Jorge Trainini1, MTSAC, Mario Wernicke2, Mario Beraudo3, Marta Cohen4, Alejandro Trainini1, 3, María Elena Bastarrica3, Benjamín Elencwajg1, Jorge Lowenstein5, MTSAC, Alejandro Ventura6
1 Hospital Presidente Perón, Buenos Aires, Argentina. Universidad Nacional de Avellaneda, Argentina.
2 Departamento de Anatomía Patológica, Clínica Güemes, Luján, Buenos Aires, Argentina.
3 Departamento de Cirugía Cardíaca, Clínica Güemes, Luján, Buenos Aires, Argentina.
4 Departamento de Histopatología Sheffield Children’s NHS FT, Reino Unido.
5 Departamento de Cardiología, Investigaciones Médicas, Buenos Aires, Argentina.
6 Cordis-Instituto del Corazón, Resistencia, Chaco, Argentina
Address for reprints: Jorge Carlos Trainini. E-mail: jctrainini@hotmail.com
Rev Argent Cardiol 2023;91:449-455. http://dx.doi.org/10.7775/rac.es.v91.i6.20722
ABSTRACT
Background: The functional anatomy of the helical, continuous myocardium allows envisioning that it initiates and ends at the origin of the great vessels. In our research, we have always considered that it should have a point of attachment to allow its helical rotation to fulfill the fundamental movements of shortening-torsion (systole) and lengthening-detorsion (suction), which once found, was called the cardiac fulcrum.
Objectives: The research aims to describe the important aspect of understanding the interrelationship between the cardiac fulcrum and the Aschoff-Tawara atrioventricular node
Material and Methods:: : A total of 31 hearts, arising from the morgue and slaughterhouse were used: 17 corresponded to bovids and 14 were human.
Results: Our investigations have shown that the myocardial support termed cardiac fulcrum, located in the trajectory of the aortic annulus septal segment, extending from the left to the right trigone and below the origin of the right coronary artery, is adjacent to the AV node. Another important aspect of this contiguous position is that the fulcrum is surrounded, and even invaded, by a rich nervous plexus interconnected with the node.
Conclusion: This description of the cardiac fulcrum would end the problem of lack of support of the myocardium to fulfill its function of torsion/detorsion. The proximity of the fulcrum to the AV node and the penetration of the nervous plexuses in the support suggest an electromechanical unit, which we have investigated according to the helical anatomy of the heart, establishing an improved cardiac stimulation with a catheter placed in the right ventricular outflow tract.
Key words: Cardiac Anatomy - Myocardium - Cardiac Fulcrum - Myocardial Support - AV node
RESUMEN
Introducción: El estudio de la anatomía funcional del miocardio helicoidal continuo permite visualizar su inicio y fin en el nacimiento de los grandes vasos. En nuestras investigaciones siempre hemos considerado que debía tener un punto de unión que permitiera su rotación helicoidal para cumplir los movimientos fundamentales de acortamiento-torsión (sístole) y alargamiento-destorsión (succión). Una vez encontrado, se le llamó fulcro cardíaco.
Objetivos: Esta investigación tiene como objeto describir y entender la interrelación entre el fulcro cardíaco y el nódulo auriculoventricular de Aschoff-Tawara
Material y métodos: Se utilizaron 31 corazones procedentes de la morgue y del matadero: 17 correspondieron a bóvidos y 14 a seres humanos.
Resultados: En nuestras investigaciones hemos demostrado que el soporte del miocardio, denominado fulcro cardíaco, que se localiza en el trayecto del segmento septal del anillo aórtico y se extiende desde el trígono izquierdo hasta el derecho por debajo del origen de la arteria coronaria derecha, es adyacente al nódulo auriculoventricular (AV). Otro aspecto importante de esta posición contigua es que el fulcro está rodeado, e incluso invadido, por un plexo nervioso interconectado con el nódulo.
Conclusión: Esta descripción del fulcro cardíaco pondría fin al problema de la falta de apoyo del miocardio para cumplir su función de torsión/destorsión. La proximidad del fulcro al nódulo AV y la penetración de los plexos nerviosos en el apoyo indican la existencia de una unidad electromecánica, que hemos investigado en función de la anatomía helicoidal del corazón. Hemos comprobado una mejor estimulación cardíaca cuando el catéter se coloca en el infundíbulo ventricular derecho.
