REVIEW ARTICLE
What Are We Talking About When We Talk About
Palliative Care in Heart Failure?
¿De qué hablamos
cuando hablamos de cuidados paliativos en insuficiencia cardíaca?
Mariángel Sánchez1,
Francisco Proasi2, Luis Ahualli1, Claudio Higa1, MTSAC
1 Division of
Cardiology. Department
of Internal Medicine. Hospital Alemán.
Buenos Aires. Argentina
2 Division of
Palliative Care. Department of Internal Medicine. Hospital Alemán.
Buenos Aires. Argentina
Address for reprints: mariangelsanchez@hospitalaleman.com Avenida
Pueyrredón 1640. Ciudad Autónoma de Buenos Aires. Argentina. CPC 1118AAT tel (+5411) 48277000
Rev Argent Cardiol 2023;91:273-278.
http://dx.doi.org/10.7775/rac.v91.i4.20654
ABSTRACT
Background: Heart failure is a chronic, complex and
progressive disease, with high morbidity and mortality, and growing prevalence.
Despite advances in therapeutic strategies to improve survival and reduce
hospitalizations, heart failure still generates a negative impact on the
patients’ quality of life, making it necessary to develop health policies based
not only on their physical but also on their psychosocial integrity. Palliative
care refers to specialized, interdisciplinary care focused on improving the
quality of life of patients who suffer a disease with elevated morbidity and
mortality. The aim of this review is to assess the impact of the implementation
of palliative care in the multidisciplinary treatment of heart failure
throughout all the stages of the disease, and to determine the feasibility of
its application in clinical practice.
Key words: Heart failure - Palliative care - Prognosis
RESUMEN
La
insuficiencia cardíaca (IC) es una enfermedad crónica, compleja y progresiva,
con elevada morbimortalidad y creciente prevalencia. Pese al avance en las
estrategias terapéuticas, destinadas a mejorar la sobrevida y reducir
hospitalizaciones, la IC continúa generando un impacto negativo en la calidad
de vida de los pacientes. Surge ante este reto la necesidad de desarrollar
políticas de salud basadas no solo en la integridad física, sino también en la
integridad psicosocial. Los cuidados paliativos (CP) hacen referencia a un
cuidado especializado, interdisciplinario, enfocado en mejorar y mantener la
calidad de vida de los pacientes que se enfrentan a una enfermedad con elevada
morbimortalidad como lo es la IC. El propósito de la presente revisión es evaluar
el impacto de la integración de los CP en el tratamiento multidisciplinario de
la IC en todas las fases de la enfermedad y determinar la factibilidad de su
aplicación en la práctica clínica.
Palabras
clave: Insuficiencia cardíaca - Cuidados
paliativos - Pronóstico
Received: 07/04/2023
Accepted: 07/28/2023
INTRODUCTION
Heart failure (HF) is a complex syndrome whose
prevalence has increased in the last years as a result of population aging, the
presence of multiple comorbidities and the higher survival of cardiovascular
diseases. (1-3) Despite the development of therapeutic strategies
destined to reduce mortality, HF is associated with elevated morbidity and
progressive functional impairment. (4) Moreover, decompensations
represent one of the main causes of hospitalization in adults over 65 years of
age, with a high rate of rehospitalizations. (5) Several authors have demonstrated a negative impact
on the quality of life of patients with HF due to the limitation in functional
class (FC), loss of independence in daily life activities and presence of
physical symptoms and mood changes (comparable or greater to those of
oncological patients) that are occasionally underdiagnosed and undertreated. (6-8).
The World Health Organization (WHO) acknowledges
palliative care (PC) as “an approach to improve the quality of life of patients
and their relatives facing problems associated with a potentially mortal
disease. It includes the prevention and the relief of suffering through the
early identification, assessment and corrective treatment of pain and other
problems, whether physical, psychosocial or spiritual. (9) In oncological patients, the early intervention of PC
teams has been shown to improve the quality of life and reduce costs and
hospital admissions. It is therefore interesting to evaluate if patients with
HF could also benefit from the care provided by the different PC levels.
The aim of the present review is to assess the
existing evidence on the impact of incorporating PC to the multidisciplinary
treatment of HF, the limiting factors in its application and its feasibility in
daily clinical practice.
