INTRODUCCIÓN
La aterosclerosis es la causa más frecuente de enfermedad de las arterias carótidas extracraneales y una de las principales causas de enfermedad cerebrovascular (ECV), y muerte. 1,2 Constituye la etiología predominante de ECV en Occidente. 3 Empero, existen otras causas no ateroscleróticas, como fibrodisplasia, enfermedad de Takayasu y disección aórtica, entre otras, que se relacionan con ECV. 1,4 Dentro de este grupo se incluyen las dolicoarteriopatías (del griego δόλιχος, dólichos, “anormalmente largo”), que han sido depositarias de la atención de los especialistas en los últimos tiempos. Las dolicoarteriopatías carotídeas (DAC), se han asociado a un amplio espectro de ECV, como el ictus y el accidente isquémico transitorio (AIT). 5 Sin embargo, su significado clínico real resulta poco claro. 1 En el presente trabajo, revisamos los principales aspectos de las DAC, centrándonos en su fisiopatología, diagnóstico, pronóstico y tratamiento.
MÉTODOS
Se efectuó una revisión no sistemática, seleccionando los trabajos más significativos vinculados con este tópico. Se utilizaron los buscadores PubMed, Scielo y Scholar Google, empleando las siguientes palabras: dolichoartheriopathies, carotid dolichoartheriopathies, arterial tortuosity, dolichoectasia, y sus equivalentes en español.
RESULTADOS
Definición, clasificación y epidemiología
Las DAC constituyen una anomalía anatómica consistente en un cambio de disposición geométrica que provoca enrollamiento, acodamiento y tortuosidad de los vasos carotídeos en su trayecto. 1,5 Algunos autores las incluyen dentro del grupo de las dolicoectasias (elongación, tortuosidad y/o dilatación de los vasos). 6 Las DAC fueron descritas por primera vez por Kelly en 1925 7, y clasificadas por Weibel y Fields 8 (Figura 1), en tres grupos:
-
Tipo I o Tortuosidad (Tortuosity): Cualquier elongación u ondulación en S o C del curso de la arteria carótida, con una angulación mayor de 90°.
-
Tipo II o Enrollamiento (Coiling): Alargamiento o redundancia de la arteria carótida interna, dando una curva en S exagerada, o en una configuración circular, adquiriendo morfología en asa (una angulación de 360° de la arteria sobre su eje transverso).
-
Tipo III o Acodamiento (Kinking): Angulación de uno o más segmentos de la arteria, con ángulo menor de 90°.
FIGURA 1
Esquema de la clasificación de las dolicoarteriopatías carotídeas, uniendo las de Weibel-Fields y Metz. La ilustración de la clasificación de Weibel-Fields se modificó de la referencia #41. La ilustración de clasificación de Metz se modificó de la referencia #5.
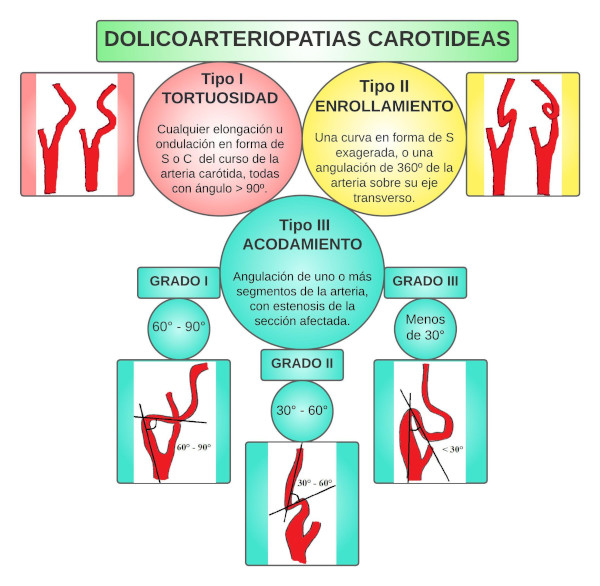
Metz y cols. subclasificaron los acodamientos en función de la severidad de la angulación: Grupo I (ángulo agudo medido entre los dos segmentos que forman la torsión de una amplitud entre 90° y 60°, Figura 2, Panel A), Grupo II (entre 60° y 30°, Figura 2, Panel B), y Grupo III (menor de 30°, Figura 2, Panel C). 9
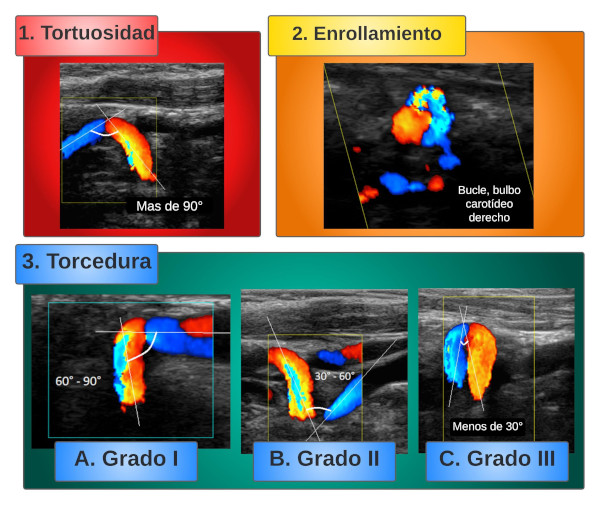
FIGURA
2 - Imágenes de diferentes tipos de dolicoarteriopatías carotídeas obtenidas con ecocardiografía Doppler color. El ángulo entre cada parte de la arteria se dibuja con líneas blancas y se describe en la imagen correspondiente.
