
INTRODUCTION
Right ventricular outflow tract (RVOT) disorders are highly prevalent in children and adults with congenital heart disease. These disorders are often residual lesions that remain after previous surgery. (1) Improved survival in these patients has led to the identification of sequelae as arrhythmias and right heart failure resulting from right ventricular volume overload or pressure overload due to pulmonary valve dysfunction. (2) Historically, surgical pulmonary valve replacement has been the strategy of choice and is still performed nowadays with high levels of effectiveness. (3) In recent decades, the utilization of percutaneous pulmonary valve replacement (PPVR) has experienced exponential growth, to the point that treatment algorithms for RVOT dysfunction recommend it as the preferred strategy in patients with previous conduits, homografts, or bioprosthetic valves. (4,5) However, many patients have native or patched tracts (hereafter referred to as native RVOTs), in which the predominant lesion is pulmonary valve regurgitation (PVR). In such cases, percutaneous implantation is more complex due to the anatomy of the RVOT, its dynamic behavior, larger pulmonary valve annulus diameter, and the lack of an adequate landing zone for the valve. The differences in underlying congenital heart diseases, the type of previous surgical repair, and the anatomy of the pulmonary arteries result in RVOTs with variable morphology, posing significant challenges in planning and selecting patients. Recently, small studies have been published about the use of PPVR in native RVOTs, adapting heart valve prostheses to larger and more complex dimensions and anatomies. (6) In Argentina, most patients with tetralogy of Fallot (TOF) and its variants have undergone transannular patch repair, resulting in large RVOTs. This anatomy is challenging for the placement of balloon-expandable valves using a one-step technique (without previously preparing the landing zone for valve insertion).
We present the initial experience in our country with the balloon-expandable MyVal® (Meril Life Sciences, India) transcatheter heart valve (THV) for PPVR in native RVOTs using a one-step technique, along with a report on the immediate and mid-term results.
OBJECTIVE
The aim of this study is to report on the initial experience of PPVR using a one-step implantation technique with a balloon-expandable heart valve in Argentina.
METHODS
We conducted an observational and descriptive study of all consecutive patients treated with PPVR due to severe and/or free PVR with signs of right ventricular dilation/dysfunction who underwent transannular patch repair as part of the initial correction of their congenital heart disease. Cases were selected on an individual basis according to a pre-established study protocol. The one-step technique was defined as valve implantation in the native RVOT without previous dilation or stent placement for preparing the landing zone.
A balloon-expandable Myval® valve (Meril LifeScience, India) was implanted in all cases. This valve features a hybrid frame design, with a distal part consisting of hexagonal open cells and a proximal part featuring tightly packed hexagonal closed cells made of a nickel-cobalt alloy. The valve is made of bovine pericardium that has undergone anti-calcium treatment. It also has a proximal polyester polymer skirt to minimize the possibility of perivalvular leaks. A 14-Fr expandable sheath is used for implantation, and its maximal diameter reaches 34 mm. The valve is available in conventional (diameter 20, 23, 26, and 29 mm) and intermediate (diameter 21.5, 24.5, 27.5, 30.5 mm) sizes.
The variables analyzed included demographics and all data available before the procedure, during the procedure and at short and mid-term follow-up. After the procedure, all patients received aspirin 100 mg/day indefinitely.
Statistical analysis
Data collection and statistical analysis were performed in accordance with the guidelines for reporting mortality and morbidity after cardiac valve interventions. (7) Categorical variables are expressed as percentages. Continuous variables are expressed as median and interquartile range 25-75.
Ethical considerations
Percutaneous pulmonary valve replacement in native RVOT using a one-step technique with a balloon-expandable valve as an alternative to a new corrective surgery was approved by the institutional review board. Prior to undergoing the procedure, all adult patients or their parents or guardians (in the case of minors), were required to sign a health information form. The study was conducted following the recommendations of the Declaration of Helsinki. (8).
RESULTS
From July 2023 to April 2025, 10 patients (8 males) underwent PPVR using the Myval® valve (Meril LifeScience, India) in native RVOTs with a one-step technique (Table 1). The primary diagnosis for the entire cohort was TOF; one patient had absent pulmonary valve variant, and another had acquired absence of the left pulmonary artery branch. Three patients had previously required stenting of the left pulmonary artery branch. All patients were in NYHA functional class II and had PVR after the initial transannular patch repair of their RVOTs. Median age was 20.2 years (IQR, 12.5-34.3) and median weight was 61.3 kg (IQR, 33.7-77.2). All patients were in NYHA functional class II and had PVR after the initial transannular patch repair of their RVOTs.
