
INTRODUCTION
Spontaneous coronary artery dissection (SCAD) is a trigger for acute myocardial infarction (AMI), mainly in young or perimenopausal women with few or no risk factors for cardiovascular disease, and it accounts for up to onethird of AMIs in this population. (1,2) SCAD is caused by bleeding from the vasa vasorum or a tear in the intima, which creates a false lumen that occludes the true lumen, compromising distal blood flow. Diagnosis is complex, requires experience and a high clinical index of suspicion, and is key to guiding definitive management. (3–6)
The information available up to 2022 was based on case reports, retrospective series, and position statements from developed countries; however, on that year the first multicenter SCAD registry with longterm followup was published, enabling the characterization of many poorly understood aspects of the disease. (4,7)
Objectives
There is no document or consensus statement based on realworld data from Latin America regarding the incidence and course of SCAD. This highlights the need to address the issue, conduct an indepth review of the literature, and generate findings that can explain the behavior of the disease, which has never been characterized in our region. This is the aim of the present review.
METHODS
A systematic review of the literature was conducted by selecting the most important studies related to this condition. The search was performed in PubMed, SciELO, and Google Scholar using the keywords “Spontaneous coronary artery dissection,” “SCAD,” “Disección coronaria espontánea,” and “Disección coronaria espontánea y displasia fibromuscular.” Given the complexity of the disease and the scarcity of largescale studies, we selected the largest registries, reviews, and the most comprehensive case reports in English and Spanish published over the past 20 years.
RESULTS
Definition, history, and epidemiology of the disease
SCAD is defined as the acute separation of the epicardial coronary arteries’ layers, unrelated to trauma, iatrogenic causes, or atherosclerotic disease. (1,2) The first description was provided by Pretty in 1931 during the autopsy of a 42-yearold woman who had died of sudden death. A link was therefore established between SCAD, ischemic heart disease, and sudden death in young women. (3)
SCAD has emerged as an increasingly common cause of acute coronary syndrome (ACS) and sudden death, including cases related to ventricular arrhythmias in young or middleaged patients without a high burden of atherosclerotic disease. (1–3)
It has been nearly a century since the first description of findings related to the disease. However, it is in the last decade that more knowledge has been generated, due to a greater number of publications and position statements from various scientific societies aimed at developing better clinical and therapeutic approaches. (4-6) In 2022, Saw et al. published the first multicenter SCAD registry in Canada, involving 750 adult patients followed over a 4-year period, characterizing poorly understood aspects of the disease, such as those related with treatment, recurrence, and mortality. (4)
SCAD affects both sexes throughout their lives; it is more common in Caucasian individuals and women, with a peak incidence between 45 and 53 years of age. (1,3,6) It accounts for 0.07% to 0.2% of all coronary angiographies performed for any reason and 2% to 4% in the context of an ACS. (7,8) Its prevalence is 1.7% to 4% of all ACS cases. When considering gender and age, Canadian, French, Spanish, and New Zealand registries show that SCAD accounts for 24% to 36% of ACS cases in perimenopausal women. (4,8,9,10)
Regarding AMI during pregnancy, it is known to occur on average in 1 out of every 16 000 pregnancies, and SCAD accounts for up to 50% of these events, particularly in the postpartum period. (11)
There is no established monogenic cause, so there are no recommendations for conducting family genetic screening following a SCAD episode. However, due to the direct link with fibromuscular dysplasia (FMD), it is considered good practice to screen for SCAD firstdegree relatives with FMD. (3)
The prevalence in men is very low, and it appears that the disease has no emotional trigger and is not related to FMD, but rather to physical stress, as the few reports are based on extreme sports and young soldiers. (3,12)
Oneyear mortality is 2%, and at 3 years it is estimated to be close to 1%, with a 3-year recurrence rate of AMI of approximately 18%. (1,13)
Pathophysiology and etiopathogenesis
There are two pathophysiological theories that converge on a similar point: the formation of a hematoma that compresses the true lumen and causes myocardial ischemia. The first is the spontaneous appearance of an intimal dissection flap (“outsidein” theory), and the second is hemorrhage within the media or the vasa vasorum (“insideout” theory), in which there is no endothelial rupture. The latter theory has received greater clinical validation and support from optical coherence tomography (OCT). (14)
Pathological findings reveal periadventitial inflammatory infiltration, in contrast to what occurs in collagen diseases, where the adventitia is spared and there is necrosis of the arterial media. (3)
The etiology of the disease is multifactorial. Genetic, hormonal, hereditary, and acquired factors, as well as systemic diseases are involved, which in the presence of precipitating factors appear to promote SCAD development.
