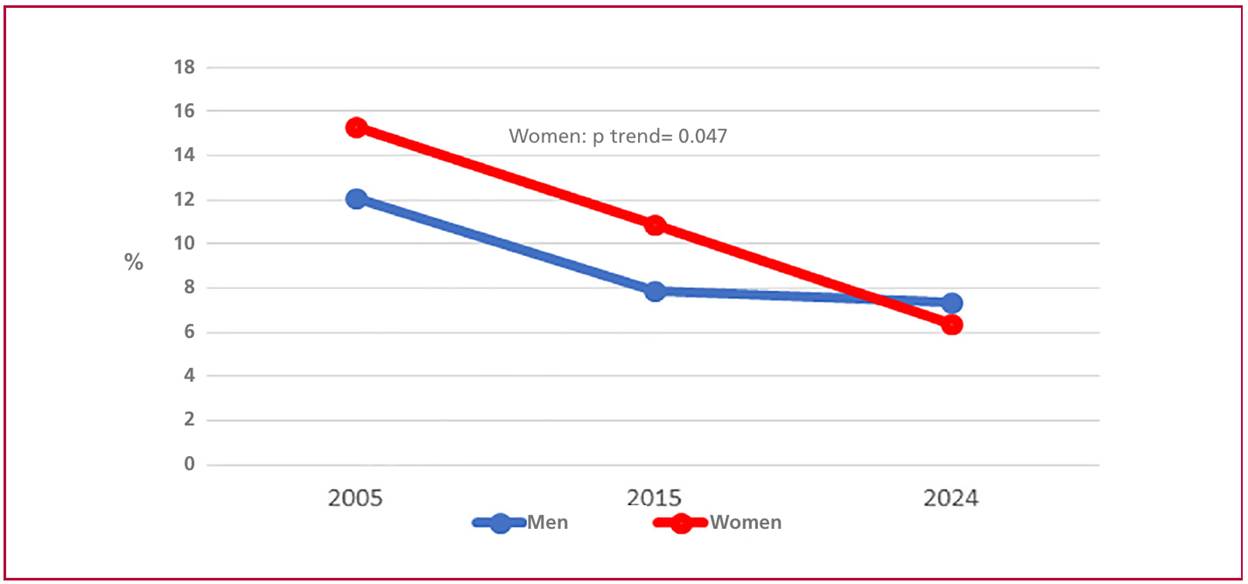
In-hospital mortality decreased over the years, from 15.3% to 10.9%, and 6.4%, respectively (p = 0.047). Compared with men, the difference was not significant in 2005 (15.3% vs. 12.1%; p = 0.342), tended to be higher in 2015 (10.9% vs. 7.9%; p = 0.061), and there were no differences in 2024 (p = 0.774) (Figure 1).
DISCUSSION
In this study of 2620 patients, the percentage of women remained relatively stable, while the median age at presentation decreased significantly. There were notable changes in the prevalence of risk factors. Hypertension decreased, while DM and tobacco use increased. The prevalence of prior CAD exhibited a marked reduction. Additionally, time to consultation improved, and reperfusion therapy and primary percutaneous coronary intervention rates increased significantly. In-hospital mortality in women showed a downward trend, becoming comparable to that of men in the most recent period.
These results are relevant because they reflect the epidemiological and clinical transition of AMI in the female population. The decrease in age at presentation and the rise in the prevalence of hypertension, in conjunction with the rise in DM and tobacco use, indicate a shift in the risk profile. This finding is consistent with international reports emphasizing the mounting significance of DM and tobacco use in young women. The higher rates in reperfusion therapy and primary percutaneous coronary intervention represent a significant advance, as historically women received fewer invasive interventions. (6) In this setting, the reduction in in-hospital mortality to levels comparable to those of men is a positive and rare finding in the literature, where female mortality is typically higher. (7,8)
There is a growing recognition that the pathophysiology and clinical manifestations of CAD differ between men and women. Women are more likely to present with non-ST-segment elevation acute coronary syndromes (NSTE-ACS) and non-obstructive ischemic heart disease, such as vasospasm or spontaneous coronary dissection, whereas obstructive CAD is more prevalent in men. (9,10)
Although typical angina remains the most common presentation of ACS in both sexes, up to one-third of patients do not present with typical symptoms, with atypical presentation being more common in women than in men (37% vs. 27%). Among women < 45 years, AMI most often presents without typical angina and is associated with a higher in-hospital mortality. (11,12)
Although other publications have reported that women with ACS are older, (13) in this study median age at presentation decreased significantly over the years, although the percentage of women who suffered an AMI remained relatively stable.
