Juan M. Telayna1. MTSAC, Juan M. Telayna(h), Sofía Krause1, Horacio Fernandez1.MTSAC, Sergio Baratta1.MTSAC, Ricardo A. Costantini
1 Hospital Universitario Austral, Buenos Aires, Argentina.
Address for correspondence: Juan Manuel Telayna (h) - Hospital Universitario Austral. Av Presidente Perón 1500, 1629, Pilar, Bs As, Argentina - E-mail: JUTELAYN@cas.austral.edu.ar o jtelayna@gmail.com - Área de Investigación SAC - Azcuénaga 980 - CABA
Rev Argent Cardiol 2023;91:317-324. http://dx.doi.org/10.7775/rac.v91.i5.20668
ABSTRACT
Background and objectives: Early discharge (within the first 48 hours) in patients with ST-segment elevation myocardial infarction (STEMI) managed with primary percutaneous coronary intervention (PCI) with stenting is a strategy that has been adopted in developed countries.
However, its implementation in South America has been uneven.
Methods: We conducted an uncontrolled intervention pilot study on low-risk STEMI patients managed with primary PCI to evaluate the early discharge rate and compare the incidence of major adverse cardiovascular events (MACE) with those occurring in patients discharged later.
Results: Of 320 STEMI patients managed with primary PCI from 2013 to 2021, 158 were low-risk patients and 63.9% (95% CI 55.9-71,4%) of them were discharged early.
Diabetes (OR 0.31, 95% CI 0.12-0.83), and anterior wall STEMI (OR 0.34, 95% CI 0.16-0.69) were independently associated with lower probability of early discharge.
During a median follow-up period of 27.2 months, the incidence rate ratio of MACE between the early discharge and non-early discharge groups was 0.77 (95% CI 0.25-2.58; p = 0.61).
The variables independently associated with MACE were complete revascularization (HR 0.18, 95% CI 0.03-0.95) and fluoroscopy time (HR 1.02, 95% CI 1.01-1.05).
There were no significant differences in vascular access complications, 30-day readmission rate and overall survival between groups.
Conclusions: Early discharge in low-risk STEMI patients managed with primary PCI may be feasible even in developing countries, without significantly increasing morbidity and mortality.
Key words: Key words: Patient Discharge - Percutaneous Coronary Intervention - Myocardial Infarction - Coronaryartery Occlusion
RESUMEN
Introducción y objetivos: El alta hospitalaria temprana (dentro de las primeras 48 horas) en pacientes con infarto agudo de miocardio con elevación del segmento ST (IAMCEST) tratados con angioplastia coronaria primaria con stent (ATCp) ha sido adoptada en países desarrollados.
Sin embargo, su implementación en Sudamérica ha sido dispar.
Material y métodos: Estudio piloto de intervención no controlado, argentino, de pacientes con IAMCEST de bajo riesgo tratados con ATCp, para evaluar tasa de alta temprana y comparar la incidencia de eventos cardiovasculares adversos mayores (MACE) con la que ocurre en pacientes externados en forma no temprana.
Resultados: Desde 2013 hasta 2021 se trataron con ATCp 320 pacientes con IAMCEST, de los que 158 fueron de bajo riesgo. Alta temprana en 63,9% (IC 95% 55,9-71,4%).
La diabetes (OR 0,31; IC 95% 0,12-0,83) y el IAMCEST anterior (OR 0,34; IC 95% 0,16-0,69) se asociaron en forma independiente con menor probabilidad de alta temprana.
Durante una mediana de seguimiento de 27,2 meses, la razón de tasas de incidencia de MACE entre los grupos de alta temprana y no temprana fue de 0,77 (IC 95 % 0,25-2,58; p = 0,61).
Las variables asociadas de forma independiente con MACE fueron la revascularización completa (HR 0,18; IC 95% 0,03-0,95) y el tiempo de fluoroscopía (HR 1,02; IC 95% 1,01-1,05). No hubo diferencias significativas en las complicaciones del acceso vascular, las tasas de reingreso a 30 días y sobrevida global entre los grupos.
Conclusiones: El alta temprana en pacientes con IAMCEST de bajo riesgo tratados con ATCp puede ser factible incluso en países en desarrollo, sin aumento significativo de la morbimortalidad.
