
INTRODUCTION
Bicuspid aortic valve (BAV) is the most common congenital heart defect, affecting 0.5 - 2% of the population, with a higher incidence in males. (1,2) This congenital heart defect represents a valvuloaortopathy with family aggregation. (3) Because of its high prevalence, most cardiologists must deal with BAV patients during their medical practice. The lifetime risk of major cardiovascular complications is high, mainly severe aortic stenosis and regurgitation, infective endocarditis, and aortic aneurysm. (4-9) This condition can be diagnosed at any stage of life, from newborns to the elderly, and in the context of different clinical circumstances. (10-12)
In our setting, multimodality imaging is not readily accessible to the general population. There are no current national echocardiographic screening programs for the detection of BAV that allow for the evaluation of index cases and their first- degree relatives, and for periodic follow- up. In most cases, the diagnosis is incidental or is made when complications occur. The extent to which healthcare professionals request or have access to these methods while monitoring patients with BAV, (13) as well as the degree to which they adhere to guidelines for the management of these patients in our setting, remains unknown. Furthermore, we are unaware of the potential for significant heterogeneity in BAV management between institutions. The decision to recommend surgical treatment before complications arise increases the life expectancy of patients with BAV. Therefore, it is imperative to investigate these aspects and understand the diagnostic process, current management, and decision- making in our setting. So far, there is no information on the management of BAV in our country.
Decision-making for these patients has become a more complex process due to the development of new technologies and treatments. This often involves the participation of various disciplines to achieve patientcentered care. (14) The availability of a multidisciplinary Heart Team to make decisions in complex cases about the type of intervention and selection of valve replacement in young patients is an important aspect for managing the condition. In patients with BAV, the Heart Team should involve members of the Aortic Team, as both conditions often coexist. This team should include cardiovascular surgeons, cardiologists (interventional and non- interventional), specialists in cardiovascular imaging, and cardiovascular anesthesiologists. Additionally, cardiologists or referral centers who have had the opportunity to get to know the patients for a longer period should be involved in the decision- making process during these regular team meetings. (15)
OBJECTIVES
The "Dr. Oscar Orías" Council on Doppler Echocardiography and Vascular Ultrasound, and the Research Area of the Argentine Society of Cardiology designed a voluntary and anonymous online survey for cardiologists in Argentina. The primary objective was to determine the characteristics of the diagnosis and current management of BAV at the national level. The secondary objective was to identify regional differences in the diagnosis and management of BAV, as well as access to more complex diagnostic and surgical techniques.
METHODS
A total of 240 cardiologists in Argentina who were treating patients with BAV anonymously and voluntarily completed the survey between May 2024 and January 2025.
The survey was distributed via a link in e- mails sent to the mailing list of the Argentine Society of Cardiology and through the social media accounts of the Argentine Society of Cardiology and the Council of Doppler Echocardiography and Vascular Ultrasound. Data were anonymously collected on the REDCap platform. The questions were divided into three sections: demographic characteristics and medical practice, diagnosis of BAV, and management and follow- up. A Likert scale was used to rate opinion and agreement/dissagement responses.
Statistical analysis
Continuous variables were expressed as mean and standard deviation, or median and interquartile range (IQR), according to their distribution. Categorical variables are presented as absolute frequencies (n) and percentages. Continuous variables were compared using the two- tailed Student's t test in case of means or the Wilcoxon in case of medians. Categorical variables were compared using the chi- square test with Yates correction or the Fisher's exact test, as appropriate. Logistic regression analysis was performed to evaluate the association between categorical variables. The results were expressed as odds ratio (OR) and its corresponding 95% confidence interval (CI). All the statistical calculations were performed with R using SOFA Stats software package under Windows operating system. A p value < 0.05 was considered statistically significant.
RESULTS
Table 1 summarizes the main characteristics of the 240 professionals surveyed and the institutions where they worked. Sixty-five percent (n = 156) of respondents were men; mean age was 48.1 ± 12.2 years, and 45.2% (n = 108) worked in tertiary care institutions. Most respondents (37.4%; n = 86) were from Buenos Aires Metropolitan Area (AMBA), 27.4% (n = 63) from the province of Buenos Aires, and 5.7% (n = 13) from Cordoba.
Table 1.