Palabras clave: Anatomía cardíaca - Miocardio - Fulcro cardíaco - Soporte miocárdico - Nódulo AV
Received: 05/27/2023
Accepted: 11/03/2023
INTRODUCTION
Previous investigations from our group have shown the presence of a myocardial support which we have named cardiac fulcrum, located in the course of the aortic annulus septal segment, extending from the left to the right trigone (below the origin of the right coronary artery). The origin and end of the myocardium attaches in this site, since as every muscle it needs a support to fulfill its function. (1,2)
When we found the anatomical contiguity of the fulcrum with the Aschoff-Tawara nodule, we set out to analyze the anatomical and histological relationship of the cardiac fulcrum with the atrioventricular node in a group of human and bovids hearts, as well as the possible functionality between both structures.
In human hearts, to demonstrate this relationship, we worked with hearts of fetuses, children and adults.
METHODS
A total of 31 hearts, coming from the morgue and slaughterhouse were used: 17 corresponded to 2-year-old bovids (10 males and 7 females), weighing 800-1000 g and b) 14 were human (8 males and 6 females), two from 16 and 23-weekold fetuses, three from 36-day, 10-week and 27-week-old infants, one from a 4-year-old boy, one from a 10-year-old boy weighing 116 g and seven from adults weighing 300 g.
Anatomical and histological studies were performed. The heart was fixed in 10% buffered formalin. Hematoxylineosin, Masson’s trichrome staining technique and 4-micron sections were used for the histological study, and 10 % formalin was used as buffer. Immunohistochemistry was also carried out (s100-neurofilaments). (3)
Since the material corresponds to morgue and slaughterhouse pieces, no ethical approval was needed.
The single continuous and helical myocardium was deployed according to a previously published technique. (1,4)
A fundamental concept at the beginning of deployment must be followed, as any attempt at not respecting in the dissection the axes where the myocardium coils as a helix, elicits the myocardial mass rupture. The concurrence of the cardiac muscle origin and end in the cardiac fulcrum constitutes a meeting point between the right segment and the ascending segment, origin and end of the myocardium (Figure 1). Thus, both ends are situated in the same site, with the origin of the myocardial fibers placed in an anterior plane to those of its end. Samples of the atrioventricular (AV) node and His bundle were obtained in Koch’s triangle.
RESULTS
The anatomical investigations have revealed that all the hearts (bovids and humans) have a myocardial support whose histological structure in the analyzed specimens presents with an osseous or chondroidtendinous character. In this structure are inserted the myocardial fibers at the origin and end of the band, which correspond to the continuous myocardium coiled as a helix (Figure 2).
Location and relationships. The cardiac fulcrum is found in the proximity of the tricuspid valve (right) the aorta (superior) and the pulmonic-tricuspid cord (anterior). In order to localize it, it is necessary to shift the pulmonary artery and the right segment to the left of the observer, stripping the aortic root at the origin of the helical myocardium. This maneuver uncovers the fulcrum below the aorta and inferior and to the left of the right trigone, without any continuity with it, below the origin of the right coronary artery, detached from aortic continuity and located as a complementary element between the aorta and the myocardium.
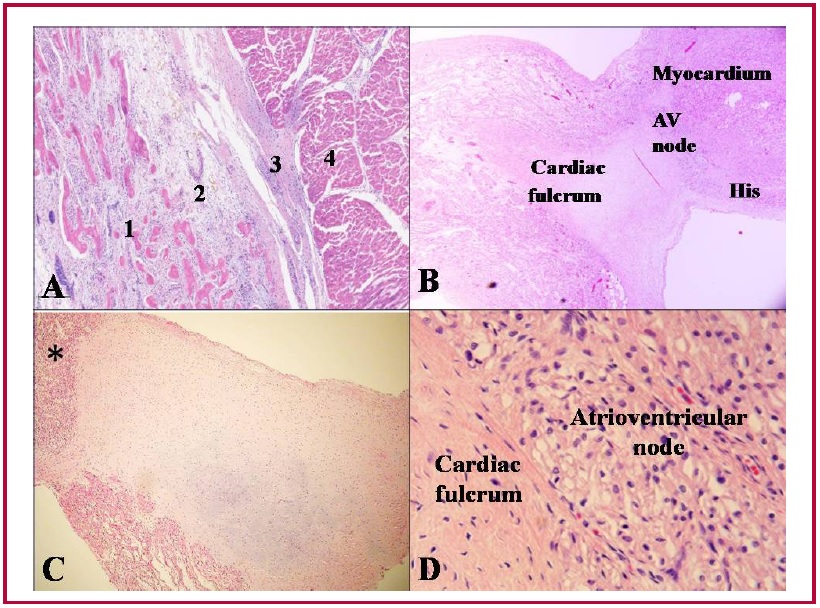
As it is situated in the atrioventricular junction at the insertion of the interventricular septum, below the aorta and the pulmonary artery, it is adjacent to the AV node, which is positioned at its right (Figure 3). The AV node is in the atrioventricular junction, at the base of the muscular septum, below the origin of the great vessels. It is adjacent to the cardiac fulcrum, placed between this and the implantation of the tricuspid septal leaflet. It constitutes a cluster of cells (specialized myocytes) that Rushmer defines as a spherical or bulbous end consisting of bundles of fibers
(5) that send the electrical impulses to the myocardial mass. In its continuity it is slowly transformed into the His bundle, whose course is short, and sometimes, even inexistent.