PALLIATIVE CARE
Originally, PC was developed within the frame of care
of end-stage oncological patients, with the purpose of achieving symptomatic
end-of-life control. (10) The growing prevalence of chronic, non-communicable
diseases and the morbidity and mortality they generate has led to a transition
from the classical model of care in which PC was administered in end-stage
patients, towards a model of integral care which emphasizes the early onset of
PC together with the active treatment of the disease. In this last model, as
the disease progresses and the needs of the patient increase, PC is intensified
to accompany the patient and his/her relatives, even contemplating the care of
the family during the mourning process after the patient’s death. This
organizational model generates a paradigm in the care of the chronic patient,
in which both the curative and palliative treatments are similarly rated,
allowing a dynamic and integral care that leaves behind the original concept of
PC focused on end-of-life treatment (11-13) (Figure 1).
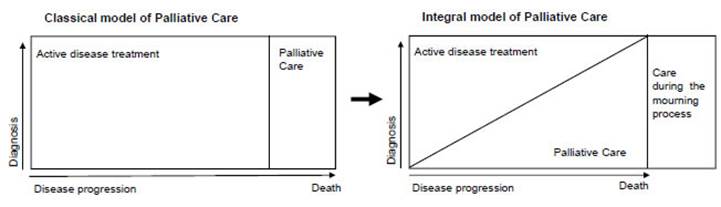
Fig.
1. Transition from the classical model
of palliative care towards an integral care model, which emphasizes the early
onset of palliative care, together with an active treatment of the disease.
Modified from Lynn J, Adamson DM. Living well at the end of life; adapting
health care to serious chronic illness in old age. WHO
regional office for Europe. 2004.
In patients with chronic diseases, PC has shown a
consistent benefit in terms of quality-of-life improvement, symptomatic
control, reduction of hospitalizations and increase in anticipated measures
that prioritize comfort over invasive measures at the end of life, with the
consequent reduction in health costs, which avoids futility. (14,15)
Three levels of care are identified in PC. (16,17)
- First level or primary PC: it involves the
application of basic PC competencies by first level of care professionals to
provide symptomatic control in patients.
- Second level or secondary PC: it consists of
interdisciplinary care in which the PC teams are consulted and deliver
complementary support. The specific structure of each team varies according to
the patient’s needs. (11)
- Third level or tertiary PC: care is carried out in
healthcare centers with specialized PC teams. It provides care to very complex
patients who need hospitalization.
Access to PC has been declared a universal human
right. (18) According to WHO, Argentina is among the countries
with active growth in PC. (11) However, there is inequity in its access. The
National Palliative Care Law was enacted in 2022 to guarantee PC access in all
the care settings.
Application of palliative care in heart failure: let´s
go to the evidence
In the prospective, randomized and open-label PRE-FER
study, an integral PC home monitoring model together with cardiologists
specialized in HF was compared with only the latter monitoring strategy in NYHA
FC III-IV HF patients (36 patients per group). The Edmonton symptoms assessment
scale (ESAS) and the Kansas City Cardiomyopathy Questionnaire (KVCQ) were used
to analyze results. The first refers to a tool evaluating the average intensity
of symptoms such as pain, dyspnea, asthenia, nausea, depression, anxiety,
welfare, poor appetite and insomnia during a period of time. The second
corresponds to a self-administered questionnaire specific for HF, consisting of
23 items that involve 5 self-perceived dimensions regarding the patient’s
health condition: physical limitation, symptoms (frequency, severity and
stability), self-care, quality of life and social limitation. The PC strategy
together with HF specialists demonstrated a statistically significant
improvement in the quality of life compared with the control group (p=0.05) as
well as improved symptom burden (p=0.035). The implementation of integral care
evidenced a significant change in FC at 6 months compared with control (39% vs.
