
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is increasingly recognized as a cause of acute coronary syndromes (ACS) not due to plaque rupture or erosion or coronary embolization, especially in young women. It represents between one-third and one-quarter of acute myocardial infarctions in women under 50 years of age in various international cohorts, and between 15% and 20% of infarctions in pregnant women and during the postpartum period. (1-5)
Spontaneous coronary artery dissection is a condition not fully understood, although the formation in the arterial wall of an intramural hematoma caused by a tear in the intima or spontaneous hemorrhage of the vasa vasorum, not related to atherosclerosis, iatrogenesis, or trauma, is the most widely accepted pathophysiology. (1-4) Timely diagnosis is a predictor of outcome and guides definitive treatment according to the type of dissection, and unlike atherosclerotic infarction, a conservative management takes precedence over interventional treatment in most cases, the latter being reserved only for cases of acute artery occlusion, or those in which there is hemodynamic instability. (5-8)
There are several registries from developed countries that reflect specific aspects of the development, approach, mortality, and SCAD recurrence. However, this is not the case in the Latin American population, especially in Argentina. (5-7)
This article presents the first multicenter SCAD experience in Argentina, including patients from both public and private healthcare systems from 2023 to 2025. The purpose of this first stage was to describe demographic data, clinical presentation, hospital outcomes, established treatment, and one-year clinical follow-up in order to understand the approaches to this pathology in our country and thus standardize diagnostic and therapeutic criteria.
METHODS
This was an observational, descriptive, retrospective, multicenter study conducted in two public hospitals and four private medical centers in the Autonomous City of Buenos Aires from January 2023 to January 2025, with the aim of obtaining local data on an underdiagnosed and increasingly prevalent disease. Participating centers had to meet physical and human standards to ensure definitive diagnosis of the disease. All patients were prospectively included since 2023 in two centers and retrospectively in the rest of the participating centers. The diagnosis and classification of SCAD was according to the Yip-Saw et al. classification and the modification proposed by a group of national researchers. (7,8) The definitive diagnosis was agreed upon by the heads of the interventional cardiology and coronary care units at each participating center. Patients with iatrogenic dissection or diagnostic doubts were excluded. Following es- tablished evidence, intravascular imaging was not used as a diagnostic method. (1-4) Due to the expected small sample size, a descriptive analysis was performed of the baseline demographic, clinical, and angiographic characteristics, as well as the therapy used during hospitalization and followup treatment. The presence of precipitating and predisposing factors was also analyzed. In addition, unexpected events such as death, reinfarction, unexpected revascularization, coronary dissection recurrence, chest pain during follow-up, and follow-up with noninvasive imaging (coronary computed tomography) were evaluated.
All patients included in the registry signed an informed consent form and agreed to participate in the analysis. Identifying data were anonymized at each center and were known only by the local investigators, responsible for telephone or in person follow-up of each patient. The analysis was conducted in accordance with the Declaration of Helsinki and its amendments, (9) the guidelines for good clinical research practices, and the Personal Data Protection Act No. 25236. (10)
Excel software (Microsoft Windows, USA) was used to transfer the study variables and perform the descriptive analysis.
RESULTS
Twenty-six patients diagnosed with SCAD at two public hospitals and four private medical centers in the Autonomous City of Buenos Aires were included over a two-year period (Figure 1). Most patients were women (84.6%). Median age was 47 years (interquartile range, IQR, 42-56.5), and hypertension was the most common cardiovascular risk factor, present in nine patients (34.6%), followed by dyslipidemia in six (23.1%) and type 2 diabetes mellitus in three (11.5%). The rest of the clinical characteristics, in addition to the predisposing and precipitating factors identified, are described in Table 1, which shows emotional stress as the main precipitating factor present in eleven patients (42.3%).