Main characteristics of respondents and places of medical practice
| Variable | n = 240 |
|---|---|
| Male sex | 156 (65%) |
| Age | 48.1 ± 12.2 |
| Clinical cardiology | 114 (47.5%) |
| Cardiovascular imaging | 109 (45.4%) |
| Years of practice | |
| 1-10 | 75 (31.5%) |
| 11-20 | 74 (31.1%) |
| > 20 | 89 (37.4%) |
| Institutional complexity | |
| Tertiary care | 108 (45.2%) |
| Secondary care | 55 (23.0%) |
| Outpatient clinic | 29 (12.1%) |
| Office | 47 (19.7%) |
| Funding | |
| Public hospital | 60 (25.4%) |
| Prepaid medical insurance | 79 (33.5%) |
| Social security | 90 (38.1%) |
| Any of the following available: | |
| Doppler echocardiography | 228 (95%) |
| Multimodality imaging | 144 (60.3%) |
| Heart Team | 120 (50%) |
| How many patients with BAV do you follow-up and manage? | |
| < 10 | 134 (56.5%) |
| Between 10 and 99 | 97 (40.9%) |
| Between 100 and 299 | 3 (1.3%) |
| > 300 | 3 (1.3%) |
BAV: bicuspid aortic valve
Ninety-five percent (n = 228) had access to Doppler echocardiography and 60.3 percent (n = 144) to multimodality imaging at their centers. This was more common among professionals working in tertiary care centers (84.1% vs. 40.9%; OR 7.6, 95% CI 4.1-14.2; p < 0.001 ), with no significant differences according to the geographical location of their medical practice.
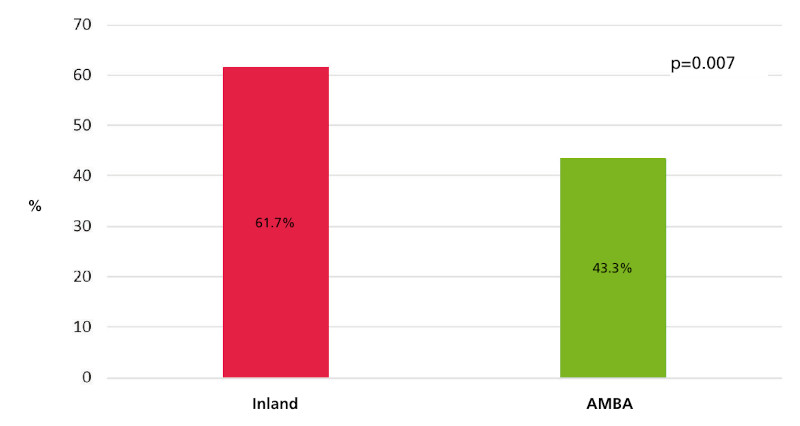
Fifty percent (n = 120) of respondents lacked a Heart Team for complex decision- making at their institution. This was more common in inland centers (61.7% vs. 43.3%; OR 2.1, 95% CI 1.2- 3.6; p = 0.007) with no significant differences between public and private institutions (Figure 1). As expected, access to a Heart Team was more frequent among professionals working in tertiary care centers (71.2% vs. 32.5%; OR 5.1, 95% CI 2.9-8.9; p < 0.001 ).
Fig. 1.
Availability of Heart Teams for complex decision- making according to the place of medical practice (AMBA vs. inland).
According to 85.4% (n = 204) of respondents, patients are usually diagnosed in adulthood. When asked about echocardiographic screening in first- degree relatives, 60.4% (n = 145) of respondents indicated that they always request it, while 10% (n = 24) never do so (Figure 2). Among those who responded affirmatively, the proportion of specialists in cardiovascular imaging was higher (46.9% vs. 12.5%; OR 6.7, 95% CI 1.9- 23.2; p = 0.001 ).
Fig. 2.
