Acute heart failure (AHF) is one of the leading causes of hospitalization in people over 65 years of age worldwide, with an in-hospital mortality rate of up to 7%. Despite notable advances in pharmacological and device-based management, optimizing diuretic treatment remains one of the most complex and least standardized clinical aspects. (1-3)
For decades, the evaluation of diuretic response has been based on indirect parameters such as body weight, total diuresis, water balance, and clinical assessment of congestion. However, these indicators have low sensitivity and specificity, especially in patients with advanced HF, refractory congestion, or impaired renal function. (1-3) In this context, urinary sodium measurement emerges as a tool both for assessing diuretic efficiency (4-11) and for guiding decongestive treatment. (12-16)
The recent position paper "Urinary sodium analysis: The key to effective diuretic titration?", published by Meekers et al. in the European Journal of Heart Failure, (17) presents a detailed and critical review of the renal mechanisms involved in water and salt retention in patients with AHF, therapeutic options in cases of diuretic resistance (DR), and the role of urinary sodium in monitoring and therapeutic guidance in these patients.
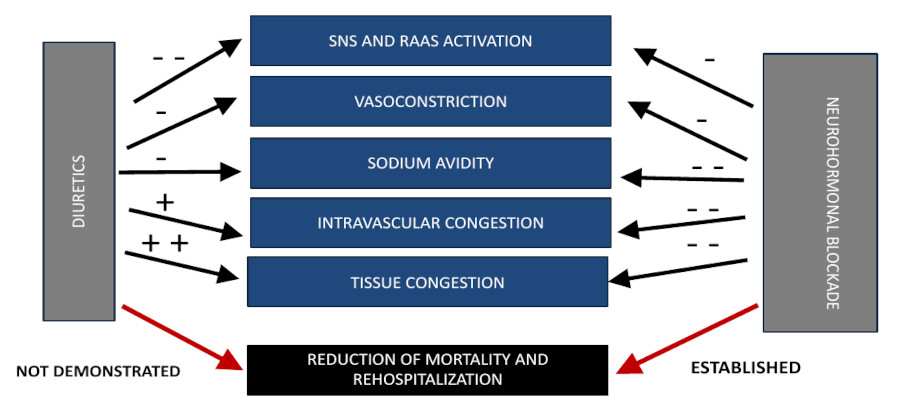
Patients with significant neurohormonal activation, chronic or acute renal impairment due to congestion and reduced renal perfusion, as well as those with hypoalbuminemia and chronic use of furosemide, experience greater water and salt retention and less effective diuretic treatment. (15,16) This condition, known as DR, can occur in up to 40% of cases of AHF and undoubtedly constitutes a therapeutic challenge. In these patients, a combination of diuretics to block sodium reabsorption in different sectors of the nephron could be beneficial, requiring careful and individualized evaluation of congestion and diuretic response. (15,16) It is then when multiparametric assessment of congestion and measurement of diuretic efficacy expressed by natriuresis become essential.
The document provides a review of the main studies that demonstrated benefits in terms of decongestion from the combination of diuretics in patients with DR.
The ADVOR (intravenous acetazolamide 500 mg/ day vs. placebo) and CLOROTIC (hydrochlorothiazide 25-100 mg/day adjusted for renal function vs. placebo) studies have shown that adding these drugs to intravenous furosemide in patients with DR is associated with increased diuresis, natriuresis, weight loss, and successful clinical decongestion, with no impact on mortality or readmissions for HF, and with increased risk of worsening renal function and hypokalemia with hydrochlorothiazide. (18,19)
Mineralocorticoid receptor antagonists could be useful in patients with acute HF and DR, as demonstrated by the ATHENA study, (20) although they have a slower onset of action and are therefore probably not useful in patients who require aggressive and rapid decongestion due to the clinical severity of their condition. The possibility of using gliflozins in patients with acute HF is also noteworthy, as they have demonstrated an adequate safety and efficacy profile in various studies, (21-24) although their diuretic action also begins at approximately 48 hours. (25) Although dapagliflozin was not superior to metazolone in patients with AHF and DR in the DAPA-RESIST study, (26) it should be noted that gliflozins provide additional modest diuresis and have long-term cardio- and nephroprotective effects. (27) It is possible that both drugs, antialdosterone agents and gliflozins, will be reserved for patients with AHF and DR with a certain degree of compensation or possibly close to discharge.
