ORIGINAL ARTICLE
Optimization of Door-to-Balloon Time Implementing a Process Improvement Program. Results after 5 Years
Optimización del tiempo puerta-balón mediante la implementación de un programa
de mejora de procesos. Resultados a 5 años de funcionamiento
Juan Furmento, Alfonsina
CandielloMTSAC, Pablo Máscolo, Pablo Lamelas, Ian Chapman, Alan
Sigal, Marcelo TriviMTSAC, Jorge BelardiMTSAC, Juan Pablo
CostabelMTSAC
By the
Ischemic Heart Disease Program from the Instituto
Cardiovascular de Buenos Aires (ICBA). Buenos Aires. Argentina
Address for reprints: Juan Pablo Costabel - Instituto Cardiovascular de Buenos Aires, Argentina. Blanco de Encalada 1543. 1428, Buenos Aires, Argentina. E-mail: jpcostabel@icba.com.ar
Rev Argent Cardiol 2023;91:135-139. http://dx.doi.org/10.7775/rac.v91.i2.20614
ABSTRACT
Background: If available, primary
transluminal
coronary angioplasty (PTCA),
performed timely and in experienced sites, is the best
reperfusion strategy for ST elevation myocardial infarction (STEMI). The
door-to-balloon (DTB) time expresses operational efficiency of the site in charge of the PTCA, with an impact on
patient’s progress. The aim of this study was to analyze the long-term results of a continuous improvement program for the DTB time process.
Methods:
Patients diagnosed
with STEMI who had undergone PTCA from January 2015 to May 2022 were prospectively
and consecutively enrolled. The
population was divided in two periods: an immediate implementation period and a
long-term follow-up period.
Results:
671 patients were
prospectively and consecutively enrolled. During the implementation period (P1)
91 patients were enrolled, and 580 during the program follow-up (P2). The
median (interquartile range, IQR) DTB time was 46 min (29-59) for P1 vs 42 min (25-52)
for P2, p=0.055). The second period showed a reduction in pre-activations (P1
54,1% vs P2 30 %, p=0.02)
and on-hour procedures (42% for P1 versus 30% for P2, p=0.029).
Conclusion: The registry showed long-term maintenance of good results,
despite reduced reactivations and on-hour procedures.
Key words:
Myocardial Infarction - Angioplasty - Time-to-Treatment
RESUMEN
Introducción: De
estar disponible, la angioplastia primaria (ATCp), en tiempos adecuados y en
centros con experiencia, es la mejor estrategia
de reperfusión para el infarto agudo de miocardio con supradesnivel del
segmento ST (IAMCEST). El tiempo puerta-balón
(TPB) es una expresión de eficiencia operativa de la institución que
realiza la ATCp, con impacto en la evolución del paciente. El objetivo
de este trabajo fue analizar los resultados
a largo plazo de un programa de mejora continua del proceso TPB.
Material y métodos: Se incluyeron en forma prospectiva y consecutiva pacientes con
diagnóstico de IAMCEST sometidos a ATCp desde
enero de 2015 a mayo de 2022. La población se dividió en dos períodos: período
de implementación inmediata y período de seguimiento a largo plazo.
Resultados: Se
ingresaron 671 pacientes en forma prospectiva y consecutiva. En el primer
período de implementación, (P1), se incluyeron 91 pacientes, y en el segundo
período, de seguimiento del programa, (P2), 580 pacientes. La mediana (rango intercuartilo, RIC) de TPB fue de 46 min (29-59) en P1 vs
42 min (25-42) en el P2, p=0,055). En el segundo período se evidenció una
reducción de las preactivaciones (P1 54,1% vs P2 30%, p=0,02) y los procedimientos on hours (42% en P1 vs 30% en P2, p=0,029).
Conclusión: El
registro mostró el mantenimiento de los buenos resultados a largo plazo a pesar
de una reducción de las preactivaciones y los procedimientos on hours.