10%, p=0.012). Additionally, the intervention group reduced hospitalizations
(p=0.009). (19). These findings are consistent with those reported by
Wong et al. who showed a reduction in the number of readmissions and
symptomatic improvement with a PC strategy in patients discharged after a
hospitalization for HF. (20)
In the PAL-HF study, 150 patients with advanced HF (AdHF) were randomly allocated to receive standard medical
care, vs. the latter together with PC monitoring. Mean age was 71 years and
more than 70% were in NYHA FC III, with an average of 2.2 hospitalizations in
the year prior to enrollment. KCCQ scores evidenced poor quality of life, with
a high symptom burden. The KCCQ and the Functional Assessment of Chronic
Illness Therapy Palliative Care scale (FACITPal) were
used to analyze the results. The latter refers to a 46-item self-administered
questionnaire evaluating quality of life in the physical, socio-familial,
emotional and functional domains and also includes specific PC aspects. A
change in favor of patients assigned to the PC interdisciplinary monitoring arm
was observed with a KCCQ difference of 9.49 points (95% CI 0.94-18.05; p=0.030)
and a difference in the FACIT-Pal scale of 11.77 points (95% CI 0.84-22.71;
p=0.035) compared with patients undergoing conventional monitoring at 6 months
of follow-up. In addition, a significant benefit was observed in the degree of
anxiety (p=0.048) and depression (p=0.020), also in favor of interdisciplinary
monitoring. (21)
In a systematic review of randomized controlled
clinical trials including 1050 AdHF patients, the
implementation of PC plus standard care was compared with standard care alone.
The integral PC monitoring combined with standard care was associated with
improved quality of life, reduced number of hospitalizations (OR 0.56; 95% CI
0.33-0.94) and decreased symptom burden compared with the usual care. (22)
These findings indicate a consistent benefit in terms
of quality of life and symptom burden improvement in patients with AdHF. However, it is necessary to emphasize the difficulty
posed by the incorporation and permanence of end-stage patients in research
studies, as reflected by the low number of patients they include. Moreover,
since most studies evaluate subjective endpoints, the potential risk of bias
should be considered when interpreting the results.
Barriers in the implementation of palliative care in
patients with heart failure
Heart failure clinical practice guidelines recommend
considering the addition of PC to patient care. (23,24) However, one third of the patients are bed-ridden at
the time of PC monitoring onset. (25,26) This exposes existing barriers that promote inequity
in the access to PC among HF patients.
For some professionals, PC monitoring together with
the active treatment of the disease involves contradictory actions, as they
consider that PC is exclusively reserved for end stages of the disease, as a
resource when the therapeutic objectives are not met and there are no other
alternatives. (27) This reveals the existing conceptual error at the
population level regarding the palliative term, as well as the limited training
in PC that healthcare professionals have. (28, 29)
On the other hand, several authors agree about the
lack of communication between physicians and HF patients. Only 12% of
professionals annually discuss the prognosis with their patients (30,31) hampering advanced care planning, as the consultation
with the GP in an ambulatory patient constitutes a favorable context to
consider anticipated directives. These directives represent a willful
declaration that the patient makes in full use of his/her mental faculties,
with the aim of their becoming effective when he/she cannot express them. Thus,
it ensures that the future healthcare is carried out according to the patient’s
preferences, guaranteeing the fulfillment of the principle of autonomy and a
better quality of endof-life care. (32,34)
Another important aspect to consider is the difficulty
that presents the detection of the right moment for inclusion in PC monitoring.
It is frequently found that after an acute decompensation,
and following the administration of adequate treatment, the patient can recover
and be discharged. However, the patient does not return to his/her previous
state. These repeated decompensation episodes with
subsequent recovery may cast doubt in the treating physicians, delaying the
inclusion in PC programs. A systematic review evaluating the criteria of
referral to PC revealed that 50% was carried out due to persistent physical
symptoms and mood disorders, 45% for advanced NYHA FC and 37% for frequent
hospitalizations. (35) Several scores have been postulated to approach this
problem, such as the Heart Failure Survival Score (HFSC) and the Seattle Heart
Failure Score (SHFS), (36) as well as the use of the surprise question “would
you be surprised if this patient died next year?”, to identify HF patients near
the end of life and thus promote the consultation with PC. Straw et el.
evidenced a statistically significant association between the answer “not
surprised” and all-cause death at one year (p=0.046).
(37) It is important to emphasize that, unfortunately,
these tools expose the idea of referral to PC in advanced stages of the
disease. Nevertheless, they could be useful for an objective assessment of the
patient’s prognosis, guiding advanced care planning.
