
INTRODUCTION
Heart failure (HF) is one of the leading causes of morbidity and mortality worldwide and represents a significant public health problem. This disease has a dynamic risk profile: risk is particularly high at the time of diagnosis, tends to decrease with the implementation of guidelinedirected medical therapy, and increases significantly again with each episode of decompensation. (1)
Approximately one out of six patients with HF with reduced ejection fraction (HFrEF) develops worsening HF within the first 18 months of followup, resulting in the need for hospitalization or treatment with intravenous diuretics. These patients also present high hospital readmission rate as early as the first month following the index event, reflecting the recurrent and complex nature of the disease. (2)
In recent decades, HF has evolved into a global epidemic, with a lifetime risk estimated at up to 25% (3,4) and a cumulative mortality rate reaching 30–50% at 3 years and up to 75% at 5 years. (5) This impact is magnified in Latin America, where the burden of disease and structural constraints underscore the need for structured care strategies tailored to the local context.
Acute HF remains one of the leading causes of hospitalization and mortality, particularly in subjects older than 65 years. Not only does it have a profound individual impact, but it also poses a significant burden on health care systems, given the vast resources required for its management. Despite the advances achieved in the armamentarium and prevention strategies, the rate of midterm adverse events remains alarmingly high in patients hospitalized for acute HF. The probability of hospital readmissions within six months reaches approximately 50%, with annual mortality ranging between 12% and 20% according to various international registries. (6-8) These figures, consistent across different regions and settings, demonstrate that hospitalization for HF remains an adverse risk marker.
Reducing readmissions for HF is a strategic goal, as it can simultaneously lower healthcare costs and improve the quality of care provided. However, achieving this goal poses a complex challenge for healthcare systems, particularly in countries with structural and budgetary constraints. In this context, the increasing complexity of HF and the expansion of therapeutic options have given rise to new care requirements, including specialized units, multidisciplinary teams, trained personnel, adequate infrastructure, and integrated care networks across different levels and centers. (9-11)
In this scenario, specialized heart failure units have emerged as an innovative organizational model of care, integrating trained multidisciplinary teams, standardized protocols, educational strategies, and structured monitoring. In developed countries, various programs of this type have been shown to reduce hospital readmissions, improve adherence to guidelinedirected medical therapy, and optimize the quality of healthcare quality measures, with a favorable impact on mortality and longterm costs. (12-16)
However, there is still limited and fragmented evidence regarding the implementation, sustainability, and adaptation of these models in the Latin American context, particularly in Argentina. In low- and middleincome countries, the limitations in access to timely diagnosis, prognosismodifying therapies, and organized models of care create a significant gap between guideline recommendations and realworld practice, resulting in high rates of rehospitalization and mortality. (17-20)
OBJECTIVE
Within this framework, the primary objective of this study is to evaluate the impact of a specialized heart failure unit on qualityofcare measures in patients hospitalized for acute heart failure at a highcomplexity center in Latin America. To this end, the program’s development was examined in two stages: the initial phase (2014–2019) and the consolidation phase (2020–2024). The indicators analyzed included inhospital mortality, 30-day hospital readmission, and length of hospital stay, with the aim of assessing the program’s development over a 10-year period.
METHODS
Study design
We conducted a retrospective observational cohort study that included consecutive patients admitted with a primary diagnosis of acute HF between January 2014 and December 2024. The study was conducted at a leading cardiology center in Argentina, which implemented a structured program for the management of HF.
Inclusion and exclusion criteria
Patients diagnosed with primary acute HF were included in the study.
Those patients with HF secondary to infective endocarditis, severe organic valvular heart disease requiring intervention, myocarditis, acute myocardial infarction, or pulmonary thromboembolism were excluded, as well as those undergoing invasive procedures during hospitalization, such as cardiovascular surgery, percutaneous coronary intervention, pacemaker implantation, or heart transplantation.