Palabras clave: Alta del paciente - Angioplastia - Infarto del miocardio - Oclusión coronaria
Received: 08/07/2023
Accepted: 9/20/2023
INTRODUCTION
Primary percutaneous coronary intervention (PCI) is the standard of care for ST-elevation myocardial infarction (STEMI) patients. (1)
During the last decade, PCI has demonstrated lower incidence of procedurerelated events, 30-day mortality and length of hospital stay. (2)
Technical advancements, such as radial access, have led to a reduction in adverse vascular events, improving patient care and outcomes. (3-5)
In this scenario, the length of stay in the coronary care unit (CCU) following primary PCI for STEMI patients has decreased, resulting in a reduction of resources used for medical care and hospital costs. (6)
In 2012, the European Society of Cardiology (ESC) suggested that early discharge of low-risk STEMI patients managed with primary PCI would not increase readmission or mortality rates. (7-9)
The European guidelines would consider recommending early discharge in low-risk patients with adequate follow-up. (10)
Other authors suggest that long length of stay in low-risk STEMI patients could be cost-effective. ((11).(12))
Therefore, early discharge could reduce health care costs. (13)
Early discharge after thrombolytic therapy has proved to be feasible. (14-18)
There are also recent data from Europe supporting early discharge 24 hours after STEMI. (19)
It remains unclear whether early discharge of low-risk STEMI patients is feasible or whether it increases the risk of readmission in other regions of the world. (20-23)
We hypothesized that early discharge after primary PCI in low-risk STEMI patients could be feasible and with no significant impact on major adverse cardiovascular events (MACE), even in a developing country. Therefore, we conducted this uncontrolled intervention pilot study to evaluate the feasibility of early discharge of STEMI patients managed with primary PCI (within the first 48 hours) at a university-based hospital in Argentina. We also compared the incidence rates of MACE among patients with and without early discharge.
METHODS
Study design and setting
In this prospective uncontrolled intervention pilot study, we included consecutive adult patients with uncomplicated STEMI managed with primary PCI in a South American center between November 2013 and June 2021. Hospital Universitario Austral is situated in Pilar, Buenos Aires, Argentina. Its operations began in the early 2000s, and it is accredited by the Joint Commission International. All the patients signed an informed consent form. The study protocol complied with the international ethical standards (N°13- 023) and was approved by the Institutional Review Board.
Eligibility
Low-risk STEMI adult patients were eligible for the study. Low-risk STEMI was defined following empirical criteria and previous publications as any MI with left ventricular ejection fraction (LVEF) of at least 50%, and with all the following conditions: 1) first MI; 2) STEMI within 12 h after symptom onset; 3) electrocardiogram (ECG) with STsegment elevation in no more than three contiguous leads; 4) successful PCI defined as residual stenosis < 20% after stent implantation with ST-segment resolution ≥ 50%; 5) absence of angina or angina equivalents, heart failure or low output volume syndrome, complex ventricular arrhythmia, mechanical complications or intraventricular thrombus; and, 6) clinical tolerance to medical treatment. All the patients should have signed the informed consent form. All eligible patients understood the likelihood and consequences of early discharge and approved and committed to subsequent follow-up programs.
Patients were excluded if they had at least one of the following conditions: 1) previous STEMI; 2) epiphenomenon; 3) LVEF < 50%; 4) acute coronary occlusion (stent thrombosis within 24 h); 5) failed PCI (residual stenosis >20% after stent implantation and final TIMI flow grade < 2); 6) hospital mortality within 48 h; and 7) anterolateral STEMI.
Procedures for early hospital discharge
After primary PCI, all the patients were admitted in the CCU. An echocardiogram was performed to evaluate heart valves, wall motion and LVEF. Cardiac monitoring, ECG and laboratory tests were performed following the usual standards. Eligible patients were invited to participate in the study within 48 h of observation.
Early discharge was canceled in the presence of any of the following events: need for mechanical ventilation, severe life-threatening arrhythmias, mechanical complications, post-MI pericarditis, systemic or vascular access bleeding according to GUSTO criteria, stroke or transient ischemic attack, acute renal failure, severe infection, decision to treat a non-culprit artery after 48 hours in the index hospitalization, or any other complication that necessitated postponement of discharge. These events were recorded to estimate the overall proportion and feasibility of early discharge in the entire population of STEMI patients.
Before being discharged, patients were given precise instructions on alarm signs and how to maintain a healthy lifestyle according to existing protocols. In addition, they were provided with the telephone numbers of the interventional cardiologist and ICU physician. Clinical follow-up was carried out in clinics 7 and 30 days after discharge, continuing thereafter with the usual care provided by the treating physician.
Exposure variables
Data were collected from the information prospectively recorded in an electronic case report form (CRF) The information recorded included: 1) demographic data: age, and gender; 2) past medical history and risk factors: previous coronary artery bypass grafting (CABG), previous PCI, peripheral vascular disease, kidney failure, dyslipidemia, diabetes, hypertension, smoking habits, infarct location, Killip-Kimball (K-K) class, and use of glycoprotein IIb/IIIa inhibitors; 3) angiographic data: number of diseased vessels, treated vessels, lesion segment (CASS classification), presence of thrombus, bifurcation, chronic total occlusion, complete revascularization, baseline and final TIMI flow/blush, lesion length, use of thrombus aspiration, intravascular ultrasound (IVUS), stent diameter and length, duration of the procedure, amount of contrast, and fluoroscopy time.