Palliative care in heart failures: guidelines and
recommendations
The European Society of Cardiology HF Association has
published several recommendations acknowledging the value of early PC
implementation for the multidisciplinary management of HF. (38) The last edition of the Diagnosis and Treatment
Guideline establishes that HF patients could benefit from the integration of PC
during follow-up, independently of the stage in which they are, even if its
incorporation is posed from the moment of diagnosis and its requirements
increase as the disease progresses and advances. This organizational model
generates a change in the paradigm for the HF patient, categorizing both the
curative and palliative treatments, thus allowing a dynamic and integral care
that leaves behind the original concept of PC focused on end-of-life treatment.
(13) Moreover, it invites healthcare professionals to
apply a palliative approach since the first level of care, detecting the
patients’ needs and enabling the referral to specialized teams for a more
specific management when this is necessary (Figure 2).
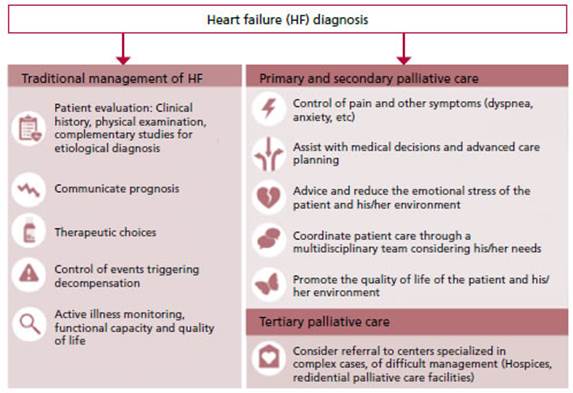
Fig.
2. Integrative care model with the
palliative care, at different levels, in the active treatment of heart failure.
From the early diagnosis of the disease, a continuum is established between the
heart failure specialist with the comfort provided from palliative care
specialist, while therapeutic goals are achieved and future planning is done.
The early implementation PC model has shown to be
beneficial in oncological patients. (15) However, no objective evidence analyzing the impact
of PC onset since diagnosis in HF patients has been found, since most studies
include patients in advanced stages of the disease. Currently, the randomized,
controlled, prospective, open-label, multicenter Early Palliative Care in Heart
Failure Trial is being developed, including 200 HF patients with preserved or
impaired left ventricular ejection fraction in NYHA FC 2. Participants have
been randomly assigned to receive standard care by specialized cardiologists or
by these physicians associated with PC. The primary outcome will evaluate
quality of life at 12 months.
(39) The conclusions of this work could provide the
necessary impulse to overcome the current challenges related with the limited
use of PC and allow a greater application from early stages in patients with
HF.
FINAL REFLECTION
Heart failure is a complex and with increasing
prevalence disease, which causes progressive functional capacity impairment and
elevated associated morbidity and mortality. The existent analogy with
oncological patients when evaluating the high symptom burden and the benefits
demonstrated by PC carried out since the early stages of the disease invite to
consider a paradigmatic change in the care of HF patients.
The progressive implementation of PC since diagnosis
and as part of a multidisciplinary management of HF from the first moment has
the main purpose of detecting and contributing to the specific needs of each
patient, optimizing his/her quality of life, while maintaining an active
treatment of the disease. As it progresses and the therapeutic options are
exhausted, an adequate and fluid communication is essential to establish a plan
of individualized care oriented to the patient and his/her environment
preferences, which guarantees autonomy and tries to avoid futile actions that
only prolong agony and suffering.
Conflicts of interest
None declared.
(See authors’ conflict of interests
forms on the web).
Financing
None.
![]() https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista Argentina de Cardiología
1. Lippi G,
Sanchis-Gomar F. Global epidemiology and future
trends of heart failure. AME Med J 2020;5:15-15.
2. Virani SS, Alonso A, Aparicio HJ,
Benjamin EJ, Bittencourt MS, Callaway C.W, et al. Heart
disease and stroke statistics-2021 update: A report from the American Heart
Association: A report from the American Heart Association. Circulation 2021;143:254-743.
3. Van Deursen
VM, Urso R, Laroche C, Damman K, Dahlström U, Tavazzi L, et al. Co-morbidities
in patients with heart failure: an analysis of the European Heart Failure Pilot
Survey: Co-morbidities in heart failure. Eur J Heart
Fail 2014;16:103-11.