Patient identification and data collection
Heart failure patients were identified based on the diagnoses recorded using the International Classification of Diseases (ICD) coding system. The discharge diagnosis was recoded and verified by a trained nurse. In cases of inconsistencies, the final decision was made by consensus between two heart failure specialists.
The variables analyzed included inhospital mortality, length of hospital stay, 30-day hospital readmission for HF, documented education at discharge, prescription of betablockers and reninangiotensin system inhibitors or angiotensin receptorneprilysin inhibitors (ARNIs) in recent years, and assignment of a followup appointment at discharge.
In 2023, the Institute for Clinical Effectiveness and Health Policy (IECS) conducted an external audit to assess the methods used for analyzing the indicators.
The collected data was updated monthly, with the cutoff date set at the end of each month. Based on this data, graphs and reports were prepared and presented at the institutional regular review meetings. The Annual Indicators Report served as the systematic synthesis of all the information.
Specialized HF management program
The specialized HF management program implemented in the unit consisted of a multidisciplinary and comprehensive approach, with the following key characteristics (1):
Critical path method: Standardized protocols for the management of acute HF, including decongestion strategies, titration of prognosticmodifying medication, early mobilization, identification of barriers to discharge, and structured discharge planning.

Structured hospital discharge checklist: Assessment of the implementation of pharmacological treatment, scheduled postdischarge followup appointment, need for devices, patient education, and prognosismodifying strategies (vaccination, smoking cessation counseling).
Dedicated heart failure physicians: A dedicated team of HF-specialist cardiologists leading patient care with fulltime commitment and involvement in the training of future HF specialists.
Specialized HF nurses: Advanced practice nurses specialized in HF management who performed periodic clinical assessments, followup, and continuous monitoring of treatment response.
Dedicated administrative staff: Efficient coordination of hospital discharges, outpatient followup tracking, and postdischarge clinic scheduling.
Discharge education with written instructions: Provision of comprehensive patient education materials detailing HF management, medication adherence strategies, and warning signs via educational booklets, a dedicated website, and predischarge nurse counseling.
Written patient instructions: Grid with drug names, specific dosages, and timing/administration schedules.
Structured postdischarge followup: Active followup through inperson and virtual consultations, with an initial postdischarge followup scheduled within 14 days of discharge. Highrisk patients were scheduled for appointments at the day hospital.
Priority consultations: Provision of urgent, rapidaccess consultations at the day hospital for complex and highrisk patients.
Grand rounds for advanced management: Periodic multidisciplinary case discussions for complex clinical decisionmaking, including advanced HF, cardiogenic shock, pulmonary hypertension, cardiomyopathies, and cardiac transplantation.
Ultrasoundguided lung decongestion: Use of ultrasound to assess response to diuretics and optimize congestion management.
Urinary sodium measurement: to systematically adjust the diuretic algorithm in the day hospital and in selected cases during hospitalization.
Telemonitoring: Progressive implementation over the past three years of technology for remote monitoring of vital signs and clinical parameters following hospital discharge.
Day hospital: Outpatient management of selected patients with lowrisk acute heart failure and intensive followup of higherrisk patients, thereby avoiding unnecessary hospitalizations.
Regular presentation of quality indicators: Analysis and regular presentation of care measures as part of an institutional program for continuous quality improvement.
Invasive testing: In patients with heart failure, pulmonary hypertension, and postheart transplantation
Definition of variables
The following endpoints were defined:
Inhospital mortality: Percentage of patients who died during the index hospitalization.
30-day hospital readmission: Percentage of patients who were readmitted within 30 days following discharge due to acute heart failure.
Length of hospital stay: Total number of days of hospitalization per patient.
Statistical analysis
Descriptive statistics were used to characterize the study population and the results of the quality measures. Qualitative variables are presented as frequency and percentage, and quantitative variables are expressed as mean and standard deviation (SD) or median and interquartile range (IQR) according to their distribution. Linear regression analysis was performed to evaluate temporal trends in mortality, hospital readmission, and length of hospital stay. Results were compared between the two periods using the Student’s ttest for continuous variables and the chisquare test for categorical variables. Additionally, the coefficient of variation (CV) was calculated for inhospital mortality and 30-day hospital readmission in each period, as a measure of the stability and consistency of care performance over time. A pvalue < 0.05 was considered statistically significant.
