
Myxomas are the most common primary benign tumors of the heart. They account for approximately 50% of primary cardiac neoplasms and occur in the left atrium in about 75% of cases. (1,2) Large myxomas (> 5 cm) can cause significant functional mitral valve obstruction, systemic embolization, and hemodynamic involvement, thus requiring rigorous and timely surgical planning.
An aberrant right subclavian artery (ARSA) is the most common congenital defect of the aortic arch, with an estimated prevalence of 0.5% to 2% in the general population. (3) In most cases, it has a retroesophageal course and is asymptomatic. However, certain anatomical configurations, especially those associated with Kommerell's diverticulum or a proximal origin, can interfere with surgical maneuvers on the ascending aorta or aortic arch. (3-5)
We present the case of a 44-year-old female patient with progressive dyspnea (class III of the NYHA), in whom transthoracic Doppler echocardiography revealed a pedunculated left atrial mass measuring 5.5 × 3.7 cm protruding into the mitral plane and a mean gradient across the mitral valve of 12 mmHg (Figure 1). These findings were consistent with significant functional obstruction.
Fig. 1.
12-lead electrocardiogram: sinus rhythm, normal QRS axis, poor R wave progression and low QRS voltage in V4-V6.
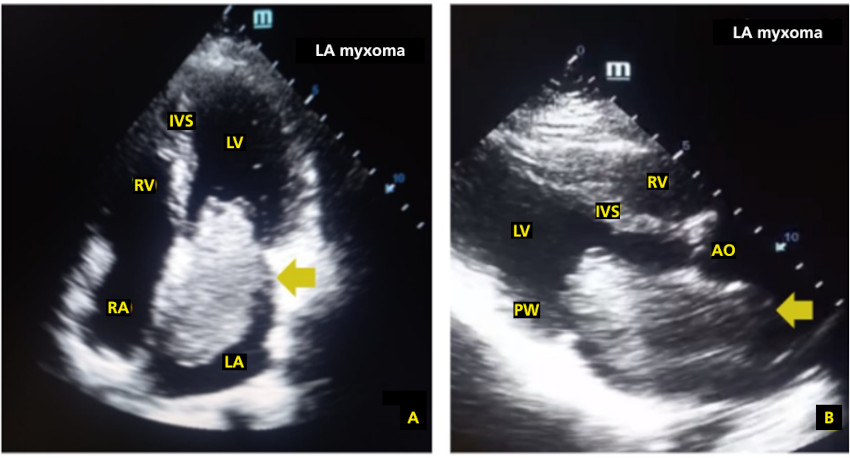
RA: right atrium; LA: left atrium; Ao: aorta; PW: posterior wall; IVS: interventricular septum; RV: right ventricle; LV: left ventricle
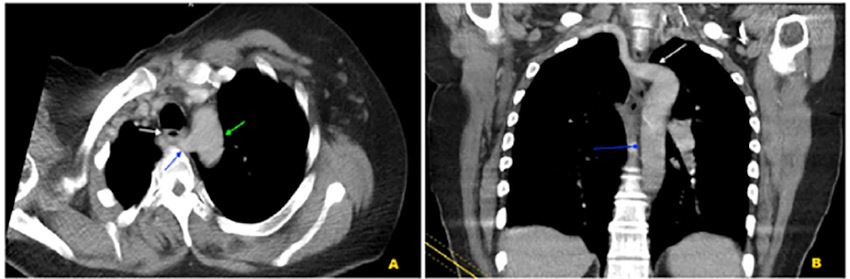
A cardiothoracic computed tomography angiography (CTA) confirmed the diagnosis of left atrial myxoma and incidentally identified an ARSA with a retroesophageal course and no evidence of aneurysmal dilatation or compression (Figure 2).
Fig. 2.
CT angiography: (A) Aberrant right subclavian artery with retroesophageal course. (B) Distal origin in the descending aorta
The vascular anomaly did not require the surgical technique to be modified, and the tumor was resected via a median sternotomy with standard ascending aortic cannulation. Nevertheless, potentially complex anatomical configurations were ruled out during preoperative assessment to reduce intraoperative uncertainty.
At 12 months of follow-up, the patient remained asymptomatic, with no tumor recurrence on follow-up echocardiography and stable ARSA.
The coexistence of atrial myxoma and ARSA is extremely rare, with no established direct embryological link between these conditions. (4) However, this case illustrates a clinically relevant aspect: the systematic identification of aortic arch variants using CT angiography can provide strategic information even when the anomaly does not modify the surgical technique. In cases where anatomical structures are less favorable, failure to acknowledge these variants may result in unplanned intraoperative decisions or an elevated technical risk.
Beyond the rarity of the association, the key message lies in the integration of multimodal imaging as a structured tool for preoperative planning in structural cardiac surgery. (6) The combination of echocardiography and computed tomography optimizes anatomical and functional tumor characterization and allows for comprehensive vascular mapping, enhancing operative safety.
In this context, the presented experience raises a broader question: preoperative vascular assessment should be considered part of a systematic planning strategy in structural cardiac surgery, not just in cases with clinical suspicion of an anomaly. Detailed vascular mapping can transform incidental findings into a tool for clinical precision and operative safety.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
Ethical considerations
Not applicable.