Some possible associations are discussed below. (3,14)
a) Fibromuscular dysplasia (FMD): This is an arterial disease strongly associated with SCAD. Some reports associate them in 11–86% of all cases, depending on the diagnostic method used. In the French DISCO registry—the largest European multicenter cohort to date—373 patients were enrolled, and the coexistence of SCAD and FMD was documented in 45% of all included patients. Furthermore, the association between SCAD and noncoronary arterial involvement due to FMD is commonly reported in the literature, renal and carotid arteries being the most frequently affected. (9)
FMD causes involvement of the arterial walls through a nonatherosclerotic and noninflammatory mechanism similar to SCAD, primarily affecting women in their fifties with few cardiovascular risk factors. (3,6)
The main characteristic of the affected vessels is concentric or tubular narrowing. The disease can be unifocal or multifocal, and unilateral or bilateral. The most common and severe form of presentation is the multifocal type, which is characterized by areas of stenosis and dilation or a beaded pattern. Complications range between stenosis, dissection and arterial aneurysms affecting the cervical, renal, and visceral arteries. (3,6)
b) Female gender, pregnancy, and menopause: The prevalence of the disease in women, between the end the fourth decade of life and the beginning of the fifth, supports the hormonal hypothesis. (3)
Canadian studies report a prevalence of pregnancyassociated SCAD of approximately 1.81 cases per 100 000 people. Peripartum involvement accounts for 10% to 15% of all SCAD cases with an apparent poorer prognosis, since it presents as ST-segment elevation ACS with greater involvement of the left main coronary artery or proximal multivessel disease, which is associated with more extensive infarcts and a greater degree of ventricular dysfunction. (4,11) Pregnant women with SCAD are typically multiparous and older at the time of delivery; however, there are some case reports of SCAD occurring years after delivery. (3,14) It is hypothesized that hormonal changes in coronary estrogen and progestogen receptors alter vascular architecture and induce conformational changes that predispose to SCAD. (13)
Among the triggering factors, the first pregnancy appears to be a trigger for the development of the disease in subsequent pregnancies. Other factors reported with a weaker association include preeclampsia, advanced maternal age, Black race, hypertension, dyslipidemia, depression, the Valsalva maneuver, nausea, and migraine. (11,13)
c) Inflammatory conditions: There are few associations with specific inflammatory diseases due to vasculitis per se. (13)
d) Inheritance and genetics: A mutation in the genes encoding the formation of the extracellular matrix of fibrillar collagen predisposes individuals to weakness of the arterial walls. (15,16) SCAD has been linked to more than 7 genes. Some related syndromes include Ehlers-Danlos (COL3A1 mutation), Marfan (FBN1 mutation), and Loeys-Dietz (TGFBR1, TGFBR2, and TGFBR3 transforming growth factor mutations). The DISCO registry found a direct association with the locus for DFM, known as PHACTR 1. (9)
Diagnosis
The characteristic presentation of SCAD is AMI in a woman with few or no cardiovascular risk factors. Chest pain is the initial symptom (85–96% of cases), with typical radiation and accompanied by dyspnea, diaphoresis, elevated biomarkers, and even abnormalities in left ventricular motility and ejection fraction. At first glance, therefore, the clinical picture is indistinguishable from that of an atherosclerotic event, stress cardiomyopathy, or a myocardial infarction without epicardial obstructive lesions. (3,6,7)
Among the most common electrocardiographic findings, ST-segment elevation typically occurs in 20% to 50% of cases, and ventricular arrhythmias are present in 3–7% of cases. (1,3)
Clinical suspicion is based on the patient’s characteristics (age, sex and absence of cardiovascular risk factors). Coronary angiography is the firstline diagnostic test due to its availability. Its major limitation is that it allows for only twodimensional evaluation, precluding a complete characterization of the arterial walls. Therefore, in light of current evidence, the use of methods that better characterize the arterial walls, the true and false lumen, hematoma, and vessel tear is recommended, including intravascular ultrasound (IVUS) and OCT. (3,4,6)
The complexity of the modern methods described above lies in their availability, high cost, the risk of intimal tear, and lack of trained operators, which leads to a risk of complications affecting up to 8% of patients diagnosed or treated using these methods.