Palabras clave: Infarto del miocardio
- Angioplastia - Tiempo de tratamiento
Received: 10/13/2022
Accepted: 02/01/2023
INTRODUCTION
Primary angioplasty (primary
transluminal
coronary angioplasty, PTCA) has shown to be the best therapy for the management of ST elevation
myocardial infarction (STEMI),
when performed timely
and in experienced sites. (1–4) Total myocardial ischemia time, from the onset of symptoms to reperfusion, is a major predictor factor in these patients. (5) The time elapsed
from the arrival of the patient to the healthcare center to the opening of the artery,
door-to-balloon (DTB) time,
is considered one of the main hospital care quality indicators. (6–8) Some tools have proven to be of benefit to reduce such time, and therefore,
our site developed a protocol in January 2015 to reduce DTB time.
The initial results of the program were published
in 2016 on this journal,
so the aim of this study is to analyze the long-term
results of such program. (9)
METHODS
Study design
The program began in January 2015, and our previous
article analyzed the results of the “working”
phase, from October 2015 to May 2016. In order to
evaluate long-term results, we have
compared the immediate implementation period
of the program (P1), from October 2015 to May 2016, against long-term follow-up of the program (P2), from June 2016 to May 2022.
As specified in the cited publication, the institution’s door-to-balloon program is developed
by a multidisciplinary team with representatives from different areas: admission
(administrative and security staff), external emergency room (doctors and
nurses), staff in charge of patient transfer
(stretcher-bearers and assistants), hemodynamics (doctors, nurses, and technicians). (9)
DTB time is defined as the time elapsed from patient’s admission
to catheter guidewire insertion
through coronary obstruction,
as recommended by international clinical guidelines. The time of catheter guidewire passage
is recorded in the angiography
machine, providing the possibility of subsequent audits.
DTB time data are monthly
reported by the Patient Safety team in our site, with staff outside the DTB program.
Working hours, when the service
was available upon admission of a STEMI patient, were from Monday to Friday, from 7 am to 8 pm (on-hour). Beyond this time, service activation was considered as non-working hours (off-hour). The initial program
included a set of strategies with evidence of DTB time reduction. These tools were maintained
until the time of writing this paper.
Ready Catheterization lab: The possibility of having the catheterization lab in good conditions
to perform the procedure off-hours.
This allows the patient to be admitted and
prepared for the intervention before the arrival of the hemodynamics team.
Bypassing the ER: Direct access to the catheterization lab for patients
admitted through the emergency room (ER) after diagnosis, to avoid delays.
ER pre-activation:
Hemodynamics team activation after the request for referral to the site of the patient
diagnosed with STEMI, from his home or from an institution. The interventionist’s activation occurs upon a single
call from admission, both to the ER and the interventional team, after receiving the referral call
from the domicile or from a referring site.
Single activation call: One single phone call by the on-duty
clerk to the member of the Hemodynamics team in charge that day,
reduces the number of communication exchanges from the ER.
Informing of program activation through loud- speakers: Activation process is informed in this way, so that each
member involved performs the corresponding tasks, and individual calls are avoided.
Statistical analysis
For quantitative data description, the mean and standard deviation (SD) or median and interquartile range (IQR) were used as applicable. Categorical
variables were described using absolute numbers and percentages. For variables
comparisons, Chi-square test, t-test or Mann-Whitney test were used as applicable. A two-tailed p value
of <0.05 was considered
to be statistically significant. The Kruskal-Wallis
test was performed for multiple group median comparisons. The SPSS statistical package was used (version 22.0 SPSS Inc., Chicago,
IL).
Ethical considerations
Informed consent was required to take part in the study.
Approval by the Ethics and Training Committee was obtained, and the principles of the Declaration of
Helsinki were followed.
RESULTS
A total of 671 patients were prospectively and consecutively
enrolled over 2 periods. During the implementation period (P1) 91 patients were
enrolled, and 580 during the program follow-up
(P2) (Table 1).