PCI protocol
All the patients received dual antiplatelet therapy before the procedure (aspirin 325 mg and clopidogrel 600 mg or prasugrel 60 mg or ticagrelor 180 mg). The Allen test was performed before radial artery cannulation. The use of IVUS was not mandatory. The decision on how and when to complete revascularization, perform thrombus aspiration or use IIb/IIIa inhibitors was left to the operator's discretion on a case-by-case basis. All the patients received a stent.
Definition of events and statistical analysis
Categorical variables are expressed as frequencies and percentages and compared using the chi-square test or Fisher's test, as applicable. Continuous variables are presented as mean and standard deviation (SD), or median and interquartile range (IQR), as appropriate. To compare the data, the t-test was used for normal distributions, and the Mann- Whitney test was used for non-normal distributions.
The primary endpoint was the overall proportion of early discharge (up to 48 hours) of STEMI patients managed with primary PCI with the corresponding 95% CI. The overall proportion of early discharge was calculated by considering the ratio of patients who were discharged early divided by the total population eligible for the study. The secondary endpoints included MACE, vascular access complications and rate of readmissions at 30 days. MACE was defined as a composite of cardiovascular and non-cardiovascular death, reintervention (PCI or CABG), and stroke. Vascular access complications were radial artery occlusion with regional ischemia, need for surgical repair, arteriovenous fistula, pseudoaneurysm, major bleeding (requiring transfusion or surgical repair) or radial hematoma > grade III. Readmission was defined as any new cardiovascular event requiring hospitalization within 30-day follow-up after primary PCI.
Multivariable logistic regression analysis was performed to generate prediction models for early discharge, estimating the odds ratio (OR) and their corresponding 95% CI of the patients' baseline characteristics and angiographic variables. The calibration of each final model was assessed by the Hosmer-Lemeshow test, and the discriminatory power using the area under the ROC curve.
We also calculated the incidence rate and incidence rate ratio for MACE and death. Time-to-event data was analyzed with Kaplan-Meier survival curves and the groups were compared using the log-rank test. Multivariate Cox regression analysis was conducted to identify those variables that were independently associated with the development of MACE. The analysis also addressed the effect of early discharge on mortality as well as confounding factors, with estimation of the hazard ratios (HR) and their corresponding 95% CI. The proportional hazard assumptions were evaluated by graphical diagnostics based on Schoenfeld residuals and log-plots. A two-tailed p value < 0.05 was considered statistically significant. All the statistical calculations were performed using STATA BE 17.0 software package.
RESULTS
Between November 2013 and June 2021, 320 consecutive patients with STEMI were managed with primary PCI at Hospital Universitario Austral. The baseline characteristics of the population are described in Table 1. Median door-to-balloon time was 92 minutes (IQR 70-120). Multivessel disease was present in 49.7% of the patients (n = 159) and compete revascularization was achieved in 76.1% (n = 121). The radial access was used in 77.2% (n = 247) of cases and the median number of stents implanted was 2 per patient (IQR 1-3).
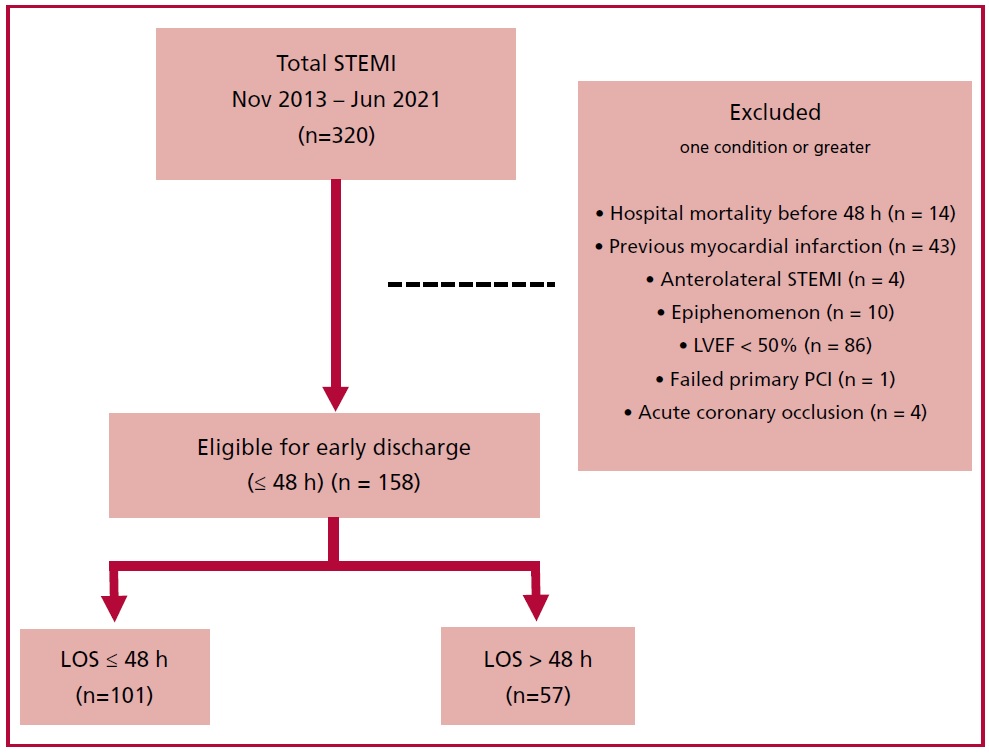
After excluding patients who died within 48 hours (n=14), those with a history of previous MI (n=43), anterolateral STEMI (n=4), STEMI as an epiphenomenon (n=10), LVEF < 50% (n=86), failed PCI (n=1), and acute coronary occlusion (n=4), a total of 158 patients were eligible for early discharge (within the first 48 hours) (Figure 1).