Histology. In bovids, the fulcrum is triangular. Its size, corroborated by dissection and imaging techniques, has an average of 37 mm in length, 45 mm in width and 15 mm in thickness. (2)
The microscopic analysis of the bovid cardiac fulcrum shows the presence of osseous trabeculae as a result of endochondral ossification. Its general structure resembles the metaphyseal growth of long bones. It is possible to observe osseous trabeculae with osteoblasts and segmental lines secondary to osseous apposition. The same histological findings have been encountered in the rest of the mammals. (6)
In the 10-year-old human heart, the description of the cardiac fulcrum is related with this early age, as it shows evidence of a central area of the fulcrum formed by chondroid tissue. Given the age, it is logical that its size is smaller. This finding was repeated in the 23-week-old human fetus with the characteristic prechondroid bluish areas in a myxoid stroma and in the heart of the 36-day newborn.
The histological analysis of the adult human heart fulcrum (average size of 25 mm in length and 15 mm in width) revealed a chondroid-tendinous matrix. In principle, similar evidence of detection, localization and morphology of the fulcrum has been found in all the analyzed hearts, both human and bovid. They present myocardial insertion in the rigid fulcrum structure, forming a cardiomyocytic matrix unit, independently of their osseous, cartilaginous, or tendinous nature in the different specimens studied. This point of attachment implies exerting as in any muscle the supporting function of muscular lever and also to act as bearing or pad, preventing that the ventricular rotation force, either by torque or torsion effort is transferred to the aorta. Thus, it dissipates the energy produced by the helical muscle movement and avoids the strangulation or bending of the artery during the systolic ejective period.
Insertion. The histology of the fulcrum, of collagen- cartilaginous nature, determines the need of an additional analysis to understand its function. In every heart and in all the histological analyses we have verified the insertion of the myocardium in the fulcrum, a finding that becomes a strong point of reasoning to understand the function of the cardiac fulcrum in its biomechanical action of torsion-detorsion. In all the hearts analyzed we found this attachment of the myocardium in the rigid structure of the fulcrum according to the studies carried out during this investigation.
To establish the identity of the cardiac fulcrum, a histological analysis was also performed on the trigones, trying to find cardiomyocytes in their composition as a possible insertion of the cardiac muscle in these structures. Our research only showed collagenous tissue without cardiomyocytes in the trigones, confirming that the fulcrum is the support of the myocardium, both at its origin and end.