IVUS has been available for more than 20 years. It has a spatial resolution of 150 µm and allows for the characterization of intimal tears, false lumen, and intraluminal thrombi. OCT has revolutionized the diagnosis of SCAD since 2008. It has a spatial resolution of 10 to 20 µm, is superior to IVUS in delineating the lumenintima interface, and is suitable for visualizing intimal tears, stenosis, intramural hematomas, and false lumen. (1,3,6)
Angiographically, SCAD presents with moderate lesions in the middle or distal third with TIMI 3 distal flow. (14) The most commonly affected vessel is the anterior descending artery (32–46% of cases), followed by the circumflex artery (15–45%) and the right coronary artery (10–39%). Multivessel involvement has been reported in 9% to 23% of the remaining cases. (3) In an analysis of 132 patients with left main coronary artery dissection published by Morosato et al., 95% of cases presented as an ACS, and 36% occurred during pregnancy; in turn, 22% of cases progressed to cardiogenic shock and 8% with ventricular arrhythmias. (17)
Other characteristics that, in the absence of dissection, could increase diagnostic yield include coronary tortuosity, the presence of FMD, and scarring in the affected vessel. (6)
Angiographic Classification
The angiographic description of SCAD was developed by Saw et al. in 2014 and initially comprises three types. Since up to 25% of patients may present with dissections at more than one site, we suggest expanding the classification to include a fourth and fifth type, which complement the diagnosis of the disease and are currently undergoing validation. (5,18,19) (Figure 1)
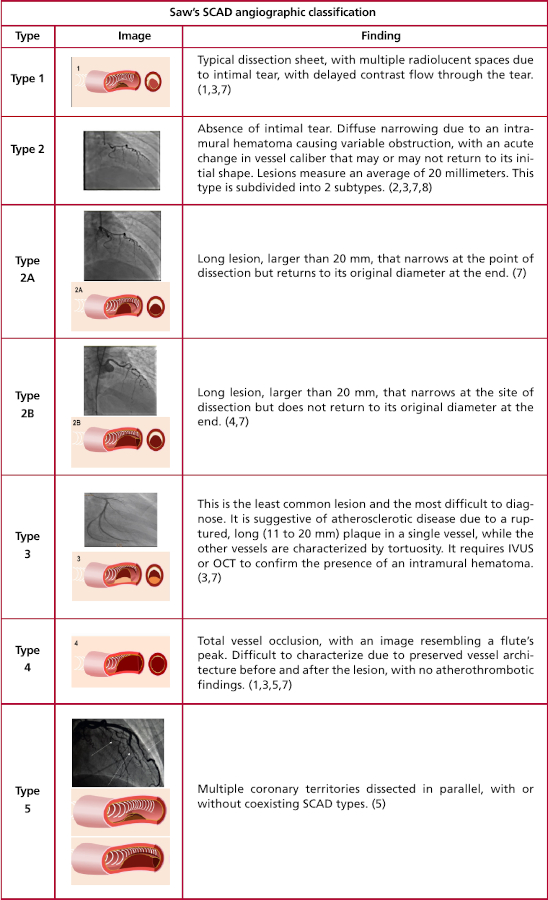
Type 1: It is characterized by a typical dissection sheet, evidenced by multiple radiolucent spaces (due to intimal tear) with contrast retention or delayed passage. (6,18)