Table 1
Demographic data, anatomical diagnosis, types of surgery, valves used, and complications
| Patient | Sex | Age (years) | Weight (kg) | Congenital heart defect | Type of repair | Valve and size (mm) | Final valve size implanted (mm) | Complications |
|---|---|---|---|---|---|---|---|---|
| #1 | M | 15 | 103 | TOF | Transannular patch + LPAB stenting | Myval 24.5 | 25.4 | Redilation 7 months after implantation |
| #2 | M | 15 | 51 | TOF | Transannular patch | Myval 32 | 30.5 | No |
| #3 | F | 29 | 85 | TOF | PV-sparing | Myval 30.5 | 31 | No |
| #4 | F | 28 | 59 | TOF | Transannular patch + LPAB stenting | Myval 26 | 24.5 | No |
| #5 | M | 13 | 69 | TOF | Transannular patch + LPAB stenting | Myval 27.5 | 26.8 | No |
| #6 | M | 46 | 77 | TOF | Transannular patch | Myval 30.5 | 28.4 | No |
| #7 | M | 10 | 27 | TOF Absent PV | Transannular patch | Myval 27.5 | 26.8 | No |
| #8 | M | 13 | 27 | TOF with absent LPAB | Transannular patch | Myval 32 | 29.7 | No |
| #9 | M | 17 | 70 | TOF | Transannular patch | Myval 32 | 30.4 | Mild perivalvular leak |
| #10 | M | 16 | 45 | TOF - Coronary artery anomaly | Transannular patch | Myval 30.5 | 28.7 | No |
LPAB: left pulmonary artery branch; M: male; PV: pulmonary valve; TOF: Tetralogy of Fallot.
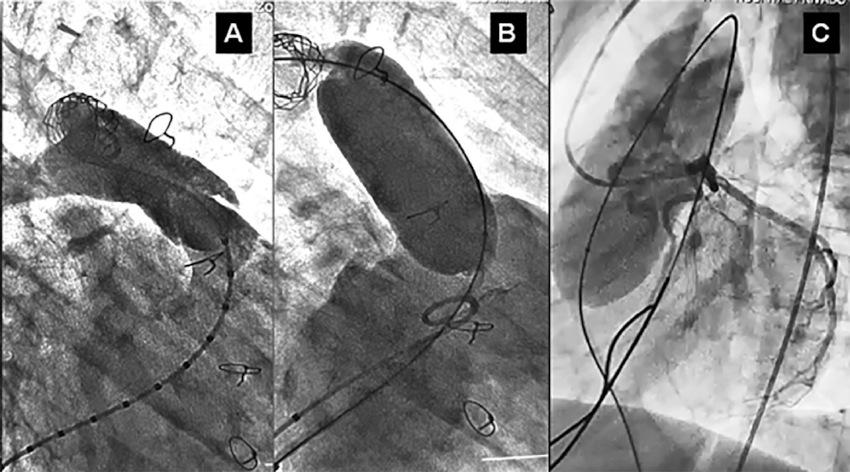
The median time since the last surgical repair was 13 years (8.7-19.5). Mean QRS duration was 143.4 ms (97.5-137.2). Pulmonary valve regurgitation, assessed by transthoracic color Doppler echocardiography, was grade 4 in all cases, with a median pulmonary annulus diameter of 24.5 mm (22.4-31). On cardiac magnetic resonance imaging, mean RV end-diastolic volume index was 151.4 mL/m2 (137.7-189.7), RV end-systolic volume index was 81.6 mL/m2 (73-90.2), regurgitation fraction was 52.4% (41-63.4), and RV ejection fraction was 47% (40.3-54.6). In all cases, the RVOT was measured beforehand with a non-compliant balloon during cardiac catheterization to select the diameter of the pulmonary valve to be implanted. The potential for distortion and/or compression of the coronary arteries post-implantation was ruled out by performing a selective coronary angiography concomitant with inflation of the non-compliant balloon in the RVOT (Figure 1). All patients underwent temporary RV apical pacing during balloon inflation and valve implantation at heart rates between 180 and 200 beats per minute to prevent device migration and/or malposition.