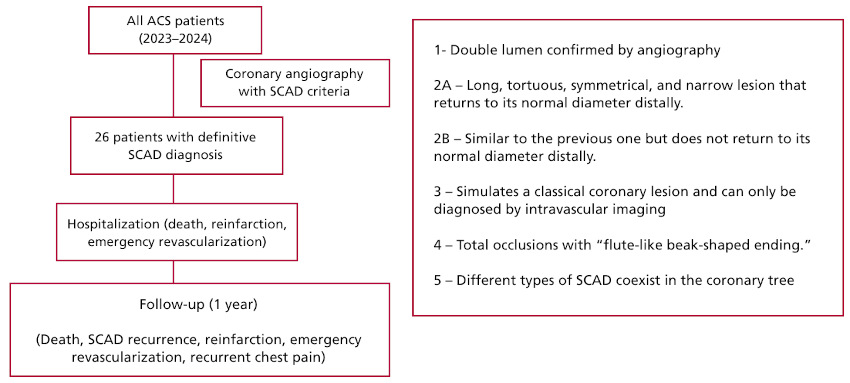
Table 1
Demographic, clinical, and angiographic characteristics.
| Variable | |
| Female gender (%) | 84.6 |
| Age, years, mean (SD) | 48.4 (10.3) |
| Cardiovascular risk factors (%) | |
| Smoking | 23.1 |
| Hypertension | 34.6 |
| Dyslipidemia | 23.1 |
| Diabetes | 11.5 |
| Family history of coronary heart disease, (%) | 3.8 |
| Weight, kg, mean (SD) | 74.5 (15.6) |
| Height, cm, mean (SD) | 155 (6.9) |
| Previous pregnancies, (%) | 30.7 |
| Predisposing factors (%) | |
| Current pregnancy | 0 |
| Postpartum period | 0 |
| Rheumatological diseases | 11.5 |
| Precipitating factors (%) | |
| Physical stress | 19.2 |
| Emotional stress | 42.3 |
| Toxic substances | 7.7 |
SD: standard deviation
The presence of muscular fibrodysplasia was explored in three patients using non-invasive imaging, with no pathological findings. None of the patients with a history of pregnancy reported complications during pregnancy.
The clinical presentation was with typical chest pain in 100% of patients, and in seven cases (26.9%) it was accompanied by dyspnea. Non-ST-segment elevation acute coronary syndromes (NSTEACS) were the most frequent electrocardiographic presentation, in 57.7% (n = 15) of cases. Table 2 shows the symptoms and baseline diagnosis on admission. The most commonly affected vessel was the left anterior descending artery (n = 16, 61.5%), and the most frequent type of dissection was type 2A in fourteen patients (53.8%) with multiple dissections identified in two cases. The rest of the angiographic characteristics are presented in Table 3, together with the motility and function characteristics of the baseline echocardiogram. Concentric, septal, and apical ventricular hypertrophy was detected in four patients (15.3%).
Table 2
Admission symptoms and electrocardiographic findings
| Symptoms (%) | |
| Typical chest pain | 100 |
| Nausea/vomiting | 15.4 |
| Dyspnea | 26.9 |
| Sudden death | 3.8 |
| Admission diagnosis (%) | |
| STEACS | 42.3 |
| NSTEACS | 57.7 |
STEACS: ST-segment elevation acute coronary syndrome; NSTEACS: Non-ST-segment elevation acute coronary syndrome
Table 3
Angiographic characteristics and modified Yip-Saw classification.
| Affected artery (%) | |
| Right coronary artery | 7.7 |
| Left coronary trunk | 0 |
| Left anterior descending artery | 61.5 |
| Circumflex artery | 38.4 |
| Intravascular imaging (%) | 7.7 |
| Classification (%) | |
| Type I | 11.5 |
| Type 2 | 73.1 |
| Type 2A | 53.8 |
| Type 2B | 19.2 |
| Type 3 | 11.5 |
| Type 4 | 7.7 |
| Type 5 | 7.7 |
| Baseline echocardiogram (%) | |
| No wall motility disorders | 19 |
| Segmental hypokinesia | 47.6 |
| Akinesia | 28.6 |
| Ventricular hypertrophy | 14.3 |
| Preserved LVEF | 76.2 |
LVEF: left ventricular ejection fraction.