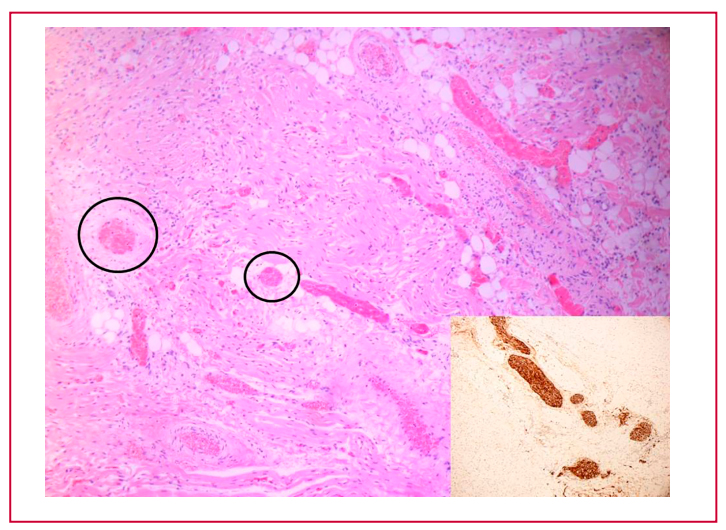
Relationship of the cardiac fulcrum with the AV node. This investigation reveals, both in human and bovid hearts, an important topic for cardiac stimulation therapeutics. In the histological study the fulcrum was found adjacent to the AV node, forming a rich cellular accumulation of plexuses with neurofilaments. This contiguity between both structures was obtained in all the specimens studied, both in bovid and human hearts. The essential point for the analysis is that the neurofilaments (Figure 4) are also found inside the cardiac fulcrum.
Fig. 1.Adult human heart. The ascending segment is seen inserting into the cardiac fulcrum. LA: left atrium; RA: right atrium; PA: pulmonary artery; RV: right ventricle. A: Cardiac fulcrum in a ten-year-old human heart. B: Cardiac fulcrum in the heart of a human embryo (23 weeks of gestation). C: Fulcrum resected from an adult human heart.
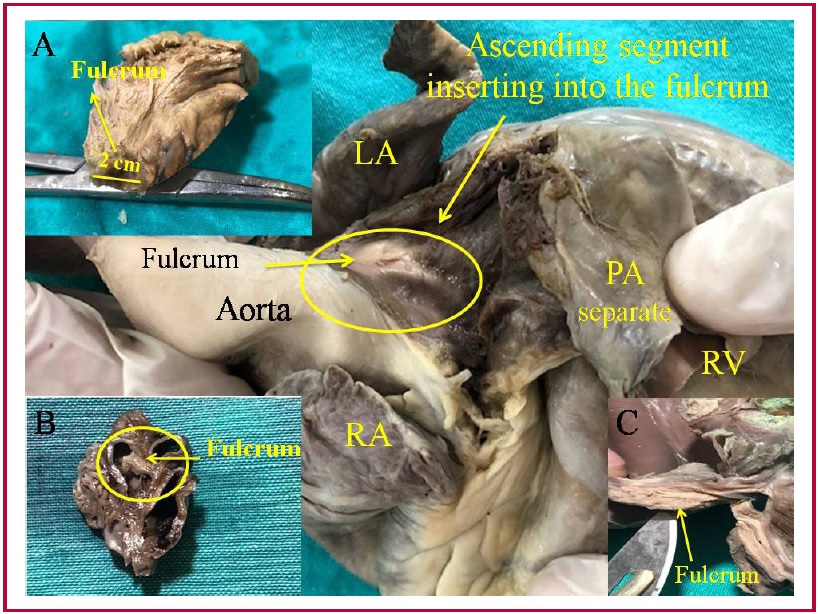
Fig. 2.Cardiomyocytes penetrating the fibrocollagen tissue of the cardiac fulcrum. 1. Cardiomyocytes; 2. Fibrocollagenous matrix (adult human heart). Insertion site is detailed in a circle. Hematoxylin- eosin technique (15x).