Las DAC son una entidad frecuente, con una prevalencia del 10 - 45%. 10 Beigelman y cols. (1, y Ghilardi y cols., 11 diagnosticaron DAC en 13,3 - 31 % de los casos, mientras que en estudios de pacientes hospitalizados, la prevalencia osciló entre el 13,5 y el 58 %. 6 Las DAC son más prevalentes en mujeres y pacientes añosos, especialmente mayores de 60 años, y pueden ser tanto uni como bilaterales, afectando las arterias carótida común (ACC), interna (ACI) y externa (ACE), pero más frecuentemente la ACI, especialmente del lado izquierdo. 12,13 Las tortuosidades y los acodamientos son más frecuentes que los enrollamientos. 1,12
Fisiopatología
Varios mecanismos han sido implicados en el desarrollo de DAC, aunque aún existe controversia. Una cuestión clave es si es un fenómeno congénito o adquirido, y si tiene alguna relación con la aterosclerosis u otros factores de riesgo cardiovascular. Algunos estudios arrojan luz al respecto.
A. Mecanismo embriológico
La vasculatura cerebral comienza a desarrollarse tempranamente en el embrión, durante la tercera semana de vida intrauterina, mediante la formación de los arcos aórticos (AA). 13,14 Hay seis pares de AA que conectan la aorta ventral (AV) con la aorta dorsal (AD). 14,15 Cada AA surge del bulbo arterioso, y discurre dentro de su arco faríngeo correspondiente para terminar en la AD. 14 Los arcos primero y segundo se desintegran, y sus raíces nacientes de la AV y AD persisten como ACI y ACE incipientes. La ACI se integra con el tercer AA bilateralmente, mientras que la raíz aórtica ventral, entre el tercer y cuarto arco, persiste como ACC. 15 Existe una variabilidad considerable en el curso y la posición de las ACC y las bifurcaciones carotídeas. La elongación de las ACC y ACI conduce a tortuosidad y acodamientos. 16 La posición de la bifurcación carotídea refleja el grado de migración embriológica de la ACE, y es variable. 16 Huber y cols. situaron la bifurcación carotídea a nivel de C4 - C5 en el 48% de 658 casos, y de C3 - C4 en el 34%. 17 Hay casos descritos de bifurcación desde T3 hasta C2. 18 En niños, se observó de C2 a C3 en un 40%, y de C3 a C4 en un 40%. 19 Carney y cols. encontraron tortuosidades en 5 de 20 fetos entre los 5 meses y a término. 20 Harrison y cols. sugirieron que el desarrollo de las arterias carótidas y del sistema esquelético puede ser asincrónico, generando alteraciones y tortuosidad en el trayecto de la arteria. 21 Beigelman y cols. estudiaron una población de 885 personas (4,5 horas postnatales - 90 años), y los dividieron en un grupo control con 245 personas (niños y adolescentes hasta 15 años), y otro de 640 individuos (16 - 90 años), en los que se había solicitado eco Doppler color de vasos de cuello por sospecha clínica de aterosclerosis. La incidencia de enrollamientos y acodamientos fue similar en ambos grupos. La presencia de placas ateromatosas en la tortuosidad solo se observó en 3 pacientes del segundo grupo. Los autores encontraron una falta de asociación con otros factores de riesgo cardiovascular, y de la localización de las placas carotídeas con las DAC. 1
B. Trastornos genéticos y moleculares
Voevoda y cols. estudiaron 61 familias cuyos niños habían sido diagnosticados previamente con DAC de la ACI mediante ecografía Doppler dúplex color. El grupo estuvo compuesto por 100 individuos con esta alteración. El grupo control (n = 245) se formó a partir de un banco de ADN basado en un enfoque poblacional. Encontraron una asociación entre el polimorfismo A80807T del gen del factor transcripcional Sp4 con las DAC. 22 Zaidi y cols. reportaron el caso de una familia kurda consanguínea cuyo niño presentaba elongación y tortuosidad severa de la aorta, carótidas y otras arterias, incluyendo otras alteraciones (piel floja, hiperlaxitud articular, hernias y rasgos faciales que se asemejan al síndrome de Ehler-Danlos [SED]). Encontraron homocigosidad del locus 20q13 en el niño afectado. 23 Arslan y cols. observaron un nivel significativamente mayor de metaloproteinasa de matriz (MMP) tipo 2 en pacientes con DAC en comparación con el grupo control. La expresión de MMP-12 fue mayor en aquellos con placas ateromatosas que en aquellos sin aterosclerosis. 24
C. Enfermedades del tejido conectivo (ETC)
Foiadelli y cols. reportaron el caso de 7 niños con SED de entre 3 a 13 años, con DAC y manifestaciones clínicas variables. 25 Welby y cols. estudiaron 286 pacientes divididos en grupos control y con ETC. La presencia de DAC fue del 44% en el segundo grupo, y del 16% en los controles (p < 0,001). Los enrollamientos fueron más prevalentes. Se vio DAC en el 88 % de los casos con síndrome de Marfan, 63% para el síndrome de Loeys-Dietz, 42% para la neurofibromatosis tipo 1, y 19% para el SED, tanto del tipo vascular como no vascular. 26
D. Asociación con otras enfermedades congénitas
Según Paltseva y cols., las DAC tienen niveles de elastina más altos, pero con fragmentación de fibras, mayor expresión de MMP-9, y una menor expresión de actina de músculo liso. 27 Ballotta y cols. analizaron 78 arterias carótidas con DAC y encontraron patrones típicos y atípicos de displasia fibromuscular (DFM). 28 Sethi y cols. encontraron una prevalencia significativamente mayor de DAC con curva en forma de S en pacientes con DFM. 29