Ethical considerations
The study was approved by the institutional review board and registered on the PRIISA.BA platform of the Ministry of Health of the City of Buenos Aires. All the patients signed an informed consent form authorizing the transfer of their personal data for scientific purposes. The study was conducted following national and international ethical standards for research on human subjects, as the Declaration of Helsinki, (21) National Ministry of Health resolution 1480/20011, Act 3301 of the city of Buenos Aires, and ANMAT regulation 6677/10 with amendments 4008 and 4009.
RESULTS
Demographic and clinical characteristics
A total of 3368 hospitalizations for acute HF between 2014 and 2024 were analyzed. Mean age was 72±10
years and 60% were men.
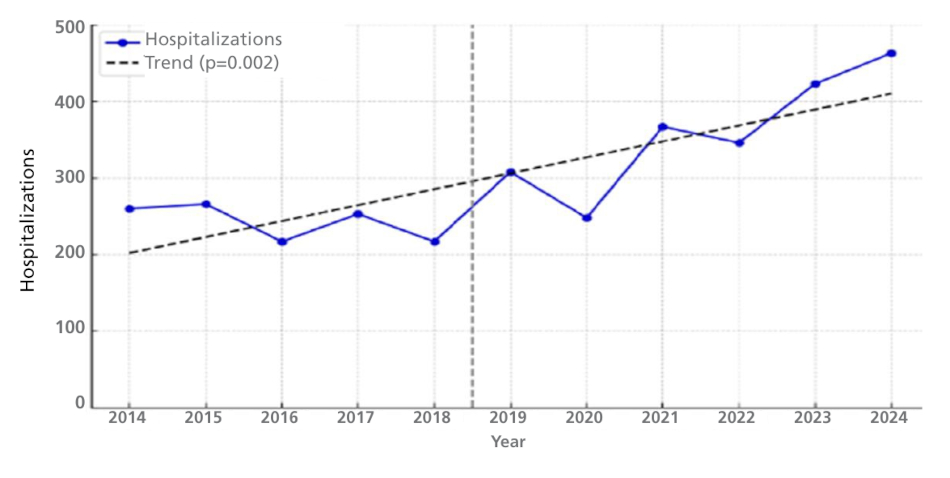
Hospitalization volume and trends The annual volume of hospitalizations for acute HF increased significantly over the years, rising from 260 in 2014 to 463 in 2024 (p = 0.002) (2).
In-hospital mortality
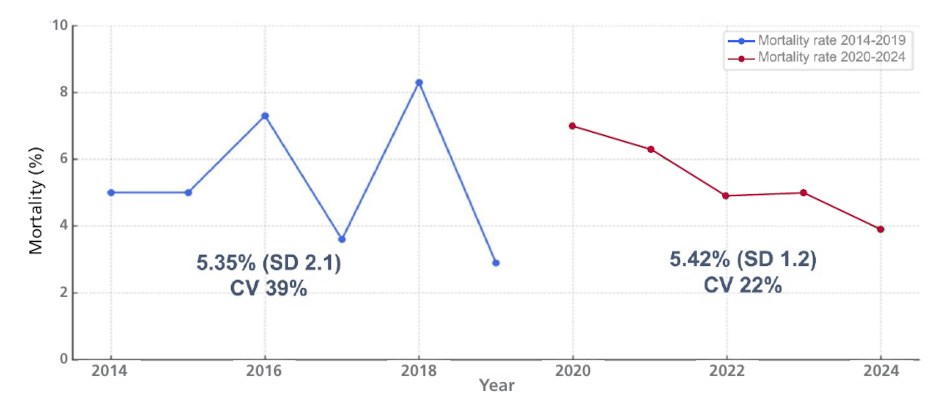
In-hospital mortality exhibited a slight decrease across the study period, falling from 5.0% in 2014 to 3.9% in 2024, although this reduction was not statistically significant (p = 0.648). However, there was a trend to-
ward lower in-hospital mortality and greater stability with a lower coefficient of variation (3).