The prevalence of traditional coronary risk factors (CRFs) is higher in older women, while those < 65 years have higher prevalence of non-traditional CRFs, as family history, complications of pregnancy and childbirth, early menopause, emotional stress, depression, and chronic inflammatory diseases. (14-16)
Both men and women smokers have higher relative risk of presenting an AMI. Tobacco use was reported as the most significant risk factor in young women. It has even been suggested that women may be more susceptible than men to the effects of tobacco. (17,18)
Microvascular and macrovascular dysfunction, as well as atherosclerotic disease, are significant pathophysiologic mechanisms in women; the etiology of myocardial infarction is more heterogeneous than in men and varies with age. Plaque rupture with thrombosis is the cause of fatal AMI in 76% of men and 55% of women. (19) In women < 65 years, up to 50% of ACS cases present with angiographically normal coronary arteries. In this population, plaque erosion is more prevalent, resulting in ischemia due to distal embolism and endothelial dysfunction. These mechanisms often remain undetectable by conventional angiography, leading to the erroneous conclusion that atherosclerotic disease is not present. (20) Women have a higher prevalence of MINOCA (myocardial infarction with non-obstructive coronary arteries). This condition, which involves multiple pathophysiological mechanisms, has a reported annual mortality rate of approximately 2%, and an increased risk of recurrent myocardial infarction, heart failure, stroke, and longterm cardiovascular events, as well as higher mortality and hospital readmission rates. (21-23).
The recommendations for the management of ACS are the same for both sexes; however, it has been reported that women tend to delay seeking medical care and, in general, receive fewer treatments recommended by the guidelines. (24) Women are more likely to present with nonspecific prodromal symptoms, such as anxiety, sleep disturbances, and unusual fatigue prior to the onset of ACS. Misinterpreting these symptoms could lead to a delay in patient evaluation. (25 )
The comparative analysis of this study revealed that time to consultation improved, and reperfusion therapy and primary percutaneous coronary intervention rates significantly increased.
Like international registries, in-hospital mortality from STEMI is higher among women than men in Argentina. (26) Nevertheless, some studies from European countries and the United States did not report the same results, with higher rates of mortality and major cardiovascular events in men, which is probably due to a higher prevalence of comorbidities. (27)
In young women, mortality is twice that of men. (28) The age of patients diagnosed with AMI has been decreasing in recent years, likely due to the higher prevalence of tobacco use, among other causes. (29)
This comparative analysis revealed that in-hospital mortality for women decreased over time, reaching a level comparable to that of men in the most recent period. This was observed despite a higher rate of KK class IV cases, probably due to the high reperfusion rates recorded in recent years.
It is important to note that these results reflect the situation of AMI in women in our country over the years. Although the number of patients recorded in 2024 is the lowest in the ARGEN-IAM-ST registry, the percentage of women remains stable, providing an accurate representation of the situation. The ARGENIAM-ST registry is the only independent tool open to the scientific community that facilitates a discussion of the reality of AMI in Argentina. (30)
CONCLUSION
The clinical characteristics of women admitted for AMI in Argentina over a 20-year period have changed.
Women are gradually younger, less likely to have HTN, but more likely to be diabetics and to smoke, and with a lower incidence of a history of CAD.
There was a significant reduction in the time to presentation, along with an increase in the frequency of prior myocardial infarction. The rates of reperfusion therapy and primary percutaneous coronary intervention rose significantly, reaching levels similar to those in men. This translates into a significant decrease in in-hospital mortality among women with AMI, despite an increase in the prevalence of heart failure during hospitalization.
These findings underscore the need to continue promoting specific strategies for the prevention and care of AMI in women in Argentina.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).