Feasibility and early discharge rates
Among STEMI patients, 31.6% (95% CI 26.5-37%; 101/320) were discharged within 48 hours. When only eligible patients were considered, the proportion was 101/158 (63.9%, 95% CI 55.9-71.4%). Mean length of hospital stay was 2 days (IQR 2-2) in the early discharge group versus 3 (IQR 2-4) in the other group (p < 0.00001).
Patients who remained in hospital for more than 48 hours (n=57) presented a higher prevalence of diabetes (21% vs. 8.9%; p = 0.03) and anterior wall STEMI (45.6% vs. 23.8%; p = 0.005) with occlusion of the anterior descending coronary artery (45.6% vs. 24.7%; p = 0.02). Within this group, a higher percentage of patients received complete revascularization of non-culprit arteries during the index hospitalization (60.8% vs, 10.2%; p < 0.0001). However, within the early discharge group, a higher percentage of patients received complete revascularization of non-culprit arteries during the index procedure (51.3% vs. 26.1%; p = 0.07) (Table 2). Table 3 shows crude and adjusted OR for the likelihood of early discharge. Diabetes (OR 0.31, 95% CI 0.12-0.83), and anterior wall STEMI (OR 0.34, 95% CI 0.16-0.69) were independently associated with lower probability of early discharge.
Table 1. Baseline characteristics of STEMI patients between 2013-2021 (n = 320)
|
Variable |
Value |
|
Age,
years (± SD) |
60 ± 11 |
|
Male
gender, n (%) |
273 (85.3) |
|
Diabetes
mellitus, n (%) |
58 (18.1) |
|
Hypertension, n (%) |
181 (56.6) |
|
Smoking
habits, n (%) |
202 (63.1) |
|
Dyslipidemia,
n (%) |
151 (47.2) |
|
Previous
PCI, n (%) |
66 (20.6) |
|
Previous
AMI, n (%) |
49 (15.3) |
|
Anterior
wall STEMI, n (%) |
151 (47.2) |
|
Killip-Kimball class, n (%) A B C D |
266 (83.1) 40 (12.5) 5 (1.5) 9 (2.8) |
|
LVEF,
% (± SD) |
50.8 ± 12.5 |
AMI: acute myocardial infarction; IQR: interquartile range; LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention; SD: standard deviation; STEMI: ST-segment elevation myocardial infarction.
LVEF: left ventricular ejection fraction; LOS: length of hospital stay; MI: myocardial infarction; PCI: percutaneous coronary intervention; STEMI: ST-segment elevation myocardial infarction. Note: 162 of 320 patients were excluded. Some patients could have more than one exclusion criteria.
Main results in patient with early discharge and non-early discharge
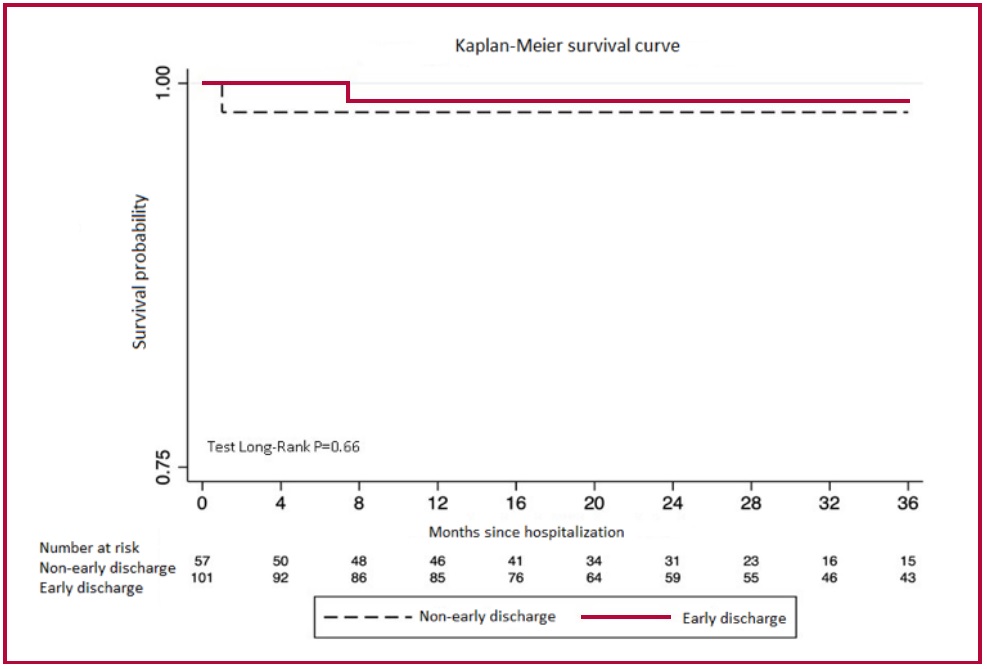
During a median follow-up period of 27.2 months (IQR16-43.5), patients who were discharged early had a 1-year survival rate of 98.8% (95% CI 92.1- 99.8), while patients who were not discharged early had a 1-year survival rate of 98.1% (95% CI 87.1-99.7; p=0.66) (Figure 2). The MACE incidence rate was 3.1 per 1000 person-months in the enrolled population, with similar rates between groups (early discharge 3.1 vs. non-early discharge 4.0 per 1000 person-months of follow-up). The incidence rate ratio of MACE was 0.77 (95% CI: 0.25-2.58; p = 0.61). The median time to MACE was 10.5 months (IQR 2.4-26.3) in the early discharge group versus 22.3 months (IQR 1-39.9) in the non-early discharge group (p = 0.89). The variables independently associated with MACE were complete revascularization (HR 0.18, 95% CI 0.03-0.95) and fluoroscopy time (HR 1.02, 95% CI 1.01-1.05). Finally, vascular event rate and 30-day readmission rate were not significantly different between the groups.