Ballota y cols. estudiaron a 43 pacientes con aneurisma de aorta abdominal (AAA) asintomáticos y DAC, y encontraron cambios displásicos degenerativos en la túnica media en todas las muestras carotídeas. En algunos casos, se superpusieron con lesiones ateroscleróticas de la íntima. Las características histológicas del AAA clásico (adelgazamiento de la túnica media subyacente a la placa aterosclerótica), se observaron en casi todas las muestras de la pared aórtica, sugiriendo una base común de alteraciones del tejido conectivo subyacente a ambas patologías. 30
E. Mecanismos adquiridos
Harrison y cols. sostienen que las DAC podrían deberse a cifosis o lordosis que desviarían el eje carotídeo. 21 Para Etheredge y cols., la inflamación de los tejidos pericarotídeos haría que estas se retraigan y desvíen su camino, desarrollando tortuosidades. 31
Ghilardi y cols., y Del Corso y cols., describen una gran prevalencia de hipertensión arterial (HTA) y aterosclerosis en pacientes con DAC. 11,32 Sin embargo, ambos estudios carecen de un grupo de participantes normales, y abordan únicamente una población seleccionada por patología vascular, en los que se espera un predominio de dichos factores de riesgo cardiovascular. Para Khasiyev y cols., debido a que las DAC también muestran dilatación, la remodelación externa compensatoria en respuesta a la aterosclerosis puede desempeñar un papel en este fenotipo. 6 La dilatación de la carótida también puede reflejar una debilidad del tejido conectivo de índole no aterosclerótica. Pancera y cols. encontraron una asociación estadísticamente significativa entre acodamiento e HTA, y también entre la presencia de HTA y mayor grado de flexión del acodamiento. 33 Oliviero y cols. estudiaron la prevalencia de DAC en pacientes con HTA y diabetes. La prevalencia de DAC fue mayor en el grupo HTA que en el de diabetes y control, y también se asoció con el tiempo que los pacientes fueron hipertensos. 34 Las fuerzas excéntricas relacionadas con la HTA, y posiblemente el envejecimiento de la arteria, acompañado del desarrollo de rigidez, puede desempeñar un papel en la dilatación de la ACI y, por lo tanto, en el desarrollo de las DAC. 6
Wang y cols. estudiaron la relación entre el índice de masa corporal (IMC) y las DAC. Analizaron un total de 513 pacientes, todos ellos sin ETC, empleando el índice de tortuosidad (IT), expresado en porcentaje, calculado como una relación entre la longitud real de la ACI (LR) y la longitud medida desde la bifurcación carotídea hasta la base del cráneo, llamada longitud del cordón (LC):
El sexo masculino y el IMC se correlacionaron significativamente con el IT. Por cada punto del IMC aumentó 1,59 veces el riesgo de desarrollar DAC. 35 Dilba y cols. utilizaron el mismo índice en una población de la cohorte Plaque At RISK. Concluyeron que la edad, la obesidad y la hipercolesterolemia se asocian con mayor IT. Además, encontraron mayor prevalencia y severidad de DAC en la ACI izquierda. La elevación del IMC y las DAC puede deberse a la presión abdominal alta. El aumento de la presión abdominal puede empujar hacia arriba el diafragma, y con él, todo el mediastino. Esto elevaría las arterias carótidas que, al estar rodeadas de tejido conectivo laxo, pueden deslizarse y desarrollar tortuosidad. Debido a que la arteria braquiocefálica “absorbe” parte de la fuerza de elevación, la ACI derecha desarrolla una tortuosidad menos grave que la izquierda. Así, la exposición repetida y prolongada a periodos de alto y bajo flujo deriva en estrés que afecta el remodelado arterial, provocando tortuosidad. 36
Derubertis y cols. observaron mayor prevalencia de DAC en pacientes previamente sometidos a radioterapia. La radiación puede devenir en retracción y alteración del tejido conectivo, produciendo tortuosidad de la arteria. 37 Saba y cols. estudiaron una población de 124 pacientes con disección de ACI diagnosticada mediante tomografía computarizada (TC) o resonancia magnética (RM). Observaron una asociación estadísticamente significativa entre la disección y el acodamiento y enrollamiento . 38 Barbour y cols. encontraron una asociación significativa entre disección arterial espontánea y tortuosidad de la ACI, especialmente si la torsión es bilateral. 39 Algunos autores plantean que las alteraciones hemodinámicas pueden producir ruptura y daño endotelial. La inflamación desencadenada puede alterar la estructura del vaso, y los agentes inflamatorios derivar en disección arterial. 6
Diagnóstico