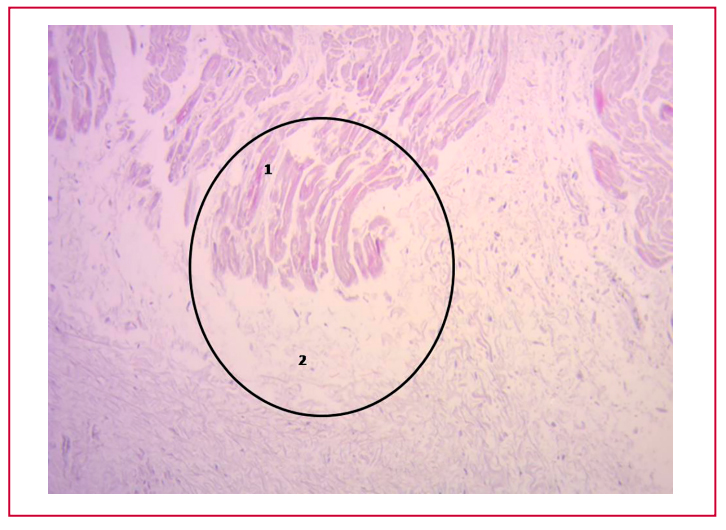
Fig. 3.A: Bovid heart, HEx25. Plexuses associated with fibrochondroid trabeculae and myocardium are observed. 1: bony trabeculae. 2: plexuses. 3: fibroconnective tissue. 4: myocardium. B: 36-day-old newborn human heart, 20x magnification. The cardiac fulcrum of cartilaginous matrix is observed with the myocardium and with the adjacent AV node. AV: Aschoff- Tawara atrioventricular node. C: 10-week infant heart. Cartilaginous cardiac fulcrum adjacent to the atrio-ventricular region (the asterisk indicates the AV node). H&E x100. D: Human heart. Fulcrum and Aschoff-Tawara AV node are seen in contiguity
DISCUSSION
Myocardial fibers constitute a single and continuous muscle that describes a double helix to form the walls of both ventricles. (4, 7, 8)
In order to fulfill its torsion-detorsion muscular function, it needs a point of support that we have found and called the cardiac fulcrum, to which itis attached at its origin and end, similarly to any other muscle. At this point there is an analogy between the skeletal muscle and the myocardium. The former performs its contraction between a fixed and a mobile point of support. This situation is found in the continuous myocardium, as there is greater solidity in the insertion between the fulcrum and the ascending segment in relation to the initial attachment of the right segment in that support.
From this experience, fundamental questions arise: why have we found that in fetus, infant, child, and adult human hearts, the cardiac fulcrum has cartilaginous characteristics, beyond that it fulfills the same function of attaching the helical myocardium that other species have? Let us bear in mind that the cartilage is the substrate for endochondral ossification, and although it does not always ossify, it is necessary to that end. Our interpretation is that perhaps the cardiac fulcrum with an osseous characteristic -as observed in bovids- is a vestigial organ typical of the evolution of mammals. A vestigial structure must be understood as the preservation during the “evolutionary” process of genetically established attributes which have lost all or part of their ancestral function in certain species. In this case, the osteo-cartilaginous histology identified in bovids refers to a cartilage-tendinous matrix which is sufficient to achieve myocardial insertion and attain a muscle power that is much lower than that of larger mammals. Let us recall that in in this investigation the bovid fulcrum is of osseus nature. (2)
The important fact that establishes the attachment of myocardial fibers to the cardiac fulcrum stems from both macroscopic and microscopic observation. Its conformation was confirmed by histology. We have called this structure, origin and end of the helical continuous myocardium, cardiac fulcrum, as a parallelism and tribute to the definition of the point of support acting as a lever expressed by Archimedes of Syracuse. It should be noted that in order to visualize the cardiac fulcrum it is essential to deploy the helical myocardium.
In 1669, Richard Lower considered that the myocardium was subjected to a torsional movement associated with the helical arrangement of its fibers. He expressed that the heart exerted a movement similar to "wringing a towel." Later, Henson (9) studied and verified this concept in mice. (1)
The heart achieves the ejection of its content through the torsion of its walls and initiates its filling by generating a negative pressure through detorsion. The synchronous torsional movement with longitudinal ventricular shortening can be explained by the helical arrangement and continuity of the cardiac muscle. (10-13)
The spatial arrangement of the continuous helical myocardium clearly indicates that the propulsion is given by its walls in the ventricular cavities that delimit these structures. Formed by the basal loops (right and left segments) and the apical loop (descending and ascending segments), the muscular unit they form are the walls of the ventricles, to which it provides propulsion power. (14-17)
Muscle homogenization masks the real spiral continuity of the fibers by the overlapping of its segments. Even the transverse interconnections between the tracts do not invalidate the concept of continuous myocardium, understanding that this compact arrangement is the result of the evolutionary development to obtain solidity in its structure in a strict relationship to its function. This implies considering that its structural strength is required in birds and mammals to ensure that blood is ejected at a high speed during a limited time, by an organ that must supply two circulations (systemic and pulmonary). The anatomical investigation of the heart through an adequate dissection (1), histological examination(2),
imaging analysis of radiological and echocardiographic studies (18-20), electrophysiological studies carried out with threedimensional electroanatomical mapping (8,21) and diffusion tensor cardiac magnetic resonance imaging (14,15) show the continuous muscular course that circumscribes the two ventricles.