Given the complexity of decongestive treatment, urinary sodium measurement emerges as a direct, quantifiable, and dynamic tool for assessing the actual natriuretic effect of intravenous diuretics, allowing for objective evaluation of the therapeutic response in the first hours after administration. In addition, there is significant evidence supporting the association between natriuresis in patients with AHF and in-hospital evolution and outpatient follow-up at 6 months after the event. (4-11)
The use of urinary sodium in spot samples, generally 2 hours after diuretic administration, is an early marker of response and may allow for more agile and personalized treatment titration, thus reducing clinical variability in congestion management, medical inertia, and risk of failure during decongestion. (15,16) Diuretic titration is recommended if the urinary sodium concentration is <70 mmol/L, bearing in mind that other cut-off points such as 50 meq/L are less sensitive in detecting patients with DR, and of course taking into account a urinary volume of less than 100-150 mL/h. (17) In a recently published study in Argentina, a single measurement of natriuresis 2 hours after a 40 mg intravenous bolus of furosemide upon hospital admission, with a cutoff point of 70 meq/L, was associated with worse in-hospital outcomes (DR, persistent congestion, use of more aggressive decongestion therapies and inotropes, and cardiovascular death). (11)
Finally, Meekers et al. present a possible algorithm for the therapeutic management of diuretics based on urinary sodium in patients with acute HF and DR, which attempts to summarize the evidence on the benefits of using tubular blockade and of three important studies that demonstrated significant improvements in natriuresis and diuresis when following therapeutic guidelines based on urinary sodium (ENACT-HF, PUSH-AHF, and EASY-HF). (28-30)
This is a pragmatic algorithm for managing diuretic therapy and assessing congestion, with fewer urinary sodium measurements but a more aggressive and early approach to tubular blockade than other previously proposed algorithms. (15,16) Although this would possibly reduce hospital stay and achieve greater success in decongestion, it necessarily implies closer control of blood volume status, tissue congestion, and the possible adverse effects of these drugs. In addition, the greater benefit of combining acetazolamide with thiazides is emphasized due to its better renal safety profile, as evidenced in the ADVOR and CLOROTIC trials, (18,19) although the choice must undoubtedly be personalized based on renal function and electrolyte and acid-base imbalances.
It is important to recognize that the available evidence, while promising, still lacks randomized clinical trials demonstrating a direct impact of this strategy on hard clinical outcomes such as mortality or readmissions. Furthermore, the usefulness of measuring natriuresis after 24-48 hours has not yet been demonstrated, so this strategy would be limited to the first day of hospitalization. Finally, serial measurement of natriuresis as a routine tool presents logistical and educational challenges, especially in centers with limited resources or no experience with standardized monitoring protocols. Therefore an institutional strategy including interdisciplinary training and adaptation of laboratory systems is required. to enable rapid and reliable analyses
Clinical trials are underway to evaluate the influence of dietary sodium and fluid intake on urinary sodium concentration and the role of urinary sodium concentration in later stages of decongestion.
In conclusion, Meekers et al.’s work reevaluates an underutilized tool in clinical practice that will potentially transform the management of congestion in patients with acute HF. We are facing a potential paradigm change, in which basic physiology returns to the center of clinical decision-making. The challenge now is to validate this strategy in prospective studies and facilitate its adoption in a safe and cost-effective manner. The remaining question is when and how to systematically integrate natriuresis measurement into our therapeutic algorithms.
Conflicts of interest
None declared.
(See authors' conflict of interests forms on the web/Additional material).