4. Jones
NR, Roalfe AK, Adoki I,
Hobbs FD, Taylor CJ. Survival of patients with chronic heart failure in the
community: a systematic review and meta-analysis. Eur J Heart Fail 2019; 21:1306-25.
5. Roger
VL. Epidemiology of heart failure. Circ
Res 2013;113:646-59.
6. Jaarsma T, Johansson P, Agren S, Strömberg A. Quality of life and symptoms of depression in
advanced heart failure patients and their partners. Curr
Opin Support Palliat Care
2010;4:233-7.
7. Bekelman DB, Rumsfeld JS, Havranek
EP, Yamashita TE, Hutt E, Gottlieb SH, et al. Symptom burden, depression, and
spiritual well-being: a comparison of heart failure and advanced cancer
patients. J Gen Intern Med 2009;24:592-8.
8.
Evangelista LS, Sackett E, Dracup
K. Pain and heart failure: unrecognized and untreated. Eur
J Cardiovasc Nurs. 2019;8:169-73.
9. World
Health Organization. WHO definition of Palliative Care.
2020. https://www.who.int/es/news-room/fact-sheets/detail/palliative-care
10. Allen
LA, Stevenson LW, Grady KL, Goldstein NE, Matlock DD, Arnold RM, et al. Decision
making in advanced heart failure: a scientific statement from the American Heart
Association. Circulation 2012;125:1928-52.
11. Connor
SR, Sepulveda Bermedo MC, Baxter S, Beckwith SK,
Clark D, Cleary J, et al. Global Atlas of Palliative
Care. Second Edition. 2020.
12. Mounsey L, Ferres M, Eastman P.
Palliative care for the patient without cancer. Aust
J Gen Pract 2018;47:765-9.
13. Lynn J,
Admason DM. Living well at the end of life: adapting
health care to serious chronic illness in old age. WHO
Regional Office for Europe 2004.serious chronic illness in old age. WHO
Regional Office for Europe 2004
14. Kavalieratos D, Corbelli J, Zhang
D, Dionne Odom JN, Ernecoff NC, Hanmer
J, et al. Association between palliative care and patient and caregiver
outcomes: A systematic review and meta-analysis. J Am Med Assoc.
2016;316:2104-14.
15. Davis
MP, Temel JS, Balboni T,
Glare P. A review of the trials which examine early integration of outpatient
and home palliative care for patients with serious illnesses. Ann Palliat Med 2015;4:99-121.
16. Herrera Molina E, Rocafort Gil J, Cuervo Pinna MA, Redondo Moralod MJ. Primer nivel asistencial en cuidados
paliativos: evolución del contenido de la cartera de servicios de atención
primaria y criterios de derivación al nivel de soporte. Atencion Primaria. 2016;38:85-92.
17. Von Gunten C.F. Secondary and tertiary palliative care in US
hospitals. J Am Med Assoc 2002;287:875-81.
18.
International Association for Hospice and Palliative Care, Worldwide Palliative
Care Alliance: Joint declaration and statement of commitment on palliative care
and pain treatment as human rights. J Pain Palliat
Care Pharmacother 2008;22:300-2
19. Brännström M, Boman K. Effects of
person-centred and integrated chronic heart failure
and palliative home care. PREFER: a randomized controlled study: PREFER: a
randomized controlled study. Eur J Heart Fail
2014;16:1142-51.
20. Wong
FK, Ng AY, Lee PH, Lam PT, Ng JS, Ng NH, et al. Effects of a transitional
palliative care model on patients with end-stage heart failure: a randomised controlled trial. Heart (British Cardiac
Society). 2016;102:1100-8.
21. Rogers
JG, Patel CB, Mentz RJ, Granger BB, Steinhauser KE, Fiuzat M, et al. Palliative
care in heart failure. J Am Coll Cardiol
2017;70:331-41.
22. Sahlollbey N, Lee C.K.s, Shirin
A, Joseph P. The impact of palliative care on clinical and patient-centred outcomes in patients with advanced heart failure: a
systematic review of randomized controlled trials. Eur
J Heart Fail 2020;22:2340-6.