The spatial helical arrangement of the myocardium forces the muscle to overlap segments. This anatomical situation has a profound correspondence with myocardial movements and with the stimulation that runs through its segments (21-23), according to the electrophysiological studies that we have previously carried out. (21,22) The interpretation of the anatomical relationship between the cardiac fulcrum and the AV node implies the complementarity of the anatomy with the physiology of the continuous helical myocardium, since the contiguity that they show is found in the point where the stimulation starts and ends, with the development of the mechanical action of torsion and detorsion in the ventricular systolic and suction phases.
The cardiac fulcrum, support and insertion of the myocardium to perform the lever function in its movements, is located adjacent to the Aschoff-Tawara AV node. Thus, an electromechanical unit located at the origin and end of the single helical myocardium is constituted. This anatomical and functional disposition of the myocardium is supported by a rich plexus of specialized filaments that interact with the mechanically working cardiomyocytes.
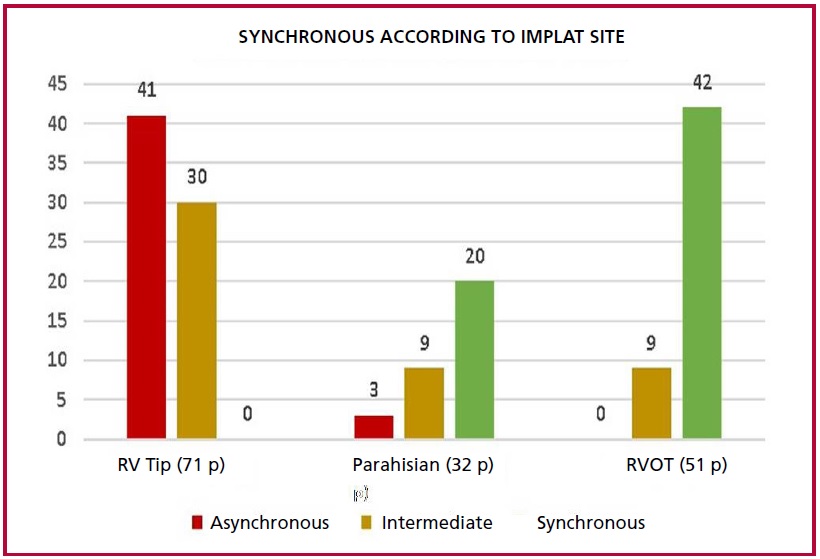
The interpretation of the findings in this research carried out in human and bovid hearts inevitably leads to therapeutic action. What is the explanation, according to our experience, why a better synchrony of pacemakers was evidenced with the catheter placed close to this electromechanical unit? The AV node is situated over the base of the muscular septum at the base of the tricuspid valve septal leaflet implantation, at the site of insertion of the interventricular septum with the aorta and the pulmonary artery. In this regard, the adjacency between the cardiac fulcrum and the origin of the continuous myocardium in its helical course in relation to the AV node, demonstrated that stimulation in the right ventricular outflow tract was more effective. In this experience with pacemakers implanted in different points of the right ventricle (tip, parahisian, outflow tract), using active standard fixation catheters, the right ventricular outflow tract achieved better electrical synchrony in the left ventricle (Figure 5). (24)
The ideal region for the location of the pacemaker stimulation catheter would be high in the outflow tract, below the pulmonary valve, and preferably on the septum, but not on the free wall.
Function leads the myocardium to have a point of support as any skeletal muscle, both at its origin and end. If the myocardium did not have this helical spatial anatomical conformation, with an insertion at both ends in the cardiac base remaining free at the apex, that is, as a pendulum in the thorax; and if it did not present a stimulation allowing torsion and detorsion, it would be unable to fulfill its extraordinary muscular power.
Having found an osseous structure in the bovid cardiac fulcrum and its relationship with the myxoidchondroid texture in human hearts, even in embryos, is consistent with the analysis of its interpretation. This disparity is associated with the different age evolution from chondroid to osseous material and with the greater power developed by bovid hearts, requiring a more rigid point of support.
Beyond its mere mention, until our investigations, no function or meaning of its presence had ever been assigned, as well as its lack of description in human beings.