Twenty-two patients in the early discharge group left the hospital after 24 hours, with no major events, most of them during the COVID-19 pandemic. In fact, during the pandemic (from March 2020 to December 2022 in our country), 28 of 128 low-risk STEMI patients (21.8%) were discharged within 24 hours of PCI. However, during the time frame between the end of our study and the presentation of this paper (July 2021 to February 2023), only 10 out of 78 lowrisk STEMI patients (12.8%) were discharged within 24 hours.
DISCUSSION
In our prospective pilot intervention study, we observed that early hospital discharge in the STEMI population may be feasible in 1 in 3 patients. This number increased to 2 in 3 in low-risk STEMI patients. Second, early discharge was less probable in patients with diabetes or with anterior wall STEMI. Third, discharge before 48 hours was not associated with an increased risk of MACE or death during longterm follow-up. Patients with complete revascularization had lower risk of MACE.
In Argentina, early discharge of STEMI patients is not a usual practice, and national guidelines do not consider this alternative. In view of the recommendations of international guidelines and the results obtained in our hospital, we decided to perform a prospective, uncontrolled intervention study to evaluate the rate of early discharge (≤48 hours after primary PCI) in all the patients with STEMI and in low-risk patients. (24) Therefore, this is the first intervention study to evaluate early discharge after primary PCI of STEMI patients in our country.
Revascularization of STEMI patients has steadily improved. In addition, the use of various clinical risk scores (11) to identify a population of patients with low-risk STEMI has promoted consideration of early discharge after primary PCI due to improved management and economic considerations.
Few decades ago, some authors demonstrated that shorter hospitalization was not associated with higher mortality. (25) The Zwolle group created a practical risk assessment tool to categorize STEMI patients following primary PCI, allowing for identification of those at low risk for cardiovascular events.(26)
Unlike previous studies, (27,28) we reduced hospital stay to 48 hours and included patients with LVEF of at least 50%. Finally, multivessel disease was not an exclusion criterion. In fact, complete revascularization was performed even within the scheduled time for early discharge. Our study is more recent and reflects the current state of practice in terms of procedure, type of stent used, and pharmacologic framework.
A Norwegian study randomized STEMI patients to early discharge or usual care and showed no differences in 30-day mortality between both groups. (29) En nuestro estudio no hemos tenido eventos tras el alta y, a diferencia de estos autores, el alta fue dentro de las 48 horas.
In our study there were no events after discharge and, unlike these authors, patients were discharged within 48 hours.
In conclusion, this is the first pilot uncontrolled intervention study in Argentina that demonstrates the feasibility of early discharge for low-risk STEMI patients undergoing primary PCI. The incidence of clinical events and readmissions were low.