23. McDonagh TA, Metra M, Adamo M,
Gardner RS, Baumbach A, Böhm
M, et al. ESC Guidelines for the diagnosis and treatment of acute and chronic
heart failure. Eur Heart J. 2021;42:3599-726.
24. Yancy CW, Jessup M, Bozkurt B,
Butler J, Casey D Jr, Drazner
MH, et al. ACCF/AHA guideline for the management of heart failure: a report of
the American College of Cardiology Foundation/American Heart Association Task
Force on Practice Guidelines. J Am Coll Cardiol. 2013;62:147-239.
25. Warraich HJ, Wolf SP, Mentz RJ,
Rogers JG, Samsa G, Kamal AH. Characteristics and
trends among patients with cardiovascular disease referred to Palliative Care.
JAMA Network Open. 2019;2:192-375.
26. Bakitas M, MacMartin M, Trzepkowski K, Robert A, Jackson L, Brown J.R, et al. Palliative
care consultations for heart failure patients: How many, when, and why? J Cardiac Fail. 2013;19:193-201
27. Kavalieratos D, Mitchell EM, Carey TS, Dev
S, Biddle AK, Reeve BB, et al. Not the ‘grim reaper service’”: an assessment of
provider knowledge, attitudes, and perceptions regarding palliative care referral
barriers in heart failure. J Am Heart Assoc 2014;3, e000544.
28.
Zimmermann C, Wong JL, Swami N, Pope A, Cheng Y, Mathews J, et al. Public
knowledge and attitudes concerning palliative care. BMJ Support Palliat Care. 2021;0:1-11
29. Pieters J, Dolmans DH, Verstegen
DM, Warmenhoven FC, Courtens
AM, Van den Beuken Van Everdingen
MH. Palliative care education in the undergraduate medical curricula: students’
views on the importance of, their confidence in, and knowledge of palliative
care. BMC Support Palliat Care 2019;18:72.
30. Dunlay SM, Foxen JL, Cole T,
Feely MA, Loth AR, Strand JJ, et al . A survey of clinician attitudes and
self-reported practices regarding end-of-life care in heart failure. Palliat Med 2015;29:260-7.
31. Schallmo MK, Dudley Brown S, Davidson PM. Healthcare
providers’ perceived communication barriers to offering palliative care to
patients with heart failure: An integrative review: An integrative review. J Cardiovasc Nurs 2019;34:9-18.
32. Seymour
J, Gott M, Bellamy G, Ahmedzai
SH, Clark D. Planning for the end of life. Soc Sci Med.2005;59:57-68.
33. Belli LF. El debate en torno a
la validez de las directivas anticipadas en salud. Persona y Bioetica 2014;18:213-25.
34. Chen
JL, Sosnov J, Lessard D,
Goldberg RJ. Impact of do-not-resuscitation orders on quality of care
performance measures in patients hospitalized with acute heart failure. Am
Heart J. 2008;156:78-84.
35. Chang
YK, Kaplan H, Geng Y, Mo L, Philip J, Collins A, et al.
Referral criteria to palliative care for patients with heart failure: A
systematic review: A systematic review. Circulation. Heart Fail.
2020;13:e006881
36. Goda A, Williams P, Mancini D, Lund LH. Selecting patients
for heart transplantation: comparison of the Heart Failure Survival Score
(HFSS) and the Seattle heart failure model (SHFM). J Heart Lung Transplant 2011;30:1236-43.
37. Straw
S, Byrom R, Gierula J,
Paton MF, Koshy A, Cubbon
R, et al. Predicting one-year mortality in heart failure using the “Surprise
Question”: a prospective pilot study. Eur J Heart Fail 2019; 21:227-34.
38. Hill L,
Prager Geller T, Baruah R,
Beattie JM, Boyne J, De Stoutz N, et al. Integration
of a palliative approach into heart failure care: a European Society of Cardiology
Heart Failure Association position paper. Eur J Heart
Fail. 2020;22:2327-39.
39. Becher MU, Balata M, Hesse M, Draht F, Zachoval C, Weltermann B, et al. Rationale and design of the EPCHF
trial: the early palliative care in heart failure trial (EPCHF). Clin Res Cardiol 2021;9;1-9