The adjacency of the cardiac fulcrum to the AV node, surrounded and even invaded by a rich plexus of neurofilaments leads us to the anatomical consideration of an electromechanical unit in which stimulation energy and muscle mechanics participate. The effectiveness achieved with the placement of the pacing catheter in the vicinity of the right ventricular outflow tract confirms the findings of this investigation.
Fig. 4.Heart of a 27-week infant. Nerve trunk hypertrophy is seen in the cardiac fulcrum (black circles) adjacent to the AV node. HEx200. The inset shows a large-diameter nerve trunk in the cardiac fulcrum confirmed with immunohistochemistry for S-100.
Limitations
The most relevant limitation is the number of specimens studied, so this experience should be expanded. Future electrophysiological experiments and clinical investigations are necessary to explore this topic, since this research can be classified as initial.
Fig. 5.Comparison of pacemakers implanted in different points of the right ventricle (RV): tip, parahisian, right ventricular outflow tract (RVOT). p: patients.
CONCLUSIONS
The muscular segments that in continuity make up the ventricular chambers must carry out their movements on a point of support, which we have investigated and termed cardiac fulcrum, same as a skeletal muscle does in a firm insertion.
Its presence is constant in all the hearts studied, both bovid and human, but its structural characteristic is different. And this difference in the intimate analysis of the cardiac fulcrum is undoubtedly related to the resistance that it must oppose to the energetic action of the myocardium in hearts of different sizes.
The adjacency of the cardiac fulcrum to the AV node is important to explain the electromechanical unit of the heart.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
https://creativecommons.org/licenses/by-nc-sa/4.0/

©Revista Argentina de Cardiología
REFERENCES
- Trainini JC, Lowenstein J, Beraudo M, Mora Llabata V, CarrerasCosta F, Valle Cabezas J, et al. Fulcrum and Torsion of the Helical Myocardium. Ed Biblos, Buenos Aires, Argentina, 2022 pp. 27-105
- Trainini J, Lowenstein J, Beraudo M, Wernicke M, Trainini A, Llabata VM, et al. Myocardial torsion and cardiac fulcrum. Morphologie. 2021;105:15-23. https://doi.org/10.1016/j.morpho.2020.06.010
- Karamchandani JR, Nielsen TO, van de Rijn M, West RB. Sox10 and S100 in the diagnosis of soft-tissue neoplasms. Appl Immunohistochem Mol Morphol. 2012;20:445-50. https://doi.org/10.1097/PAI.0b013e318244ff4b
- Torrent-Guasp F. Estructura y función del corazón [Structure and function of the heart]. Rev Esp Cardiol. 1998;51:91-102. Spanish. https://doi.org/10.1016/s0300-8932(98)74718-9
- Rushmer RF. Structure and Function of the Cardiovascular System. Philadelphia, Saunders Company, 1972
- Best A, Egerbacher M, Swaine S, Pérez W, Alibhai A, Rutland P, et al. Anatomy, histology, development and functions of Ossa cordis: A review. Anat Histol Embryol. 2022;51:683-95. https://doi.org/10.1111/ahe.12861
- Cosín Aguilar JA, Hernándiz Martínez A, Tuzón Segarra MT, Agüero Ramón-Llin J, Torrent-Guasp F. Experimental study of the so called left ventricular isovolumic relaxation phase. Rev Esp Cardiol. 2009;62:392-9. English, Spanish. https://doi.org/10.1016/s1885-5857(09)71666-4
- Buckberg GD, Coghlan HC, Torrent-Guasp F. The structure and function of the helical heart and its buttress wrapping. V. Anatomic and physiologic considerations in the healthy and failing heart. Semin Thorac Cardiovasc Surg. 2001;13:358-85. https://doi.org/10.1053/stcs.2001.29957
- Henson RE, Song SK, Pastorek JS, Ackerman JJ, Lorenz CH. Left ventricular torsion is equal in mice and humans. Am J Physiol Heart Circ Physiol. 2000;278:H1117-23. https://doi.org/10.1152/ajpheart.2000.278.4.H1117
- Arvidsson PM, Töger J, Carlsson M, Steding-Ehrenborg K, Pedrizzetti G, Heiberg E, et al. Left and right ventricular hemodynamic forces in healthy volunteers and elite athletes assessed with 4D flow magnetic resonance imaging. Am J Physiol Heart Circ Physiol. 2017;312:314-28. https://doi.org/10.1152/ajpheart.00583.2016
- Pedrizzetti G, Arvidsson PM, Töger J, Borgquist R, Domenichini F, Arheden H, et al. On estimating intraventricular hemodynamic forces from endocardial dynamics: A comparative study with 4D flow MRI. J Biomech. 2017;60:203-10. https://doi.org/10.1016/j.jbiomech.2017.06.046
- Maksuti E, Carlsson M, Arheden H, Kovács SJ, Broomé M, Ugander M. Hydraulic forces contribute to left ventricular diastolic filling. Sci Rep. 2017;7:43505. https://doi.org/10.1038/srep43505
- Trainini JC, Trainini A, Valle Cabezas J, Cabo J. Left Ventricular Suction in Right Ventricular Dysfunction. EC Cardiology 2019;6:572- 57.