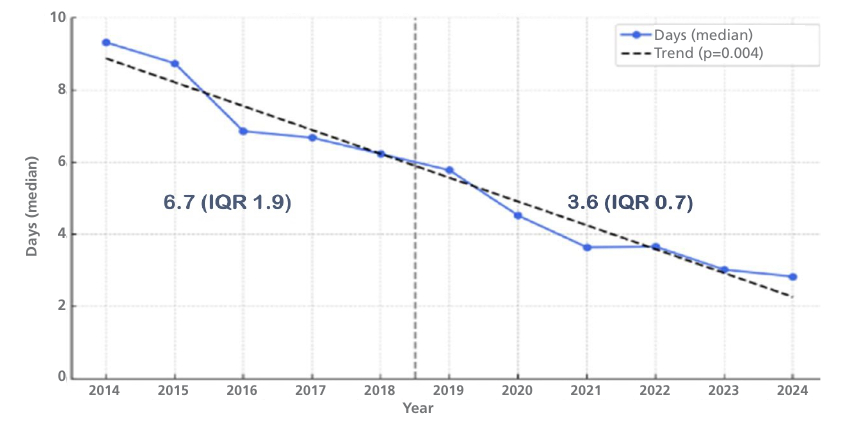
Length of hospital stay The length of hospital stay showed a progressive and sustained reduction over the analyzed period (2014–2024), with a significantly downward trend over time (p < 0.001).
Length of hospital stay
The length of hospital stay showed a progressive and sustained reduction over the analyzed period (2014–2024), with a significantly downward trend over time (p < 0.001).
Mean length of hospital stay decreased significantly from 9.3 days in 2014 to 2.8 days in 2024 (p < 0.001). Median length of stay was significantly shorter during the program consolidation phase compared to the initial period: 3.6 (IQR 0.7) vs. 6.7 (IQR 1.9); p = 0.004 (4).
30-day hospital readmission
30-day hospital readmission rate for HF did not show statistically significant differences between the program initial period (2014–2019) and the consolidation phase (2020–2024). However, there was a significant shift in the temporal pattern of the indicator. During the initial phase, annual hospital readmission rates showed marked interannual variability, with values ranging approximately from 6% to 21%. In contrast, during the consolidation phase, 30-day hospital readmission rate remained within a narrower range, with values consistently around 13–14%. This finding was reflected in a substantial reduction in the CV of this indicator during the consolidation phase compared to the initial period, suggesting more stable and consistent care performance over time (5).

CV: coefficient of variation; SD: standard deviation
DISCUSSION
The results suggest that the implementation of a specialized heart failure unit was associated with a positive impact on multiple healthcare quality measures, particularly in terms of hospital efficiency. The sustained reduction in length of hospital stay observed over the decade analyzed constitutes the most robust finding of the study and reflects more effective clinical management. This is likely related to optimized lung decongestion, earlier initiation of prognosismodifying therapies, and the structured organization of the discharge and postdischarge followup processes. These findings are consistent with international experiences that have demonstrated that specialized heart failure units improve efficiency and clinical outcomes, especially in middleincome health systems. (10)
Inhospital mortality presented an absolute reduction, from 5.0% in the initial phase to 3.9% in the consolidation phase; yet this difference was not statistically significant. International registries such as ADHERE (22) and ESC-HF Pilot (23) have reported similar rates, while national and regional studies have described higher inhospital mortality rates, ranging from 7% to 11%. (17,20,24) The lack of statistical significance in our analysis may be attributed to the clinical heterogeneity of the patients and the inherent complexity of acute HF, a condition that remains associated with high mortality, even under optimal management. However, the observed reduction in absolute terms, along with greater interannual stability of the indicator, suggests a possible beneficial effect of the implemented care model.