Table 1. Comparison of the 2 periods
|
Variable |
Period 1 91 patients |
Period 2 580 patients |
p |
|
Age –
years-median (IQR) |
60.1
(53.1-70.7) |
62
(54-73) |
0.221 |
|
Men –
n (%) |
69
(76) |
469
(81) |
0.585 |
|
Radial
artery access – n (%) |
182
(92.9) |
83
(96.5) |
0.083 |
|
Primary
angioplasty – n (%) |
170
(86.8) |
78
(89.7) |
0.014 |
|
Killip
& Kimball A-B -n (%) |
80
(88) |
516
(89) |
0.839 |
|
Times |
|||
|
Direct
consultation – n (%) |
27
(29) |
300
(52) |
0.001 |
|
Emergency
system - n (%) |
64
(71) |
280
(48) |
0.001 |
|
Pre-activation
- n (%) |
49
(54.1) |
174
(30) |
0.021 |
|
Bypassing ER – n (%) |
45 (46) |
160 (27.5) |
0.001 |
|
On-hour
– n (%) |
38
(42) |
174
(30) |
0.029 |
|
DTB
time – min-median (IQR) |
46
(29-49) |
42
(25-42) |
0.119 |
|
DTB time lower than
90 min – n (%) |
84
(92) |
562
(97) |
0.055 |
DTB: door-to-balloon. ER: emergency room. IQR: interquartile range.
Baseline characteristics showed no differences as regards mean age and sex of patients. The percentage of patients undergoing the procedure as PTCA was slightly
higher in P2 (89.7% vs 86.8%), with no differences in
the rate of radial artery access or the hemodynamic condition upon admission.
During P1, 71% of patients
were admitted through ER versus 48% in P2 (p=0.001), which was associated with a higher rate of ER
pre-activation (54% vs 30%, p=0.02) and bypassing ER. The rate of on-hour procedures was reduced from 42% in P1 to
30% in P2 (p=0.029).
The DTB time was similar
in both periods: 46 min (IQR 29-59) in P1 vs 42 (IQR 25-52) in P2, with a 97%
of patients below target time of 90 minutes in P2. (Figures 1 and 2).

Fig. 1. Median door-to-balloon time (min) over time
Q: quarter
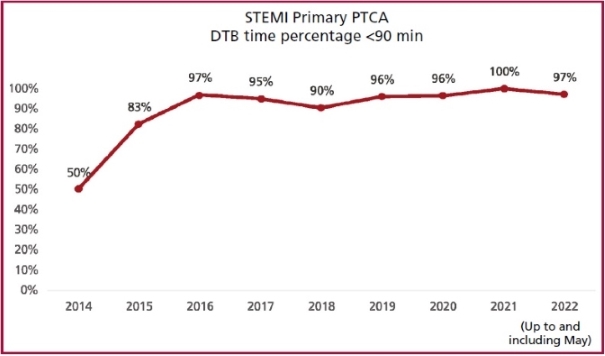
Fig. 2. PTCA in less than 90 minutes
over time
DTB: door-to-balloon time. PTCA: primary
transluminal
coronary angioplasty. STEMI: ST elevation myocardial infarction
DISCUSSION
Our experience shows that it is possible to maintain a DTB time optimization process in a site
over time. We have hierarchically ordered these five findings.
First, the program showed the capacity to maintain a
proper DTB time, with more than 97% of patients below 90 minutes, and 80% below
60 minutes. These results
are comparable to those reported
by other institutions
worldwide. (1,10)
Maintaining such a process throughout
5 years, with staff changes and institutional development, requires a coordinated effort for the task to become natural and be passed from one person to the other in all groups
taking part. Long-term success of
this type of processes depends on
having a defined list of objectives and the ability to obtain performance metrics; therefore, programs also need the capacity to measure performance
indicators. These are specific to the context
affecting each site
and country. The working group should meet regularly to analyze performance and discuss any
required adjustment. Please note that the process continued
even throughout the pandemics. (11)
Second, a key process to reduce DTB time is pre-activation,
which enables the site to be prepared, so that everything is ready for prompt reperfusion as soon as the patient
arrives. The pre-hospital ECG allows for early identification and pre-hospital
management of STEMI patients and affects both clinical decision-making and
choice of target hospital. Prior notice to
the receiving hospital shortens reperfusion therapy times and allows actions to be taken there. (6) When comparing both periods, there seems to be a reduction in this phenomenon, which might be
explained by a reduced communication
flow between the site and the ambulance
systems, the inclusion of the pandemics in the
analysis, and the fragmentation of the outpatient medical emergency system in the city of Buenos Aires. It is worth pointing out that, despite
this reduction, the DTB time remained low, although it
definitely represents an opportunity for improvement.