Las DAC se pueden diagnosticar mediante un amplio espectro de técnicas de imagen. El estándar de oro parece ser la ultrasonografía. 1,2,6 El flujo sanguíneo turbulento dentro de los vasos tortuosos se puede estudiar con exploración Doppler. 40 Di Pino y cols. estudiaron la prevalencia de DAC en ACI empleando eco Doppler color en 2856 sujetos (0-96 años), y demostraron picos de prevalencia en los extremos etarios (<21 años y >60 años). Se detectaron DAC en el 9,9% de los participantes. Este estudio fue uno de los primeros en utilizar ultrasonografía en una gran cohorte. 41 Uchino y cols. comunicaron un caso de DAC diagnosticado por angiografía por tomografía computarizada (TC) y tomografía computarizada por emisión de fotón único (SPECT). Ambas permitieron estudiar con mayor definición la morfología de la tortuosidad de la ACI y las alteraciones secundarias de la perfusión. 42 En otros trabajos, la TC permitió evaluar anomalías finas, como microaneurismas, y las reconstrucciones 3D de la TC impresionan ser más eficaces a la hora de clasificar las variaciones morfológicas de la ACI y detectar estas anomalías. 43,44,45 Balevi y cols. encontraron una prevalencia de DAC del 40,3%. en la población general mediante angioresonancia (angio-RM) con contraste. 12 Tomiya y cols. realizaron angio-RM en 13 pacientes, obteniendo imágenes nítidas de DAC. 46 Yu y cols. opinan que la RM es una buena opción para el diagnóstico de las DAC. La angiografía por sustracción digital (ASD), estándar de oro para el diagnóstico de enfermedades de los vasos cervicales e intracraneales, podría proporcionar datos hemodinámicos de las DAC y estudiar su morfología, pero no puede determinar los cambios patológicos a nivel de la pared de la ACI. 40 Funcionaría como un complemento en el estudio de las DAC más que una técnica de imagen útil para el diagnóstico. Para llegar a un diagnóstico correcto, todas estas técnicas son válidas y no excluyentes, y deberían elegirse en orden de mayor complejidad e invasividad.
Implicancia clínica
La implicancia clínica de las DAC es controvertida. Hay evidencia limitada para apoyar la asociación entre DAC y ECV. 6 Yin y cols. observaron una mayor incidencia de lesiones de sustancia blanca en aquellos pacientes con DAC en comparación con controles. La gravedad de estas lesiones se relacionó directamente con el número de acodamientos. 47 Otros autores sostienen que la enfermedad isquémica es más frecuente en personas con DAC y otros factores de riesgo cardiovascular. Pancera y cols. encontraron una asociación significativa entre acodamientos y AIT. La HTA y las DAC podrían ser factores de riesgo aditivos en la fisiopatología de los AIT. 33 Oliviero y cols. demostraron que la presencia de acodamiento carotídeo en sujetos hipertensos no puede considerarse un factor de riesgo adicional para eventos isquémicos. 48 Pero, como afirman Pancera y cols., la adición de factores de riesgo a la presencia de DAC puede aumentar el riesgo de eventos vasculares. 33 Iwai-Takano y cols. observaron una asociación entre las DAC y el envejecimiento, la HTA y el género, pero no con dislipidemias, diabetes o tabaquismo. 49
Quienes apoyan el peligro de las DAC sostienen que las curvas en la ACI, además de estrechar la arteria y generar daño endotelial, pueden producir turbulencias en el flujo sanguíneo que devendrían en un estado protrombótico. Para otros, como Balevi y cols., las DAC son más una curiosidad que un verdadero predictor de eventos isquémicos. 12 Valvano y cols. abogan por la ausencia de asociación entre DAC y ECV. 50 Las DAC pueden causar hipoperfusión cerebral, llevando a encefalopatía, vértigo, diplopía, AIT e infarto. 40 La prevalencia de síntomas cerebrovasculares en pacientes con DAC varía entre el 15 y el 23%. 51 El enrollamiento no se considera un factor de riesgo para eventos isquémicos debido a su débil asociación con los síntomas, a diferencia de los acodamientos, que impresionan ser más sintomáticos debido a la hipotensión transitoria durante el sueño o al movimiento repentino y extremo de la cabeza y el cuello. 40 Otras alteraciones observadas son la discapacidad visual como la amaurosis fugax, uveítis, retinitis y distrofia macular. 52 En casos graves, las DAC pueden producir efecto de masa, dando lugar a disfagia, disnea, estrechamiento de la vía aérea superior y apnea obstructiva, y, más raramente, acúfenos pulsátiles y espasmo mesolingual. 40,53,54
Sobre la relación entre las DAC y la aterosclerosis, en el Northern Manhattan Study (NOMAS), Khasiyev y cols. estudiaron la relación entre DAC y biomarcadores de aterosclerosis en 558 participantes. Las DAC se correlacionaron con la presión arterial diastólica y el gran diámetro de la raíz aórtica, pero no con otras medidas de aterosclerosis. Determinar el riesgo de eventos vasculares asociados a este fenotipo no aterosclerótico puede ayudar a una mejor estratificación del riesgo para las personas con DAC. 55
Beigelman y cols. estudiaron la génesis de las complicaciones neurológicas relacionadas con las DAC. Sesenta pacientes con DAC sin aterosclerosis fueron sometidos a pruebas de rotación cefálica y estudiados mediante Doppler color de las ACI y oftálmicas, y se evaluó en estas últimas su comportamiento hemodinámico. Los resultados sugirieron que las DAC no son causa de alteraciones o síntomas neurológicos, ya que no se registraron eventos durante el estudio, y se constató reducción significativa de las velocidades en la arteria oftálmica en solo 3 de 60 casos. 56