Figure 1
(A) Angiography in right anterior oblique projection (45) of the right ventricular outflow tract (RVOT). (B) Measurement of the RVOT with non-compliant balloon concomitant with right ventriculography to rule out peri-balloon leaks and estimate the correct diameter of the valve to be implanted. (C) Selective angiogram of the left coronary artery simultaneously with RVOT measurement with non-compliant balloon to rule out distortion and/or compression of the valve
Valve implantation was successful in all cases, with a mean fluoroscopy time of 26.5 min (23.7-39.4) (Figure 2). The diameters of the implanted valves were 24.5 mm (n = 1), 26 mm (n = 1), 27.5 mm (n = 2), 30.5 mm (n = 3), and 32 mm (n = 3). Mean pulmonary artery diastolic pressure increased from 11 mm Hg to 21.2 mm Hg. None of the patients exhibited significant RVOT gradient or PVR immediately after valve implantation, although one patient presented mild paravalvular leak immediately after valve implantation. The mean length of hospital stay was 36 hours (24-72). After a median follow-up of 6.7 months (1.2-15.7), PVR remained grade 0 in all patients, mean peak systolic gradient across the valve, estimated by color Doppler, was 21.8 mm Hg (15-30.1), and functional class improved to NYHA I in 9 patients. Only one patient increased the gradient 7 months after implantation and required high-pressure balloon dilation which reduced the gradient to 21 mm Hg. There were no cases of valve displacements and/or fractures, episodes of arrhythmias, infective endocarditis (IE), need for valve explantation, or deaths during short- and mid-term follow-up.
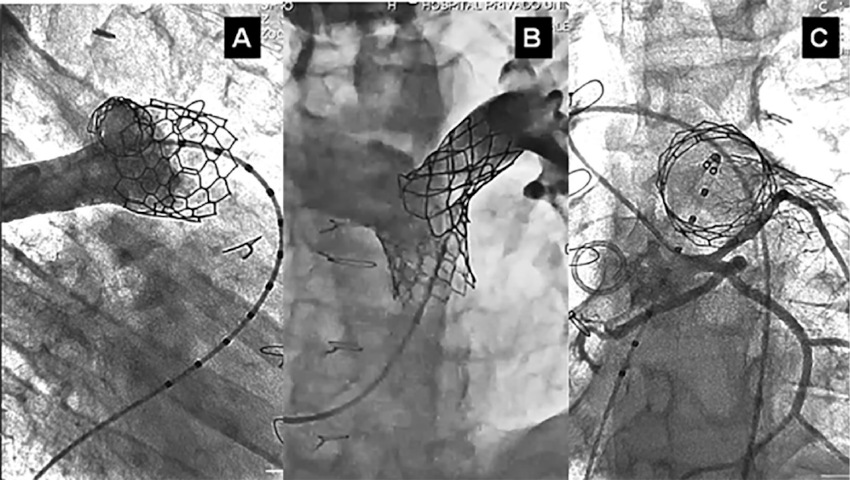
Figure 2
(A) Right ventricular outflow tract (RVOT) in right anterior oblique projection (45°) and (B) in left anterior oblique projection (30°) - cranial angulation (30°), with the valve in situ demonstrating the absence of residual valve regurgitation and perivalvular leaks. Its relationship to the stent previously placed in the left pulmonary artery branch is also observed. (C) Selective coronary angiography with valve in situ in the left anterior oblique projection (20°) - caudal angulation (30°), showing the integrity of the coronary arteries after valve implantation and the optimal circular expansion of the prosthetic valve, ruling out its underexpansion.
DISCUSSION
The adverse impact of PVR has been extensively studied in patients with TOF after surgical repair. (4) Percutaneous pulmonary valve repair using balloon-expandable valves is an established alternative to surgical reintervention and its use is limited to patients with dysfunctional conduits between the RV and pulmonary artery as well as on bioprosthetic valves. (4,5) Most TOF patients have undergone transannular patch repair, resulting in large RVOTs. (9) This anatomy is a challenge for the placement of balloon-expandable valves using a one-step technique.
Currently, two models of balloon-expandable valves are commercially available and approved for the treatment of dysfunctional bioprosthetic valves and conduits/homografts: the Melody® (Medtronic, United States) and Sapien® (model S3, Edwards Lifesciences, United States) bioprosthetic valves. Although they have not yet been authorized for implantation in native RVOTs, both have been used off-label in this setting. (10) The Melody heart valve prosthesis has a maximum diameter of 24 mm, while the Sapien S3 has a maximum diameter of 29 mm. To address the specific characteristics of native RVOTs, several models of self-expanding valves have been developed, such as the Venus-P® (Venus MedTech, China), PULSTA® (TaeWoong Medical, South Korea), and Harmony valves (Medtronic, United States) which have a maximum diameter of 34 mm according to the different models. The Alterra® device (Edwards Lifesciences, United States) has also been used. This valve serves as a self-expanding present onto which a SAPIEN S3 valve is later implanted.