Table 2. Comparative analysis between patients early discharged within 48 h and those with longer length of hospital stay.
|
Variable |
Early discharge (n = 101, 63.9%) |
Non-early discharge (n = 57,
36.9%) |
p |
|
Age, years (± SD) |
57.2 ± 11.2 |
58.3 ± 10.5 |
0.523 |
|
Male gender, n (%) |
85 (84.2) |
50 (87.7) |
0.541 |
|
Diabetes mellitus, n (%) |
9 (8.9) |
12 (21) |
0.033 |
|
Hypertension, n
(%) |
50 (49.5) |
28 (49.1) |
0.924 |
|
Smoking habits, n (%) |
65 (64.4) |
33 (57.9) |
0.421 |
|
Dyslpidemia, n (%) |
42 (40.6) |
30 (52.6) |
0.145 |
|
Previous PCI, n (%) |
9 (8.9) |
9 (15.8) |
0.156 |
|
Anterior wall STEMI, n (%) |
24 (23.8) |
26 (45.6) |
0.005 |
|
Killio-Kimball class, n (%) A B C D |
98 (97) 3 (3) 0 0 |
55 (96.5) 2 (3.5) 0 0 |
1.0 - |
|
LVEF, % (± SD) |
60.1 ± 8.0 |
58.8 ± 7.0 |
0.334 |
|
Median door-to-balloon time, minutes (IQR) |
93 (71-124) |
90 (62-118) |
0.246 |
|
Culprit artery, n (%) LAD RCA LCx |
25 (24.7) 49 (48.5) 27 (26.7) |
26 (45.6) 18 (31.5) 13 (22.8) |
0.022 |
|
Multivessel disease, n (%) |
42 (41.6) |
27 (47.4) |
0.481 |
|
Complete revascularization, n (%) |
39 (92.9) |
23 (85.2) |
0.302 |
|
Complete revascularization, n
(%) Same session Same hospitalization At 30 days |
20 (51.3) 4 (10.2) 15 (38.5) |
6 (26.1) 14 (60.8) 3 (13.04) |
0.073 <0.0001 0.042 |
|
Bifurcation, n (%) |
3 (2.9) |
4 (7) |
0.256 |
|
Baseline TIMI flow grade 0-1,
n (%) |
60 (59.4) |
35 (61.4) |
0.804 |
|
Radial access, n (%) |
89 (88.1) |
47 (82.5) |
0.328 |
|
7-8 Fr introducer, n (%) |
4 (13.9) |
8 (3.8) |
0.082 |
|
|
|
|
|
|
Thrombus aspiration, n (%) |
8 (7.9) |
7 (12.3) |
0.403 |
|
Direct stenting, n (%) |
23 (22.7) |
9 (15.8) |
0.292 |
|
Median stents in index
procedure (IQR) |
2 (1-3) |
2 (1-2) |
0.754 |
|
Mean stent diameter, mm (± SD) |
2.9 ±
0.4 |
3.0 ±
0.5 |
0.226 |
|
Median stent length, mm (IQR) |
34 (23-49) |
35 (23-59) |
0.492 |
|
IIb-IIIa, n (%) |
7 (6.9) |
8 (14) |
0.163 |
|
IVUS, n (%) |
2 (1.9) |
3 (5.2) |
0.352 |
|
Median fluoroscopy time,
minute (IQR) |
9.1 (6.5-12.4) |
9 (6.4-14.1) |
0.536 |
|
Median contrast volume, mL (IQR) |
160 (140-201) |
160 (129-200) |
0.394 |
AMI: acute myocardial infarction; IIb-IIIa: IIb-IIIa glycoprotein inhibitors; IQR: interquartile range; IVUS: intravascular ultrasound; LAD: left anterior descending coronary artery; LCx: left circumflex coronary artery LVEF: left ventricular ejection fraction; PCI: percutaneous coronary intervention; RCA: right coronary artery SD: standard deviation; TIMI: Thrombolysis in Myocardial Infarction.
Table 3. Variables associated with early discharge. Logistic regression analysis.
|
Variable |
Unadjusted OR (95% CI) |
p |
Adjusted OR (95% CI) |
p |
|
Diabetes mellitus Yes (n = 21) No (n = 137) |
0.37 (0.14-0.93) - |
0.036 |
0.31 (0.12-0.83) - |
0.019 |
|
Anterior wall STEMI Yes (n = 50) No (n = 108) |
0.37 (0.18-0.74) - |
0.005 |
0.34 (0.16-0.69) - |
0.003 |
|
Culprit artery LAD (n=51) RCA (n = 87) LCx (n = 40) |
Ref 2.83 (1.31-6.11) 2.16 (0.91-5.1) |
- 0.008 0.08 |
|
|
|
Complete
revascularization in the
index hospitalization Yes (n = 18) No (n = 44) |
0.07 (0.02-0.28) - |
<0.0001 - |
|
|
STEMI: ST-segment elevation myocardial infarction; LAD: left anterior descending coronary artery; LCx: left circumflex coronary artery; RCA: right coronary artery. Notes: The adjusted OR column shows the variables with statistical significance on multivariate analysis. The p value for calibration of the model with Hosmer-Lemeshow test was 0.76. Area under the ROC curve 0.66 (95% CI 0.58-0.73)
Fig 2: Kaplan-Meier survival analysis
Study limitations
One of the limitations of our study is the intervention design in the absence of a control group (without evaluating the effect of random assignment). Therefore, different unknown confounding factors have not been evaluated. However, we adjusted for the effect of known confounding variables in a multivariable model and, on the other hand, designing and executing a controlled study was not feasible.