Type 2: It occurs in 60% to 75% of cases and is characterized by the absence of intimal tear. Diffuse narrowing is observed due to the intramural hematoma, which causes variable obstruction, with an acute change in vessel caliber, which may or may not return to its initial form. The lesions are typically long and measure an average of 20 millimeters. They are subdivided into two types, and the intramural hematoma can be characterized using OCT. (6,17)
Type 2a: A long lesion, larger than 20 mm, that narrows at the site of dissection but returns to its original diameter at the end. (6,18)
Type 2b: A long lesion, larger than 20 mm, that narrows at the site of dissection but does not return to its original diameter at the end. (6,18)
Type 3: This is the least common and most difficult to diagnose of all SCAD types. The image is suggestive of atherosclerotic disease in a single vessel and is characterized by tortuous vessels elsewhere. Lesions are typically extensive (11 to 20 mm). It cannot be distinguished from a ruptured plaque, except through intravascular imaging that characterizes the compressive intramural hematoma. (6,18)
Type 4: It presents with total vessel occlusion, with a “flute peak” appearance. It is difficult to characterize because the vessel architecture is preserved both before and after the lesion, with no atherothrombotic findings. The definitive treatment is percutaneous. (5)
Type 5: Multiple coronary territories are dissected in parallel, with or without coexisting types of SCAD.
Definitive treatment must be interventional. (5)
Treatment
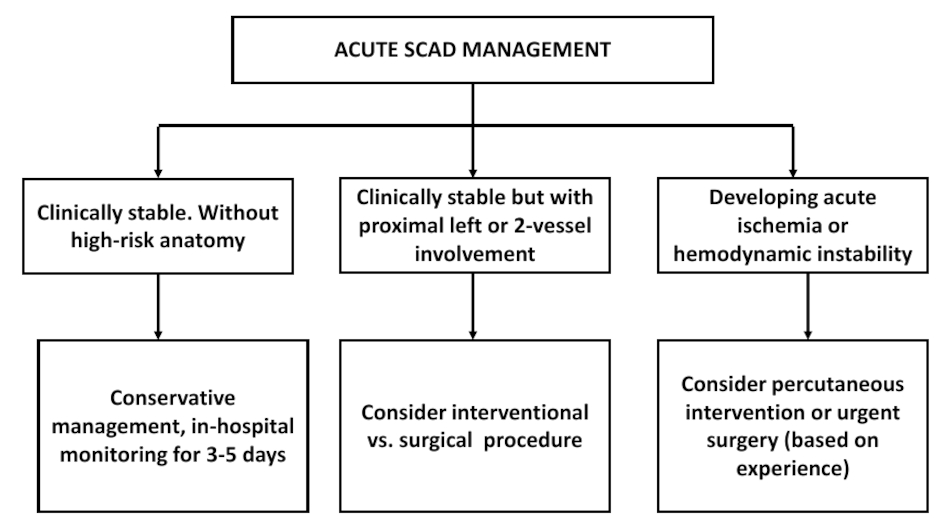
Based on the only prospective, multicenter study available to date, the recommendation is to analyze each case individually, aiming to choose conservative treatment over interventional treatment. (4) However, given the high risk of recurrence, some authors suggest invasive management from the outset. (17,20) (Table 1 and management algorithm in Figure 2).