In recent years, there has been a significant increase in the availability of data regarding the efficacy, safety, and durability of percutaneous valves implanted in the pulmonary position. The study with the largest number of cases is the IMPACT registry, conducted by the American College of Cardiology, which included 4513 patients who were treated with PPVR (57% with Melody valves and 43% with Sapien valves). Thirty-three percent of valve implants were into homograft conduits, another 33% into bioprosthetic valves, 25% were in native RVOTs, and 6% were into Contegra® conduits (Medtronic, United States). Success was achieved in 95% of patients (95.7% in homografts, 96.2% in bioprosthetic valves, 94.2% in native RVOTs, and 95.4% in Contegra conduits). Adverse events occurred in 2.4% of patients, most commonly in homografts (2.9%) or native RVOTs (3.4%). (11)
Another multicenter registry, which included a significant number of patients, reported 2476 cases. The data indicate that 82% of the cases involved Melody valves, while 18% utilized SAPIEN valves, with 16% of these cases involving implants in native RVOTs. The 8-year survival rate following implantation was 91.1%, with a reintervention rate of 25.1%, which is consistent with the rates reported in other surgical series. (12,13)
Self-expanding valves were designed for large diameter RVOTs, adapting to the different and challenging anatomies of the outflow tracts with more stable fixation. The published data suggest a very high implant success rate with encouraging results during short- and mid-term follow-up, including a low complication rate. (14,15) Although the initial results of implanting these self-expanding valves were favorable, warnings have recently been published regarding their complications, including perforations of the main pulmonary artery and complex ventricular arrhythmias. (16-18) Regarding the latter, future access to the RVOT for an electrophysiology study with potential ablation of an arrhythmic substrate may be limited by the presence of the valve metal mesh in the anatomical site. (19)
The higher incidence of IE has been widely reported and associated with patient-related risk factors, as adult age, male sex, history of IE, discontinuation of aspirin, unprotected exposure to high-risk medical procedures. Procedure-related factors that increase the risk of IE include longer procedures, a higher number of stents placed as landing zones, higher residual gradients, the presence of homografts or bioprosthetic valves, and valves composed of bovine jugular tissue compared to those made from bovine pericardium. (20)
Considering the most common anatomical characteristics of dilated native RVOTs in our setting, the reported effectiveness and safety of balloon-expandable valve placement, the cost-benefit ratio of the intervention, the complications described in self-expanding valves and devices, the higher incidence of IE in cases where a safe landing zone is created with stents, and, in addition, the availability of a user-friendly, balloon-expandable valve requiring a small-diameter sheath (14F) that expand to a maximum diameter of 34 mm such as Myval® Meril LifeScience, India), we decided to begin implanting these valves in native RVOTs using a one-step technique.
Our initial data show that the implant has a high success rate and that the procedure is safe and effective. It should be noted that patient selection is crucial and must include an evaluation using advanced imaging methods and prior cardiac catheterization with accurate measurements of the native RVOT using non-compliant balloons. Concomitant compression and/or coronary distortion must also be ruled out. This strategy can reduce the incidence of the most common complications of this procedure, as valve migration/ embolization (0-4.5%) in large native RVOTs without a prior landing zone, paravalvular leaks, and coronary compression/distortion (3%). Additionally, the utilization of long (65 cm) sheaths (WL. Gore, United States) has been shown to prevent another less frequently described complication, such as tricuspid valve injury (3-6%). (18) In patients with anatomies that present more challenges, such as those with stents in the pulmonary artery branches, we demonstrated favorable outcomes in three cases in the present series, thereby indicating that this is not a relative contraindication for this strategy. Transient RV apical pacing during valve inflation is strongly recommended in order to avoid malposition or migration of the bioprosthetic valve, particularly in dynamic RVOTs with large diameter variability at different times of the cardiac cycle. The occurrence of mild paravalvular leak in one case and the need for early valve redilation in another case in our series suggest that it will be necessary to include a larger number of patients with a longer follow-up period to confirm the initial results of our experience. Regarding valve durability, one year of follow-up data is currently available, confirming acceptable results. (21,22)
Finally, we believe that PPVR in native RVOTs using a single-step strategy, as presented in this experience, offers clear and significant advantages. These include simplifying the procedure, making it less invasive and less risky by avoiding the placement of stents as a landing zone and therefore potentially reducing the incidence of IE and complex ventricular arrhythmias. Additionally, and a key advantage in our context, it is highly cost-effective.
There are limitations to this study. The data were collected retrospectively and from a single center with expertise in percutaneous valve implants; therefore, the results presented may not be generally applicable. There may also be selection bias due to the inclusion of high-risk patients with RVOT with severe or free PVR. Finally, this is an initial and preliminary report of a novel procedure involving the use of valves approved for off-label use in RVOT, with a clear need for longer-term follow-up.
CONCLUSIONS
Percutaneous pulmonary valve replacement in native RVOT using a one-step technique with balloon-expandable Myval valves Meril LifeScience, India) is feasible, safe and efficient in this preliminary experience in Argentina. Immediate restoration of pulmonary valve competence was observed after implantation. The appropriate selection of patients and the size of the valve to be implanted are crucial variables for the success of the procedure.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
Funding
None declared.
REFERENCES