Wang y cols. analizaron las variaciones de presión provocadas por las DAC en 12 pacientes mediante ASD. Midieron el ángulo de acodamiento mediante angiografía rotacional y calcularon la presión arterial en los sitios proximal, intra-acodamiento y distal de la ACI empleando un microcatéter. Estos resultados se compararon con dos simulaciones: una numérica, con un modelo geométrico de ACI tortuosa construido con un software; y otra de flujo in vitro, utilizando un tubo de silicona sometido a diferentes grados de torsión, a través del cual fluía agua impulsada por una bomba peristáltica. La simulación del software mostró una caída lineal de la presión del flujo con disminuciones en el ángulo de torsión. La mínima caída de presión fue en el ángulo de torsión de 180º, y la máxima en 30º. Pero ocurrió una inversión entre 30º y 20º: el aumento del grado de acodamiento condujo a una caída menor de la presión. Lo mismo ocurrió con la simulación in vitro: cuando el caudal era constante, la caída de presión disminuyó al aumentar el ángulo de torsión, pero se incrementó al aumentar el mismo de 20º a 30º. Sin embargo, estos hallazgos no se correspondieron con las observaciones clínicas: las pruebas realizadas en pacientes mostraron un aumento notable de la caída de presión cuando el ángulo de torsión era inferior a 30º, el acodamiento marcado indujo una disminución promedio del 15,5 % en la presión arterial. En la medición clínica no se observó el desarrollo de la inversión de caídas de presión con ángulos superiores a 20º - 30º. Esto se atribuyó a una excesiva elongación y estenosis de la ACI en casos de torsiones graves. Y aunque la caída de presión cambió gradualmente en las simulaciones, disminuyó rápidamente en las mediciones clínicas cuando el ángulo era menor de 45º, pero fue más gradual con ángulos más altos. Este comportamiento podría ser causado por las características del fluido (la sangre es un fluido no newtoniano), y las paredes elásticas de la ACI. Ambos factores crearían un “rango protector” que puede contribuir al mecanismo de autorregulación del flujo sanguíneo. 57 Dicho trabajo fue uno de los primeros estudios en evaluar estos aspectos de las DAC comparando observaciones clínicas y artificiales, con mediciones directas de las presiones de la ACI. Estos hallazgos evidencian que las alteraciones de la presión arterial y el flujo sanguíneo pueden ser las responsables de la interrupción de la perfusión cerebral, de isquemia consecuente y, por lo tanto, eventos cerebrovasculares.
Algunos autores observaron una relación entre DAC y aneurismas en el contexto de las ETC. 26 El valor predictivo positivo de la combinación de aneurisma de aorta y DAC asociada a ETC fue del 95,4%, con una especificidad del 98,6%. Un mayor IT de las arterias aorta y vertebral se comportó como predictor independiente de disección arterial en pacientes con síndrome de Marfan. Así, las DAC permiten sospechar la presencia de aneurismas de gran importancia clínica en pacientes con ETC. 6,26,40
Las DAC se han relacionado con mayor morbimortalidad en los procedimientos quirúrgicos de cabeza y cuello. Ya en los trabajos de Weibel y Fields 8 y Metz (9 se conocía este riesgo. Nayak y cols. remarcan la importancia de estudiar la morfología de los vasos carotídeos antes de realizar procedimientos quirúrgicos en la zona faríngea, ya que pueden complicarse con lesión de los vasos, sangrado y, en casos graves, muerte por hemorragia masiva. 58 Por ello, resulta perentorio su estudio exhaustivo previo a la realización de cualquier procedimiento en la zona cervical.
Tratamiento
A pesar de la controversia sobre la implicancia clínica de las DAC, se han elaborado algunas indicaciones terapéuticas para actuar sobre ellas en función del grado de compromiso hemodinámico de la tortuosidad, entre otros parámetros. Gavrilenko y cols. 59 propusieron tratar las DAC en las siguientes condiciones:
-
1. Estenosis de la ACI del 60% o más, con placas ateroscleróticas y cualquier grado de insuficiencia cerebrovascular; o,
-
2. Estenosis de la ACI inferior al 60 % con placas ateroscleróticas, grado moderado a grave de insuficiencia cerebrovascular, en combinación con tortuosidad, flujo sanguíneo lineal de 100 cm/seg o más, y flujo sanguíneo turbulento.
Grego y cols. (60) propusieron casos específicos en los que se justifica el tratamiento, tales como:
-
a) AIT (síntomas hemisféricos);
-
b) Pacientes asintomáticos con ángulo de acodamiento menor de 30°, con oclusión carotídea contralateral;
-
c) Pacientes con síntomas no hemisféricos, tras descartar otras posibles causas neurológicas o no neurológicas mediante resultados positivos de los siguientes estudios: 1) ecografía Doppler de vasos de cuello con aumento de velocidades, 2) TC y angio-RM cerebral con lesiones isquémicas en hemisferio ipsilateral, y 3) inversión del flujo circulatorio en la arteria cerebral anterior y su reducción en la arteria cerebral media, en relación con maniobras de rotación y flexoextensión cefálica.