Third, bypassing ER has also shown to reduce inhospital ischemia times. Studies have shown that long emergency service times contribute to a
substantial proportion of general
delays between identified patients and pre-hospital STEMI activation. (8,12–14) The protocols used to bypass ER and take patients
with suspected infarction directly to the Cath
lab have been associated with improved
results. Reduced use of this strategy in P2 seems to be directly
linked to reduced pre-activations. However, this may happen not necessarily with a pre-activation, but
just by evaluating patients with chest pain and an electrocardiogram, upon
arrival of the ambulance. Fortunately, for the
past few years, many emergency systems have had an ECG machine
inside the ambulance
when chest pain is the activation diagnosis. It is still necessary to continue to interpret and disclose the benefits of pre-activation.
Fourth, please note that these strategies are applicable
to other healthcare systems, provided they are
part of institutional
programs and performed after analysis of the barriers
at the site. The latter
is of major importance, as different systems
and sites pose different
barriers. The management process for patients
with STEMI requires
the action of different players at
the receiving site and joint efforts to optimize the delay. (15,16)
Fifth, we are aware that optimal
STEMI treatment should be based on using networks of hospitals with different levels of healthcare
connected by an efficient ambulance service. (17) This type of network reduces
delayed treatment and increases the proportion of patients receiving
reperfusion. Much work is pending in
this sense in the city of Buenos Aires. Work
teams from scientific associations involved in initiatives such as Stent-Save a Life! Argentina
have the mission to improve STEMI patients access
to quality reperfusion treatments in
order to reduce morbidity and mortality. (18,19) However, to achieve
these goals, it is essential to begin with the internal
organization of our sites in
order to be incorporated in these networks though efficient
work.
LIMITATIONS
This is a retrospective analysis of a prospective database.
This ensures consecutive patients, but limits
process data for analysis.
CONCLUSIONS
The study shows that door-to-balloon program effectiveness
could be maintained, despite reduced pre-activations and inclusion of the pandemics in the process.
Conflicts of interest
None declared.
(See authors' conflict
of interests forms on the web/Additional material.)
![]() https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista
Argentina de Cardiología
1. Chandrashekhar Y, Alexander
T, Mullasari A, Kumbhani DJ, Alam S, Alexanderson E, et al. Resource and
Infrastructure-Appropriate Management of ST-Segment Elevation
Myocardial Infarction in Low- and Middle-Income Countries. Circulation
2020;141:2004–25. https://doi.org/10.1161/CIRCULATIONAHA.119.041297
2. Blancas R, López-Matamala B, Martínez-González Ó, Ballesteros-Ortega D. Primary angioplasty versus fibrinolysis in
ST-segment elevation acute
myocardial infarction: Reassessing the best strategy. Med Intensiva 2013;37:499. https://doi.org/10.1016/j.medin.2013.05.003
3. Zeymer U, Schröder R, Machnig T, Neuhaus KL. Primary
percutaneous transluminal coronary
angioplasty accelerates early myocardial reperfusion compared to thrombolytic
therapy in patients with acute myocardial infarction. Am Heart J 2003;146:686–91. https://doi.org/10.1016/S0002-8703(03)00326-0
4. Keeley EC, Boura JA, Grines CL. Primary angioplasty versus intravenous
thrombolytic therapy for acute myocardial infarction: a quantitative review of 23 randomised
trials. Lancet 2003;361:13–20. https://doi.org/10.1016/S0140-6736(03)12113-7
5. Tai MH,
Shepherd J, Bailey H, Williams N, Hatz M, Campos Tapias I, et al. Real-world treatment patterns of PCSK9
inhibitors among patients
with dyslipidemia in Germany, Spain,
and the United Kingdom. Curr Med Res Opin 2019;35:829–35. https://doi.org/10. 1080/03007995.2018.1532885
6. Cheskes S, Turner
L, Foggett R, Huiskamp M, Popov D, Thomson
S, et al. Paramedic contact
to balloon in less than 90 minutes:
A successful strategy for st-segment elevation
myocardial infarction bypass to
primary percutaneous coronary intervention in a Canadian emergency medical
system. Prehosp Emerg Care
2011;15:490–8. https://doi.org/10.3109/10903127.2011.598613
7. Wang YC, Lo PH, Chang SS, Lin JJ, Wang HJ, Chang CP, et al. Reduced
door-to-balloon times in acute ST-elevation myocardial infarction
patients undergoing primary percutaneous coronary intervention. Int J Clin Pract
2012;66:69–76. https://doi.org/10.1111/j.1742-1241.2011.02775.x
8. Gross BW, Dauterman KW, Moran MG, Kotler
TS, Schnugg SJ, Rostykus PS, et al. An
Approach to Shorten Time to Infarct Artery Patency in Patients With ST-Segment Elevation Myocardial Infarction. Am J Cardiol
2007;99:1360–3. https://doi.org/10.1016/j.amj-card.2006.12.058
9. Nau G, Lalor N, Costabel JP, Pedernera G, Morales P, Candiello A, et al. Optimization of Door-to-Balloon Time Implementing a Process Improvement Program. Rev Argent
Cardiol (English) 2017;85:117-23. http://dx.doi.org/10.7775/rac.v85.i2.9172
10.