Proportion of professionals who request echocardiographic screening and evaluation of the aorta at the time of the diagnosis of bicuspid aortic valve
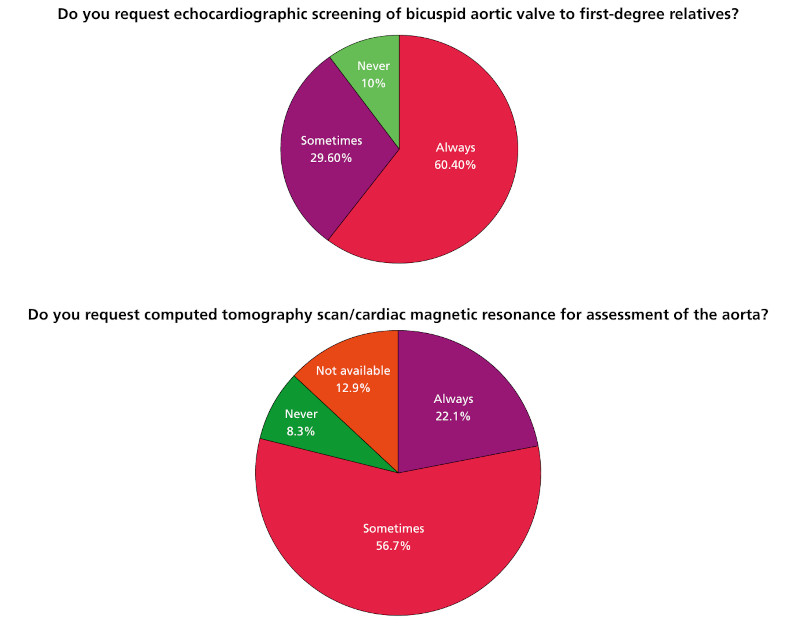
Computed tomography or magnetic resonance imaging was never requested at the time of diagnosis of BAV by 8.3% (n = 20) of respondents, 12.9% (n = 31) reported that these methods were not available, and 71.3% (n = 171) of professionals requested computed tomography (CT) or magnetic resonance imaging (MRI) scans in less than 40% of patients with BAV during follow-up
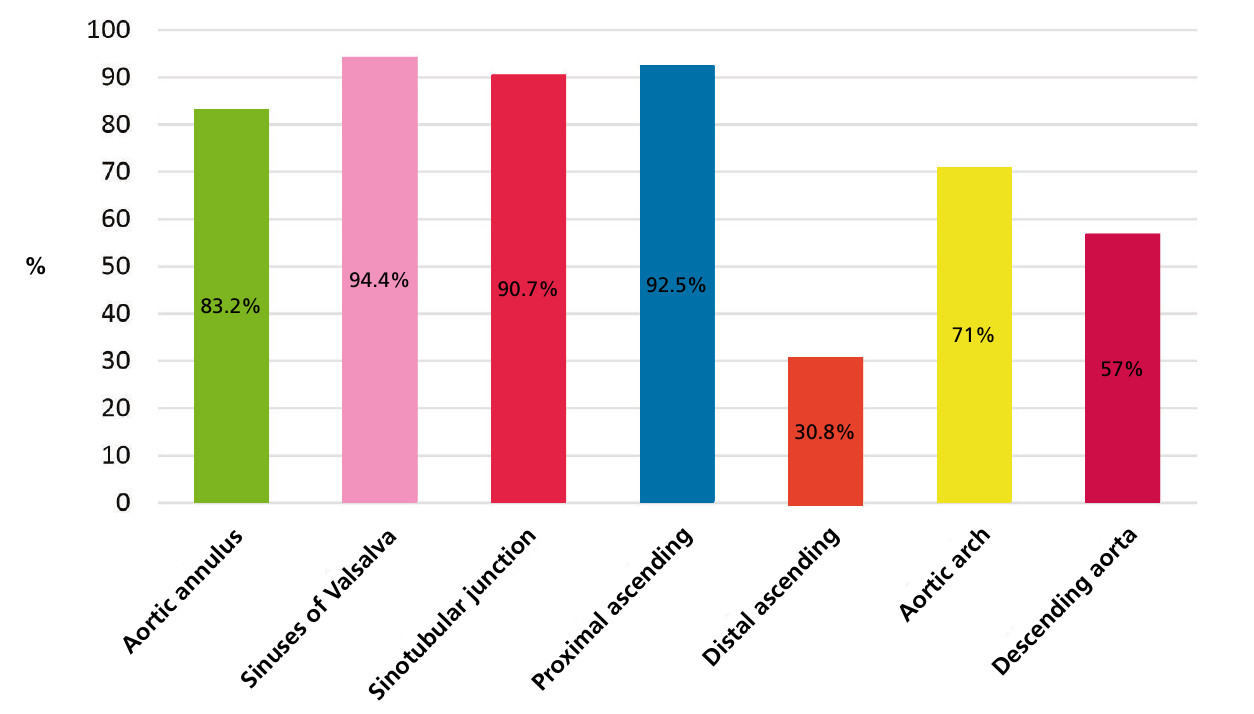
Figure 3 shows that only 30.8% of the professionals surveyed measure the distal ascending aorta, a common site of aortic dilatation in patients with BAV.
Fig. 3.
More than 80% of the professionals surveyed reported that they measure the aortic annulus, sinuses of Valsalva, sinotubular junction, and proximal ascending aorta. Only 30.8% reported measuring the aorta in its distal tubular portion
Regarding the type of intervention, 65.7% (n = 144) have never indicated the Ross procedure to any patient, 65.4% (n = 157) have not indicated aortic valve replacement to any patient. However, 40.7% (n = 95) have recommended transcatheter aortic valve implantation (TAVI) to some patients with VAB.