This is a single-center study conducted on a relatively small sample. In addition, the population is young, and the prevalence of women is low. We did not assess clinical factors such as anemia or chronic renal failure that could impede early discharge. However, this is the first regional protocol on this subject. There may also be the biases inherent to the nature of a registry. But this approach reflects real patients who were selected using previously validated inclusion criteria and who received second- and third-generation drug-eluting stents.
CONCLUSION
Our data show that in a significant number of lowrisk STEMI patients managed with primary PCI and stenting, early discharge within 48 hours may be feasible. An economic analysis should be conducted to evaluate the reduction in hospital costs without increasing MACE.
Outpatient procedures and early discharge are increasingly utilized by institutions to reduce length of hospital stay and decrease adverse in-hospital events.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web/Additional material).
https://creativecommons.org/licenses/by-nc-sa/4.0/

©Revista Argentina de Cardiología
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Acknowledgments
We would like to thank Dr. Federico Piñero for his cooperation.
BIBLIOGRAFÍA
- Wijns W, Kolh P, Danchin N, Di Mario C, Falk V, Folliguet T, et al. Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS); European Association for Percutaneous Cardiovascular Interventions (EAPCI); Guidelines on myocardial revascularization. Eur Heart J. 2010;31:2501-55. https://doi.org/10.1093/eurheartj/ehq277
- Kiemeneij F, Laarman GJ, Odekerken D, Slagboom T, van der Wieken R. A randomized comparison of percutaneous transluminal coronary angioplasty by the radial, brachial and femoral approaches: the access study. J Am Coll Cardiol. 1997;29:1269-75. https://doi.org/10.1016/s0735-1097(97)00064-8
- Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, et al. RIVAL trial group. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): a randomised, parallel group, multicentre trial. Lancet. 2011;377:1409-20. https://doi.org/10.1016/S0140-6736(11)60404-2.
- Intorre M, Costantini RA, Telayna JM, García C. Abordaje radial y femoral en angioplastia primaria. XVII Congreso Sociedad Latinoamericana de Cardiología Intervencionista 3 - 5 de agosto de 2011 (Poster 019).
- Telayna JM, Costantini R, García C. Transradial percutaneous coronary angioplasty in acute myocardial infarction. J Heart Dis 2012;9:109. Abstract 436.
- Stathopoulos I, Jimenez M, Panagopoulos G, Kwak EJ, Losquadro M, Cohen H, et al. The decline in PCI complication rate: 2003-2006 versus 1999-2002. Hellenic J Cardiol. 2009;50:379-87.
- Steg PG, James SK, Atar D, Badano LP, Blömstrom-Lundqvist C, Borger MA, et al. Task Force on the management of ST-segment elevation acute myocardial infarction of the European Society of Cardiology (ESC). ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2012;33:2569-619. https://doi.org/10.1093/eurheartj/ehs215
- Spencer FA, Lessard D, Gore JM, Yarzebski J, Goldberg RJ. Declining length of hospital stay for acute myocardial infarction and postdischarge outcomes: a community-wide perspective. Arch Intern Med. 2004;164:733-40. https://doi.org/10.1001/archinte.164.7.733
- Berger AK, Duval S, Jacobs DR Jr, Barber C, Vazquez G, Lee S, et al. Relation of length of hospital stay in acute myocardial infarction to postdischarge mortality. Am J Cardiol. 2008;101:428-34. https://doi.org/10.1016/j.amjcard.2007.09.090
- Ibanez B, James S, Agewall S, Antunes MJ, Bucciarelli-Ducci C, Bueno H, et al. ESC Scientific Document Group. 2017 ESC Guidlines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39:119-77. https://doi.org/10.1093/eurheartj/ehx393
- De Luca G, Suryapranata H, van ‘t Hof AW, de Boer MJ, Hoorntje JC, Dambrink JH, et al. Prognostic assessment of patients with acute myocardial infarction treated with primary angioplasty: implications for early discharge. Circulation. 2004;109:2737-43. https://doi.org/10.1161/01.CIR.0000131765.73959.87
- Newby LK, Hasselblad V, Armstrong PW, Van de Werf F, Mark DB, White HD, et al. Time-based risk assessment after myocardial infarction. Implications for timing of discharge and applications to medical decision-making. Eur Heart J. 2003;24:182-9. https://doi.org/10.1016/s0195-668x(02)00301-9
- Zhan C, Miller MR. Excess length of stay, charges, and mortality attributable to medical injuries during hospitalization. JAMA. 2003;290:1868-74. https://doi:.org/10.1001/jama.290.14.1868