The 30-day hospital readmission rates for HF were not significantly different between the two periods. However, during the consolidation phase, there was a marked reduction in the interannual variability of the indicator, as reflected in a lower CV. This finding suggests more consistent and predictable care performance, which may be linked to the implementation of standardized processes, structured followup, discharge education, and the use of a day hospital for selected highrisk patients.
From the perspective of continuous quality improvement, stability of results constitutes a relevant indicator of care performance. (25) In this regard, even in the absence of significant reductions in hard events, the lower variability observed in mortality and hospital readmission during the consolidation phase can be interpreted as a sign of the program’s maturity and greater consistency in the care provided.
The literature has reported that a multidisciplinary approach in HF clinics reduces hospitalizations, improves adherence, and optimizes the use of guidelinedirected medical therapy, with an impact on clinical outcomes and costs, particularly in highincome countries. (10,17-20,26)
The prevalence of heart failure and its associated burden continue to rise, driven by population aging and increased survival among patients with cardiovascular disease. (27) In this context, there are still significant challenges related to structural limitations, heterogeneity in the quality of care, and restricted access to specialized care models, particularly in low- and middleincome countries, which is associated with worse clinical outcomes and inefficient use of health care resources. (18,28) Our results show that, even in this scenario, the implementation of a structured, specialized care program is feasible and can generate sustained improvements in key care quality measures.
It is important to note that, although the impact on inhospital mortality and 30-day hospital readmissions did not show statistically significant differences between the two periods analyzed, the progressive and sustained reduction in length of hospital stay constitutes a relevant indicator of improvement in the efficiency and quality of care. Length of hospital stay has been recognized as a measure sensitive to the organization of care and the coordination of care processes. Its reduction, when achieved without an increase in adverse events, reflects more efficient and patientcentered care. (29) In this regard, integrating strategies such as structured discharge education, telemonitoring, and day hospital for selected patients could have contributed to the observed results. (30) This study provides local evidence on the feasibility and impact of a specialized heart failure unit in a Latin American setting, facilitating comparison of these results with those from national multicenter registries. The ARGEN-IC registry, which included patients from 18 Argentine provinces, reported longer length of hospital stay, high inhospital mortality, and limited access to early outpatient followup. (20) In comparison, our experience shows shorter length of hospital stay rates and greater stability in clinical outcomes over time, suggesting the positive impact of a structured and sustained care model.
The study has several limitations that should be considered. First, it is a singlecenter, retrospective study, with the biases inherent in this type of design. No analysis was performed adjusted for clinical severity, comorbidities, or other relevant prognostic predictors, which limits the causal interpretation of the results. Furthermore, in recent years, the hospital has established itself as a highcomplexity referral center for advanced diseases and as a heart transplant center, which likely increased the proportion of more critically ill patients during the consolidation phase. This might have attenuated the observed impact on some outcomes. Finally, the absence of an external control group limits the possibility of making direct comparisons with other care models, and it was not possible to ensure full adherence to the program’s various interventions by all patients.
CONCLUSION
The implementation and consolidation of a specialized HF unit at our institution was associated with significant improvements in hospital efficiency, reflected primarily in a progressive and sustained reduction in length of hospital stay over a decade of experience.
It is important to note that, although the impact on inhospital mortality and 30-day hospital readmissions did not show statistically significant differences between the two periods analyzed, the greater stability and lower variability of these indicators during the consolidation phase suggest a sustained improvement in the quality of care provided.
These findings provide evidence about the feasibility and impact of structured specialized care programs with standardized processes for heart failure patients in Latin America. The observed success in reducing the length of hospital stay and the lower variability in clinical outcomes suggest that this type of model could be replicated in other regional settings, contributing to more effective, predictable, and sustainable care for this vulnerable population.