Otros autores propusieron iniciar tratamiento en casos de cociente ACI/carótida común mayor de 2, o velocidad del flujo sanguíneo mayor de 180 cm/seg (61,62. Pero la indicación real de tratamiento de las DAC sigue siendo controvertida. La mayoría concuerdan en intervenir los casos de DAC sintomáticas descartando cualquier otra causa.
Se han propuesto técnicas invasivas para corregir las DAC, con resultados exitosos (fijación de la ACI al músculo digástrico, anastomosis término-terminal, reimplantación término-lateral, endarterectomía carotídea con parche, bypass y angioplastia carotídea, y colocación de stent). 40 Sin embargo, a pesar del éxito de estas técnicas, el tratamiento adecuado sigue siendo controvertido. Son necesarios más estudios para determinar la efectividad real del abordaje quirúrgico de las DAC.
CONCLUSIÓN
Las DAC son una entidad común, con etiología multifactorial y evidencia limitada, pero no despreciable, de compromiso cerebrovascular. Son necesarios más estudios que establezcan la utilidad de las estrategias terapéuticas para mejorar su pronóstico. Un control estricto y un seguimiento más cercano de los pacientes, con una valoración global del riesgo tromboembólico, son medidas prudentes para prevenir futuros eventos.
BIBLIOGRAFÍA
1. Beigelman R, Izaguirre AM, Robles M, Grana DR, Ambrosio G, Milei J. Are kinking and coiling of carotid artery congenital or acquired? Angiology. 2010;61:107-12. https://doi.org/10.1177/0003319709336417
2. Beigelman RL, Izaguirre AM, Azzato F, Milei J. Carotid Artery - Pathology, Plaque Structure - Relationship between Histological Assessment, Color Doppler Ultrasonography and Magnetic Resonance Imaging - Dolichoarteriopathies - Barorreceptors. In: Rezzani R, editor. Carotid Artery Disease - From Bench to Bedside and Beyond [Internet]. London: IntechOpen; 2014. https://doi.org/10.5772/57157
3. The global burden of disease: 2004 update. World Health Organization (WHO) Press; 2008. http://www.nhlbi.nih.gov/health/health-topics/topics/catd/[Online]
5. Dilba K, van Dam-Nolen DHK, Crombag GAJC, van der Kolk AG, Koudstaal PJ, Nederkoorn PJ, et al. Dolichoarteriopathies of the extracranial internal carotid artery: The Plaque At RISK study. Eur J Neurol 2021;28:3133-8. https://doi.org/10.1111/ene.14982
6. Khasiyev F, Gutierrez J. Cervical Carotid Artery Dolichoectasia as a Marker of Increased Vascular Risk. J Neuroimaging. 2021;31:251-60. https://doi.org/10.1111/jon.12815
7. Kelly AB. Tortuosity of the internal carotid in relation to the pharynx. J Laring 1925;40:15-20. https://doi.org/10.1177%2F003591572401700607
8. Weibel J, Fields WS. Tortuosity, coiling and kinking of the internal carotid artery.Etiology and radiographic anatomy. Neurology.1965;15:7-18. https://doi.org/10.1212/wnl.15.1.7
9. Metz H, Murray-Leslie RM, Bannister RG, Bull JW, Marshall J. Kinking of the internal carotid artery. Lancet. 1961;1:424-6. https://doi.org/10.1016/s0140-6736(61)90004-6
10. Verlato F, Camporese G, Rocco S, Salmistraro G, Signorini GP. Carotid kinks relationship to atherosclerosis and cerebral ischemia. J Vasc Surg. 2000;32:293-8. https://doi.org/10.1067/mva.2000.106953
11. Ghilardi G, De Monti M, Longhi F, Trimarchi S, Bortolani E. Prevalenza del kinking carotideo in unapopolazioneresidente. Risultatiparzialidelprogramma OPI (ObiettivoPrevenzione Ictus) [Prevalence of carotid kinking in a resident population. Partial results of the OPI (Objective Prevention of Ictus)]. Minerva Cardioangiol. 1993;41:129-32.
12. Balevi M. Dolicho-Arteriopathies (Kinking, Coiling, Tortuosity) of the Carotid Arteries: A Study by Magnetic Resonance Angiography. Int J Neck Head Surg, 2020;11:50-4. https://doi.org/10.5005/jp-journals-10001-1405
13. Valvano A, Bosso G, Apuzzi V, Mercurio V, Di Simone V, Panicara V, et al. Long-term follow-up in high risk hypertensive patients with carotid dolicoarteriopathies. Int Angiol. 2020;39:24-8. https://doi.org/10.23736/S0392-9590.19.04229-9
14. Bertulli L, Robert T. Embryological development of the human cranio-facial arterial system: a pictorial review. Surg Radiol Anat. 2021;43:961-73. https://doi.org/10.1007/s00276-021-02684-y
18. Vitek JJ, Reaves P. Thoracic bifurcation of the common carotid artery. Neuroradiology. 1973;5:133-9. https://doi.org/10.1007/BF00341527
23. Zaidi SH, Peltekova V, Meyer S, Lindinger A, Paterson AD, Tsui LC, et al. A family exhibiting arterial tortuosity syndrome displays homozygosity for markers in the arterial tortuosity locus at chromosome 20q13. Clin Genet 2005;67:183-8. https://doi.org/10.1111/j.1399-0004.2004.00391.x.