Table 1
Recommended Treatment for Spontaneous Coronary Dissection
| Recommended treatment for SCAD | ||
|---|---|---|
| Treatment | Recommendation | Indication |
| Beta-blockers | + | Independent of LVEF. They reduce up to 64% the risk of recurrence. Their use is contraindicated during pregnancy. (1,9) |
| ACEI | - | Recommended in conjunction with a decrease in LVEF. Anti-remodeling effect. (1,7) |
| ARA II | - | Recommended in cases of ACEI intolerance and in conjunction with a decrease in LVEF: anti-remodeling effect. (1,7) |
| Aspirin | +/- | In cases of PCI: 3 months to 1 year of DAPT. (1,7) |
| P2Y12 | +/- | In cases of PCI: 3 months to 1 year of DAPT o (P2Y12 inhibitors?). (1,7) |
| Anticoagulation | - | Initial treatment for ACS. Once SCAD is confirmed, anticoagulation should be discontinued due to the pathophysiological mechanism and the potential spread of the hematoma. (1,7) |
| Statins | - | Not recommended. (1,7) |
| Antianginal agents | + | Their use should be recommended: 20% of patients experience persistent pain. (1,7) |
| Fibrinolysis | - | Contraindicated: increases the risk of dissection. |
| PCI | +/- | Complex or refractory cases. Indicated for active ischemia and type 4–5 dissec- tion. Risk of enlarging the dissection and stent migration. |
| CABG | +/- | Multivessel disease or left main coronary artery disease. Failed PCI or medical therapy. |
ACEI: Angiotensinconverting enzyme inhibitors; ACS: Acute coronary syndrome; ARA II: Angiotensin II receptor antagonist; CABG: Coronary artery bypass grafting; DAPT: Dual antiplatelet therapy; LVEF: Left ventricular ejection fraction; PCI: Percutaneous coronary intervention.
Conservative Treatment
The primary objectives are angina management, prevention of chronic pain and recurrence, and extracardiac vascular anomalies’ screening. Patients with impaired left ventricular systolic function should receive standardized treatment for this condition. Some observational data from angiography suggest that the majority (73–97%) of patients show improvement in scar formation at the site of the dissections after weeks or months. (7,13,14,21)
In highrisk cases—characterized by persistent pain, extensive and proximal dissection of a vessel, multivessel involvement, poor distal flow, shock, or ventricular arrhythmias—revascularization via percutaneous intervention or coronary artery bypass grafting is recommended, depending on the experience of each center. Due to the pathophysiology of the disease, fibrinolysis is contraindicated. (3,13,14)
Pregnancy and lactation are periods associated with an increased risk of toxicity transmission; therefore, the risk of mother-to-fetus transmission must be considered in any treatment.
Expert opinions suggest:
beta-blockers: They reduce wall stress and SCAD recurrence. This conclusion is based on an observational study of 327 patients, in which 64% of cases who used beta-blockers had a lower incidence of recurrence. (21) A metaanalysis on recurrence published in 2022 by Chi et al. confirmed the reduced risk of recurrence with beta-blockers (RR 0.51; 95% CI 0.33–0.77; p < 0.001). Their use is limited in pregnant women due to fetal bradycardia and intrauterine growth restriction. (22)
Antiplatelet therapy: Most patients are discharged on at least one antiplatelet agent. Regarding dual antiplatelet therapy, its continuation is recommended for a period ranging from one month to one year following a percutaneous coronary intervention. Beyond that, there is lack of scientific support. The evidence regarding the use of clopidogrel in pregnant women is unclear. (3,6)
Antianginal therapy: Pain following a dissection is common and accounts for approximately 20% of hospital admissions within 30 days after SCAD; it may even become chronic, so the use of antianginal therapy may be considered. (1)
Invasive treatment
Percutaneous coronary intervention (PCI) poses a significant challenge due to the risk of invading the false lumen and enlarging the dissection. The success rate varies among different cohort studies, ranging from 47% to 72%. With regard to the anatomical characteristics or the affected territory at the time of intervention, proximal dissections of one or multiple vessels are taken into account, particularly those of the anterior descending artery or the left main coronary artery. If adequate TIMI 2–3 flow is maintained, even in the presence of significant occlusion, medical management is recommended due to the risk of hematoma resorption and subsequent stent migration. (1,6,14) Coronary artery bypass grafting (CABG) is successful in the short term in most cases. It is rarely performed (1% of cases) and is reserved for cases of treatment failure with medical and percutaneous therapies. (6,14,20)