Regarding the intervention of patients with indication for surgery, 12.9% (n = 31) reported that patients received delayed surgical treatment due to prolonged waiting times, with some deaths occurring while on the waiting list. This was more common among professionals working in public institutions (26.6% vs. 8.3%; OR 4, 95% CI 1.8- 8.6; p < 0.001 ). In addition, 40.8% (n = 98) responded that they refer patients to centers with advanced expertise in the appropriate technique for each case (the Ross procedure, the Bentall-De Bono technique or aortic valve repair).
When asked about the number of patients they had managed with aortic dissection and BAV over the past 5 years, 91.3% (n = 219) of the professionals responded that they had managed between 0 and 5 patients. Most respondents (57.1% n = 137) reported not restricting competitive sports activity due to the risk of aortic dissection.
Only 16.7% of respondents (n = 40) reported consulting the Heart Team for all complex patients with indications for intervention to discuss the best therapeutic decision. Meanwhile, 39.6% of respondents (n = 95 ) reported discussing only some of their patients with indications for intervention with the Heart Team.
Prophylaxis for infective endocarditis is prescribed to all patients with BAV by 41.4% (n = 99) of professionals, only in cases of high risk of endocarditis in 41.4% (n = 99) according to current guidelines, and 14.2% (n = 34) responded that they only indicated prophylaxis in patients with BAV and aortic valve dysfunction.
Regarding genetic counseling, 40.8% (n = 98) responded that they never request it in patients with BAV, and 47.1% n = 113 responded that they only do so in cases of familial BAV.
DISCUSSION
This anonymous and voluntary survey, completed by 240 Argentine cardiologists, provides insight into the characteristics of the diagnosis and current management of BAV in our country. The findings reveal several important aspects that require detailed analysis in the context of international literature and clinical practice guidelines.
Detection and family screening
One of the main findings is the confirmation that, in Argentine clinical practice, the diagnosis of BAV is usually made in adulthood, a fact reported by 85.4% of the surveyed professionals. This finding highlights the lack of systematic population-based or family echocardiographic screening programs in our setting. This is different from the recommendation for early detection in first-degree relatives due to the family aggregation of BAV. (3) While a considerable proportion of respondents (60%) reported requesting screening for family members, 10% never did so. The request was significantly higher among professionals specializing in cardiovascular imaging, which could suggest a bias due to the subspecialty practiced. This heterogeneity in medical practice underscores the necessity for enhanced dissemination of recommendations and the implementation of strategies to facilitate family screening.
Although international guidelines recommend echocardiographic screening of first-degree relatives of patients with BAV, adherence to this recommendation is unknown. A recent meta-analysis included 2297 patients (32 ± 21 years, 71% men) with BAV and 6054 screened relatives (29 ± 13 years, 50.6% men). The prevalence of BAV among first- degree relatives was 7.3% (95% CI 6.1% - 8.6% p < 0.001) and 9.4% for aortic dilatation. (15) Family members with BAV were about 6 times more likely to have aortic dilatation than family members with tricuspid aortic valves. The existence of aortic dilatation without BAV could be due to limitations of echocardiography to identify partial raphe. The indication for echocardiographic screening is based on a significantly higher prevalence of positive findings in relatives than in the general population. Given that echocardiography is a safe and relatively low- cost test in our country, implementing echocardiographic screening seems feasible and useful. However, the optimal age for recommendation remains unclear, whether it should be for pediatric or adult patients, and whether performing it at an early age is beneficial (given the anxiety surrounding the diagnosis and the potential complications in adulthood). Additionally, there is a need to determine whether a transthoracic echocardiogram is sufficient, considering the prevalence of false negative results.