24. Arslan Y, Arslan IB, Pekçevik Y, Sener U, Köse S, Zorlu Y. Matrix Metalloproteinase Levels in Cervical and Intracranial Carotid Dolichoarteriopathies. J Stroke Cerebrovasc Dis 2016;25:2153-8. https://doi.org/10.1016/j.jstrokecerebrovasdis.2016.05.028
25. Foiadelli T, Ippolito R, Corbetta R, Simoncelli AM, Amariti R, Licari A, et al. Clinical variability in children with dolichoarteriopathies of the internal carotid artery. Childs Nerv Syst 2020;36:621-8. https://doi.org/10.1007/s00381-019-04395-7.
26. Welby JP, Kim ST, Carr CM, Lehman VT, Rydberg CH, Wald JT, et al. Carotid Artery Tortuosity Is Associated with Connective Tissue Diseases. AJNR Am J Neuroradiol 2019;40:1738-43. https://doi.org/10.3174/ajnr.A6218
27. Paltseva EM, Oskolkova SA, Polyakova VO, Krylova YS, Ivanova AG, Abramyan AV, et al. [The structure of the internal carotid artery wall in pathological tortuosity]. Arkh Patol 2015;77:3-8. Russian. https://doi.og/10.17116/patol20157753-8
28. Ballotta E, Thiene G, Baracchini C, Ermani M, Militello C, Da Giau G, et al. Surgical vs medical treatment for isolated internal carotid artery elongation with coiling or kinking in symptomatic patients: a prospective randomized clinical study. J Vasc Surg 2005;42:838-46; discussion 846. https://doi.org/10.1016/j.jvs.2005.07.034
29. Sethi SS, Lau JF, Godbold J, Gustavson S, Olin JW. The S curve: a novel morphological finding in the internal carotid artery in patients with fibromuscular dysplasia. Vasc Med 2014;19:356-62. https://doi.org/10.1177/1358863X14547122
31. Etheredge SN, Effeney DJ, Ehrenfeld WK. Symptomatic extrinsic compression of the cervical carotid artery. Arch Neurol 1984;41:672-3. https://doi.org/10.1001/archneur.1984.04210080084020
32. Del Corso L, Moruzzo D, Conte B, Agelli M, Romanelli AM, Pastine F, et al. Tortuosity, kinking, and coiling of the carotid artery: expression of atherosclerosis or aging? Angiology 1998;49:361-71. https://doi.org/10.1177/000331979804900505
33. Pancera P, Ribul M, Presciuttini B, Lechi A. Prevalence of carotid artery kinking in 590 consecutive subjects evaluated by Echocolordoppler. Is there a correlation with arterial hypertension? J Intern Med 2000;248:7-12. https://doi.org/10.1046/j.1365-2796.2000.00611.x
34. Oliviero U, Cocozza M, Picano T, Policino S, Russo N, Fazzio S, et al. Prevalence of carotid kinking and coiling in a population at risk.Vasc Surg 1997;31:43-9. https://doi.org/10.1177/153857449703100106
35. Wang HF, Wang DM, Wang JJ, Wang LJ, Lu J, Qi P, et al. Extracranial Internal Carotid Artery Tortuosity and Body Mass Index. Front Neurol. 2017;8:508. https://doi.org/10.3389/fneur.2017.00508
36. Dilba K, van Dam-Nolen DHK, Crombag GAJC, van der Kolk AG, Koudstaal PJ, Nederkoorn PJ, et al. Dolichoarteriopathies of the extracranial internal carotid artery: The Plaque At RISK study. Eur J Neurol 2021;28:3133-8. https://doi.org/10.1111/ene.14982
37. Derubertis BG, Hynecek RL, Kent KC, Faries PL. Carotid tortuosity in patients with prior cervical radiation: increased technical challenge during carotid stenting. Vasc Endovascular Surg. 2011;45:619-26. https://doi.org/10.1177/1538574411408745
38. Saba L, Argiolas GM, Sumer S, Siotto P, Raz E, Sanfilippo R, et al. Association between internal carotid artery dissection and arterial tortuosity. Neuroradiology 2015;57:149-53. https://doi.org/10.1007/s00234-014-1436-x.
39. Barbour PJ, Castaldo JE, Rae-Grant AD, Gee W, Reed JF 3rd, Jenny D, et al. Internal carotid artery redundancy is significantly associated with dissection. Stroke. 1994;25:1201-6. https://doi.org/10.1161/01.str.25.6.1201.