In the aforementioned report by Morosato et al., when treatment options were discussed, it was clarified that CABG was performed in 21% of cases, which reduced mortality compared with medical treatment alone; this allowed for the hypothesis that the intervention (PCI-CABG) in this group of patients is associated with a lower incidence of adverse events. (17)
The incidence of recurrent inhospital myocardial infarction is 5% to 10%, and the risk of extension of the same dissection is 17% during the first 2 weeks; half of these cases occur within 48 hours after discharge, so a minimum hospital stay of 5 days is recommended. (3,13)
Rehabilitation and Physical Activity
Available data show low adherence to cardiovascular rehabilitation. The evidence clearly demonstrates the benefits of rehabilitation and the safety of the process. It is recommended to follow the Vancouver General Hospital program for SCAD, based on exercise testing with blood pressure targets not exceeding 130/80 mmHg and a heart rate between 50% and 70% of the ageadjusted maximum. (3)
Special Considerations
Pregnancy-associated SCAD: Most events occur during the first 4 to 5 weeks postpartum. However, the disease can manifest at any stage of pregnancy, with reports even during the lactation period. (11,23) Most events present as ST-segment elevation ACS involving the left anterior descending artery, with higher morbidity and mortality than in the nonpregnant group. Recommendations regarding invasive diagnosis and treatment are similar to those for the nonpregnant group. (3,11,14,24)
Psychosocial considerations: Patients with SCAD present higher scores on distress, anxiety, and depression assessments, reduced physical capacity and greater emotional dependence. (3)
Assessment and management of chest pain following SCAD: Experience indicates that chest pain following SCAD is common and may occur in up to 50% of registered patients, becoming a problem in the emergency department. (3,6,14) The general approach is the same as for the first SCAD episode and indistinguishable from that for an atherosclerotic event. It is recommended that patients with persistent symptoms that are refractory to optimal medical treatment undergo further evaluation. (3)
Prognosis and Recurrence
The prognosis for this disease is favorable. Two forms of recurrence have been described: the first involves extension of the dissection due to acute expansion of the intramural hematoma; the second involves a new dissection in an artery other than the one previously affected, occurring more than 30 days after the initial event. The latter is the most widely accepted. Recurrence rates vary depending on study design, population scope, the definition of recurrence, and the final treatment provided. They range from approximately 5% at 22 months, 15% at 27 months, and 30% at 10 years. (25)
A meta-analysis that included 14 studies with 4206 SCAD patients analyzed risk factors associated with recurrence. The findings most strongly associated with recurrence were vascular anomalies, such as FMD (RR 2.02; 95% CI 1.03–3.94; p = 0.04) and hypertension (RR 1.49; 95% CI 1.05–2.12; p = 0.02). (26) Another notable characteristic of recurrence is that it appears to occur most often within the first week following the primary event, and it is more frequent in groups that received medical treatment than in those who underwent intervention. (26) There is no strong evidence to suggest that pregnancy is a clear predisposing factor for recurrence, as the limited available evidence comes from a small case series. (11)
Gaps in the Approach to the Disease
Many aspects of the disease remain unclear, ranging from predisposing factors to genetic and microvascular associations related to arterial collagen formation, as seen in FMD; moreover, the hormonal effects on the arterial wall and the spontaneous formation of intramural hematomas have not been fully elucidated. There is a significant gap in knowledge on the role of noninvasive diagnosis using coronary angiotomography and regarding treatment, the duration of beta-blocker use, single- or dual antiplatelet therapy as well as the management of psychosocial conditions that perpetuate the risk of disease recurrence remain undefined. (27) All of these factors provide sufficient reason to continue the search for new information based on local data, in order to gain a full understanding of the disease behavior and offer better treatment.
CONCLUSION
SCAD is a major cause of ACS in young people, particularly in perimenopausal women with few cardiovascular comorbidities. To date, no large randomized trials are available to evaluate all aspects related to the disease. However, large cohorts from industrialized countries provide insights into the possible etiology and pathogenesis, as well as diagnostic and therapeutic approaches. Clinical suspicion continues to play a fundamental role in ensuring an appropriate initial approach, with the aim of providing timely diagnosis and treatment.