Access to advanced diagnostic and therapeutic resources
Access to multimodality imaging assessment during follow- up of patients with BAV remains limited in our country. Although 60.3% of professionals work in centers with these techniques, they are significantly more available in tertiary care institutions. A considerable percentage of professionals (21.2%) , including those working in centers lacking these techniques and those who never request them, do not have access to these tools at the time of diagnosis. The majority of these professionals request these tests for less than 40% of their patients under follow-up. This situation could lead to underdiagnosis of aortic dilation and affect adequate risk stratification and timely planning of interventions, considering the high prevalence of aortic complications in this population. (4-6)
Only half of the surveyed cardiologists reported Heart Teams available at their institutions. A lack of Heart Teams was more common among inland professionals. These results are consistent with those of a Canadian study that reported that 47.6% of the high-complexity centers surveyed lacked Heart Teams. (16) In that study, centers with Heart Teams highlighted that their main benefits were collaborative decisionmaking with shared responsibility and transparency, improvement in communication among professionals, improvements in patient care and outcomes, and inter professional learning for new approaches and technologies. The lower availability of Heart Teams in lower complexity centers could influence the homogeneity of management and access to optimal therapeutic strategies for complex cases. Although the guidelines for the management of patients with valvular heart disease recommend Heart Team assessment (Class I recommendation, level of evidence C), the assigned level of evidence demonstrates a lack of supporting data, as it is derived from expert consensus and/or small studies, retrospective series, or registries. (17,18)
Therapeutic and Intervention Strategies
When analyzing intervention strategies, the Ross procedure and aortic valve repair were indicated less frequently than conventional aortic valve replacement, and 34.3% and 34.6% of survey respondents did not indicate the Ross procedure and aortic valve repair, respectively, for any patient. Notably, a significant percentage of professionals (40.7%) indicated TAVI for some patients with BAV. This could reflect an increasing trend in the use of TAVI, despite limited evidence and unfavorable outcomes in this valve phenotype compared to degenerative aortic stenosis. This is a special concern given the still- undefined long- term role of TAVI in younger patients. (19,20)
A worrying finding was that 13% of respondents reported that patients with indication for surgery experience delayed treatment due to long waiting times, with cases of death while on the waiting list, particularly in public institutions. This situation highlights the barriers to timely treatment and underscores the need to optimize resources and waiting list management.
Low adherence to current guidelines on prophylaxis of infective endocarditis is also worth noting. Despite the recommendation to limit prophylaxis to high- risk patients, many professionals continue to prescribe it for all patients with BAV or in the presence of valve dysfunction. According to the current recommendations of the American Heart Association and the Argentine Society of Cardiology, BAV is no longer an indication for antibiotic prophylaxis, as it is a condition with a moderate risk of morbidity and mortality related to endocarditis. (19,20) However, adherence to these guidelines is low, and the incidence of endocarditis has been detected to increase since their publication. It is recommended that patients be informed that BAV is no longer an indication for antibiotic prophylaxis; yet, the decision to stop indicating it is complex.
Finally, genetic counseling for patients with BAV is not a systematic practice in our country. Most professionals only request genetic counseling for familial cases of BAV. There is still a lack of information on the usefulness of genetic testing in this scenario, although the identification of mutations associated with familial forms has been increasing in recent years. The limited availability of current panels for patients with BAV may contribute to the underutilization of genetic testing, which could hinder the early identification of other affected family members and the implementation of proactive follow- up strategies.
Study limitations
Our study has some limitations. As this was a voluntary online survey, there is a possibility of selection bias, as more cardiologists with a greater interest in the topic of BAV could have participated. Furthermore, the responses are based on the self- perception of the professionals, which may not fully reflect actual clinical practice. Although the sample size was significant, it may not fully represent the heterogeneity of cardiology practice nationwide.
Clinical implications and future lines of research
The findings of this study have significant implications for clinical practice in Argentina, underscoring the need to implement of echocardiographic familial screening strategies and improve access to multimodality imaging techniques. It is also necessary to encourage the creation and functioning of multidisciplinary Heart Teams, optimize waiting times for surgery, and promote greater adherence to updated clinical guidelines, especially with regard to the prophylaxis of infective endocarditis.
Future lines of research could focus on prospective studies evaluating the impact of different management strategies on the clinical outcomes of patients with BAV in Argentina. It would be worthwhile to investigate why aortic valve replacement and the Ross procedure are underused, and to examine the role and long- term outcomes of TAVI in this population. Similarly, developing strategies to improve access to genetic evaluations and family counseling could significantly impact the early detection and comprehensive management of BAV in our country.
CONCLUSION
This pioneer national study provides a valuable snapshot of the diagnosis and management of BAV in Argentina. The findings reveal an opportunity to improve medical practice, including implementation of early detection strategies, optimization of access to advanced imaging tests, multidisciplinary decisionmaking, and greater adherence to international clinical guidelines. It is imperative for the Argentine cardiology community to acknowledge these findings and collaborate to enhance the comprehensive management of BAV patients in our country.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors. Conflicts of interest
Conflicts of interes
None declared. (See authors' conflict of interests forms on the web).
Acknowledgments
We are grateful to all the professionals who voluntarily agreed to participate in the survey.