- Poveda F, Gil D, Martí E, Andaluz A, Ballester M, Carreras F. Helical structure of the cardiac ventricular anatomy assessed by diffusion tensor magnetic resonance imaging with multiresolution tractography. Rev Esp Cardiol (Engl Ed). 2013;66:782-90. https://doi.org/10.1016/j.rec.2013.04.021
- Carreras F, Ballester M, Pujadas S, Leta R, Pons-Llado G. Morphological and functional evidences of the helical heart from non-invasive cardiac imaging. Eur J Cardiothorac Surg. 2006;29:Suppl 1:S50-5. https://doi.org/10.1016/j.ejcts.2006.02.061
- Ballester M, Ferreira A, Carreras F. The myocardial band. Heart Fail Clin. 2008;4:261-72. https://doi.org/10.1016/j.hfc.2008.02.011
- Torrent-Guasp F, Buckberg GD, Clemente C, Cox JL, Coghlan HC, Gharib M. The structure and function of the helical heart and its buttress wrapping. I. The normal macroscopic structure of the heart. Semin Thorac Cardiovasc Surg. 2001;13:301-19. https://doi.org/10.1053/stcs.2001.29953
- Trainini JC, Beraudo M, Wernicke M, Carreras-Costa F, Trainini A, Mora Llabata V, et al. “Evidence that the myocardium is a continuous helical muscle with one insertion”. REC: CardioClinics 2022;57:194- 202. https://doi.org/10.1016/j.rccl.2022.01.006
- Mora V, Roldán I, Romero E, Saurí A, Romero D, Pérez-Gozalbo J, et al. Myocardial Contraction during the Diastolic Isovolumetric Period: Analysis of Longitudinal Strain by Means of Speckle Tracking Echocardiography. J Cardiovasc Dev Dis. 2018;5:41. https://doi.org/10.3390/jcdd5030041
- Mora V, Roldán I, Bertolín J, Faga V, Pérez-Gil MDM, Saad A, et al. Influence of Ventricular Wringing on the Preservation of Left Ventricular Ejection Fraction in Cardiac Amyloidosis. J Am Soc Echocardiogr. 2021;34:767-74. https://doi.org/10.1016/j.echo.2021.02.016
- Trainini JC, Elencwajg B, López-Cabanillas N, Herreros J, Lago N. Electrophysiological Bases of Torsión and Suction in the Continuous Cardiac Band Model. Anat Physiol 2015;5:S4-001. https://doi.org/10.13140/RG.2.1.4952.5200
- Trainini JC, Elencwajg B, López-Cabanillas N, Herreros J, Lowenstein J, Bustamante-Munguira J, et al. Ventricular torsion and cardiac suction effect: The electrophysiological analysis of the cardiac band muscle. Interventional Cardiol 2017;9,45-51.
- Elencwajg B, López Cabanillas N, Cardinali EL, Barisani JL, Trainini J, Fischer A, et al. The Jurdham procedure: endocardial left ventricular lead insertion via a femoral transseptal sheath for cardiac resynchronization therapy pectoral device implantation. Heart Rhythm. 2012;9:1798-804. https://doi.org/10.1016/j.hrthm.2012.07.010
- Ortega D, Logarzo E, Barja L, Paolucci A, Mangani N, Mazzetti E, Bonomini MP. Novel implant technique for septal pacing. A noninvasive approach to nonselective his bundle pacing. Journal of Electrocardiology 2020;63:35-40. https://doi.org/10.1016/j.jelectrocard.2020.09.00