- Topol EJ, Burek K, O’Neill WW, Kewman DG, Kander NH, Shea MJ, et al. A randomized controlled trial of hospital discharge three days after myocardial infarction in the era of reperfusion. N Engl J Med. 1988;318:1083-8. https://doi.org/10.1056/NEJM198804283181702
- Sanz G, Betriu A, Oller G, Matas M, Magriñá J, Paré C, et al. Feasibility of early discharge after acute Q wave myocardial infarction in patients not receiving thrombolytic treatment. J Am Coll Cardiol. 1993;22:1795-801. https://doi.org/10.1016/0735-1097(93)90759-t
- Mark DB, Sigmon K, Topol EJ, Kereiakes DJ, Pryor DB, Candela RJ, et al. Identification of acute myocardial infarction patients suitable for early hospital discharge after aggressive interventional therapy. Results from the Thrombolysis and Angioplasty in Acute Myocardial Infarction Registry. Circulation. 1991;83:1186-93. https://doi.org/10.1161/01.cir.83.4.1186
- Newby LK, Califf RM, Guerci A, Weaver WD, Col J, Horgan JH, et al. Early discharge in the thrombolytic era: an analysis of criteria for uncomplicated infarction from the Global Utilization of Streptokinase and t-PA for Occluded Coronary Arteries trial. J Am Coll Cardiol. 1996;27:625-32. https://doi.org/10.1016/0735-1097(95)00513-7
- Grines CL, Marsalese DL, Brodie B, Griffin J, Donohue B, Costantini CR, et al. Safety and cost-effectiveness of early discharge after primary angioplasty in low risk patients with acute myocardial infarction. PAMI-II Investigators. Primary Angioplasty in Myocardial Infarction. J Am Coll Cardiol. 1998;31:967-72. https://doi.org/10.1016/s0735-1097(98)00031-x
- Rathod KS, Comer K, Casey-Gillman O, Moore L, Mills G, Ferguson G, et al. Early Hospital Discharge Following PCI for Patients With STEMI. J Am Coll Cardiol. 2021;78:2550-60. https://doi.org/10.1016/j.jacc.2021.09.1379
- Kotowycz MA, Cosman TL, Tartaglia C, Afzal R, Syal RP, Natarajan MK. Safety and feasibility of early hospital discharge in ST-segment elevation myocardial infarction--a prospective and randomized trial in low-risk primary percutaneous coronary intervention patients (the Safe-Depart Trial). Am Heart J. 2010;159:117.e1-6. https://doi.org/10.1016/j.ahj.2009.10.024
- Karabulut A, Cakmak M, Uzunlar B, Bilici A. What is the optimal length of stay in hospital for ST elevation myocardial infarction treated with primary percutaneous coronary intervention? Cardiol J. 2011;18:378-84
- Gong W, Li A, Ai H, Shi H, Wang X, Nie S. Safety of early discharge after primary angioplasty in low-risk patients with ST-segment elevation myocardial infarction: A meta-analysis of randomised controlled trials. Eur J Prev Cardiol. 2018;25:807-15. https://doi.org/10.1177/2047487318763823
- Jones DA, Rathod KS, Howard JP, Gallagher S, Antoniou S, De Palma R, et al. Safety and feasibility of hospital discharge 2 days following primary percutaneous intervention for ST-segment elevation myocardial infarction. Heart. 2012;98:1722-7. https://doi.org/10.1136/heartjnl-2012-302414
- Telayna JM, Costantini R. Resultados de 10 años de tratamiento percutáneo del infarto agudo de miocardio. Rev Argent Cardioangiol Interv 2010;l2:152.
- Berger AK, Duval S, Jacobs DR Jr, Barber C, Vazquez G, Lee S, et al. Relation of length of hospital stay in acute myocardial infarction to postdischarge mortality. Am J Cardiol. 2008;101:428-34. https://doi.org/10.1016/j.amjcard.2007.09.090.
- Tralhão A, Ferreira AM, Madeira S, Borges Santos M, Castro M, Rosário I, et al. Applicability of the Zwolle risk score for safe early discharge after primary percutaneous coronary intervention in ST-segment elevation myocardial infarction. Rev Port Cardiol. 2015;34:535-41. https://doi.org/10.1016/j.repc.2015.04.006.
- Noman A, Zaman AG, Schechter C, Balasubramaniam K, Das R. Early discharge after primary percutaneous coronary intervention for ST-elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2013;2:262-9. https://doi.org/10.1177/2048872612475231
- Azzalini L, Solé E, Sans J, Vila M, Durán A, Gil-Alonso D, et al. Feasibility and safety of an early discharge strategy after low-risk acute myocardial infarction treated with primary percutaneous coronary intervention: the EDAMI pilot trial. Cardiology. 2015;130:120-9. https://doi.org/10.1159/000368890
- Melberg T, Jørgensen M, Ørn S, Solli T, Edland U, Dickstein K. Safety and health status following early discharge in patients with acute myocardial infarction treated with primary PCI: a randomized trial. Eur J Prev Cardiol. 2015;22:1427-34. https://doi.org/10.1177/2047487314559276