De Luca G, Biondi-Zoccai G, Marino P. Transferring
Patients With ST-Segment
Elevation
Myocardial
Infarction
for Mechani- cal Reperfusion: A Meta-Regression Analysis
of Randomized Trials. Ann Emerg Med. 2008;52:665–76. https://doi.org/10.1016/j.annemergmed.2008.08.033
11.
Costabel JP, Muñoz F, Máscolo P, Candiello A, Viruel M, Belardi J. Infarto agudo
de miocardio en pandemia COVID-19. Medicina (B Aires). 2021;81:887–9.
12. Bajaj S,
Parikh R, Gupta N, Aldehneh A, Rosenberg M, Hamdan A, et al. “Code STEMI” protocol
helps in achieving reduced door-to- balloon times in patients
presenting with acute ST-segment elevation
myocardial infarction during off-hours. J Emerg
Med 2012;42:260–6. https://doi.org/10.1016/j.jemermed.2011.03.014
13. Kontos MC, Kurz MC, Roberts CS, Joyner SE, Kreisa L, Ornato JP, et al. Emergency physician-initiated cath
lab activation reduces door to
balloon times in ST-segment elevation myocardial infarction patients. Am J Emerg
Med 2011;29:868–74. https://doi.org/10.1016/j.ajem.2010.03.025
14. Bagai A, Al-Khalidi HR, Muñoz D, Monk L, Roettig ML, Corbett
CC, et al. Bypassing the emergency department and time to reperfusion in patients with prehospital ST-segment-elevation: findings
from the reperfusion in acute myocardial infarction in Carolina
Emergency Departments project. Circ Cardiovasc Interv 2013;6:399–406. https://doi.org/10.1161/CIRCINTERVENTIONS.112.000136
15.
Pereira H, Calé R, Pereira E, Mello S, Vitorino S,
Jerónimo de Sousa P, et al. Five years of Stent for Life in Portugal.
Rev Port Cardiol 2021;40:81–90. https://doi.org/10.1016/j.repc.2020.05.018
16. Jollis JG, Al-Khalidi HR, Roettig ML, Berger PB, Corbett CC, Doerfler SM, et al. Impact of Regionalization
of ST-Segment-Elevation Myocardial Infarction Care on
Treatment Times and Outcomes for Emergency Medical
Services-Transported Patients Presenting to Hospitals With Percutaneous Coronary
Intervention: Mission: Lifeline Accelerator-2. Circulation 2018;137:376–87. https://doi.org/10.1161/CIRCULATIONAHA.117.032446
17. Mullasari AS, Victor SM, Alexander
T. STEMI India:
reimagining STEMI networks in low- and middle-income countries: Reimagining
STEMI. AsiaIntervention [Internet] 2022;8:17–23. https://doi.org/10.4244/AIJ-D-22-00012
18. Candiello A, Alexander T, Delport
R, Toth GG, Ong P, Snyders A, et al. How to set up regional
STEMI networks: a “Stent – Save a life!” initiative. EuroIntervention 2022;17:1313–7. https://doi.org/10.4244/EIJ-D-21-00694
19. Pereira H, Naber C, Wallace
S, Gabor T, Abdi S, Alekyan B, et al. Stent-Save a Life international
survey on the practice of primary percutaneous coronary
intervention during the COVID-19 pandemic.
Rev Port Cardiol 2022;41:221–7. https://doi.org/10.1016/j.repc.2021.04.006