Fifteen patients (57.7%) were initially treated conservatively. Beta-blockers were used in 100% of cases, and aspirin in 92%. Among this group, one patient underwent revascularization during hospitalization due to hemodynamic instability. A total of twelve patients (46.1%), underwent revascularization, eleven at baseline and one during hospitalization, all by angioplasty, with 1.9 stents per patient.
Twenty-three patients (88.4%) received statins at discharge. Among patients who received conservative treatment without stent implantation, 35.7% were discharged with dual antiplatelet therapy, 92.8% with at least one antiplatelet agent, and one patient was anticoagulated.
Regarding events, there were no deaths and one emergency revascularizations during hospitalization.
During follow-up, four patients (15.4%) reported recurrent chest pain, and in three cases, anatomical evaluation was again performed, in two by coronary angiography and in one by computed tomography, without evidence of new dissections.
DISCUSSION
We present the first Argentine SCAD registry. Of note, a significant effort was made to recruit as many centers as possible and, hence patients with this rare disease.
Similarly, as in large global series, most cases were perimenopausal women with high emotional stress. This could be explained by some genetic and conformational differences in the arterial walls of men and women, in addition to apparent hormonal modifications in coronary estrogen and progestogen receptors which trigger mechanisms that alter vascular architecture both in pregnancy and perimenopause and produce conformational changes predisposing to SCAD. (8,11,12)
This disease accounts for 1 to 40 out of 1000 angiographies performed per center, and in turn explains 2 to 4% of all SCADs and up to one-third of AMIs in the perimenopausal female population. (13-16)
There are different genetic variants in collagen fibers that are associated with higher risk of developing the disease. (15-20) Although fibromuscular dysplasia is the arteriopathy and genetic condition most closely associated with SCAD development, (2,9) the search for this disease was very poor in our series and it was possible to perform angiotomography of intra-abdominal and cervical vessels only in 3 patients, without any positive results. Although pregnancy (especially in the third trimester and in the immediate postpartum) is associated with SCAD, it did not manifest in our series. (19)
In all the series presented, including ours, SCAD develops in populations with few or no cardiovascular risk factors. In the group analyzed, the most relevant cardiovascular risk factor was hypertension, analogous to classic coronary artery disease, and in line with other published series. (18-20)
When analyzing the presentation on admission, and comparable to large international series, more than half of the cases evidenced NSTEACS (5,6,11,18-20).
Also, similar to global reports, the most commonly involved artery was the left anterior descending artery, and, importantly, two patients presented with multiple types of dissection in different vascular territories. Despite the incidence of intravascular imaging in these patients is low, both in this registry and worldwide, there are recommendations that encourage its use in cases where there are diagnostic doubts. (1-3,16)
There are some points worth highlighting in our registry. On the one hand, in our series, 1 in 5 patients continued to experience persistent pain after discharge, in line with other registries. (5,6,11,18-20) On the other hand, there was no evidence of consensus on antiplatelet therapy in patients treated conservatively, either in terms of selection (aspirin or clopidogrel), dosage (single or dual antiplatelet therapy), or duration.
Among the study limitations, the small sample size stands out. Nevertheless, different therapeutic approaches were evidenced, especially during follow-up, as well as the lack of screening for fibrodysplasia, which allows us to outline guidelines for possible position documents and recommendations from our Society.
CONCLUSION
Spontaneous coronary artery dissection occurs predominantly in women between the 4th and 5th decades of life without cardiovascular risk factors, generally as acute coronary syndrome and with emotional stress as the main triggering factor. Treatment was conservative except in cases of hemodynamic instability, and the results during hospitalization and at one year of follow-up were good. The lack of consensus on antithrombotic treatment in this group of patients should be noted.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web).