40. Yu J, Qu L, Xu B, Wang S, Li C, Xu X, et al. Current Understanding of Dolichoarteriopathies of the Internal Carotid Artery: A Review. Int J Med Sci. 2017;14:772-84. https://doi.org/10.7150/ijms.19229
41. Di Pino L, Franchina AG, Costa S, Gangi S, Strano F, Ragusa M, et al. Prevalence and morphological changes of carotid kinking and coiling in growth: an echo-color Doppler study of 2856 subjects between aged 0 to 96 years. Int J Cardiovasc Imaging. 2021;37:479-84. https://doi.org/10.1007/s10554-020-02014-0
42. Uchino A, Kohyama S. Long segment dolichoectasia of the right internal carotid artery diagnosed by CT angiography. Radiol Case Rep. 2019;14:1084-7. https://doi.org/10.1016/j.radcr.2019.06.013
43. Mamedov FR, Arutiunov NV, Usachev DIu, Lukshin VA, Beliaev AIu, Mel'nikova-Pitskhelauri TV, et al. [Neuroradiological diagnostics of atherosclerotic lesions and kinking of the carotid arteries in determination of indications to surgical treatment]. Zh Vopr Neirokhir Im N N Burdenko. 2011;75:3-10.
44. Nagata T, Masumoto K, Hayashi Y, Watanabe Y, Kato Y, Katou F. Three-dimensional computed tomographic analysis of variations of the carotid artery. J Craniomaxillofac Surg. 2016;44:734-42. https://doi.org/10.1016/j.jcms.2016.02.011
46. Tomiya Y, Chiba S, Moriyama H, Kikuchi Y, Ohta M. [Eighteen cases of tortuosity of the internal carotid--usefulness of MR-angiography in diagnosis]. Nihon Jibiinkoka Gakkai Kaiho. 1995;98:1367-72. Japanese. https://doi.org/10.3950/jibiinkoka.98.1367
47. Yin L, Li Q, Zhang L, Qian W, Liu X. Correlation between cervical artery kinking and white matter lesions. Clin Neurol Neurosurg. 2017;157:51-4. https://doi.org/10.1016/j.clineuro.2017.04.003
49. Iwai-Takano M, Watanabe T, Ohira T. Common carotid artery kinking is a predictor of cardiovascular events: A long-term follow-up study using carotid ultrasonography. Echocardiography 2019;36:2227-33. https://doi.org/10.1111/echo.14536
50. Valvano A, Bosso G, Apuzzi V, Mercurio V, Di Simone V, Panicara V, et al. Long-term follow-up in high risk hypertensive patients with carotid dolicoarteriopathies. Int Angiol. 2020;39:24-8. https://doi.org/10.23736/S0392-9590.19.04229-9
51. Metz H, Murray-Leslie RM, Bannister RG, Bull JW, Marshall J. Kinking of the internal carotid artery. Lancet. 1961;1:424-6. https://doi.org/10.1016/s0140-6736(61)90004-6
53. Sismanis A, Girevendoulis A. Pulsatile tinnitus associated with internal carotid artery morphologic abnormalities. Otol Neurotol. 2008;29:1032-6. https://doi.org/10.1097/MAO.0b013e3181865913
55. Khasiyev F, Rundek T, Di Tullio MR, Wright CB, Sacco RL, Elkind MSV, et al. Systemic Arterial Correlates of Cervical Carotid Artery Tortuosity : The Northern Manhattan Study. Clin Neuroradiol. 2022;32:435-43. https://doi.org/10.1007/s00062-021-01044-y
57. Wang L, Zhao F, Wang D, Hu S, Liu J, Zhou Z, et al. Pressure Drop in Tortuosity/Kinking of the Internal Carotid Artery: Simulation and Clinical Investigation. Biomed Res Int. 2016;2016:2428970. https://doi.org/10.1155/2016/2428970
58. Nayak SB, Shetty SD. Surgical and embryological perspective of a big loop of internal carotid artery extending laterally beyond internal jugular vein. Surg Radiol Anat. 2021;43:413-16. https://doi.org/10.1007/s00276-020-02619-z
59. Gavrilenko AV, Kuklin AV, Khripkov AS, Abramian AV. Otsenka éffektivnosti rekonstruktivnykh operatsii na sonnykh arteriiakh v sochetanii stenoza i patologicheskoi izvitosti [Assessment of efficacy of reconstructive operations on carotid arteries in combination of stenosis and pathological tortuosity]. Angiol Sosud Khir. 2014;20:116-22. Russian.
61. Illuminati G, Ricco JB, Caliò FG, D'Urso A, Ceccanei G, Vietri F. Results in a consecutive series of 83 surgical corrections of symptomatic stenotic kinking of the internal carotid artery. Surgery. 2008;143:134-9. https://doi.org/10.1016/j.surg.2007.07.029
Información del Artículo
License:  Esta obra esta bajo una Licencia Creative Commons Atribución 4.0 Internacional.
:
Esta obra esta bajo una Licencia Creative Commons Atribución 4.0 Internacional.
:
License: Esta obra esta bajo una Licencia Creative Commons Atribución 4.0 Internacional.
:
HTML generado desde un archivo xml-jats con la plantilla jats-rac.xsl. El motor utilizado es Apache Software Foundation (Xalan XSLTC).
INTRODUCTION
Carotid artery atherosclerosis is the most common cause of extracranial carotid artery disease and is one of the leading causes of cerebrovascular disease (CVD) and death, 1,2 constituting the predominant etiology of CVD in Western countries. 3 However, other non-atheromatous causes of carotid disease are also related with CVD such as fibrodysplasia, Takayasu disease, and aortic dissection. 1,4 Dolichoarteriopathies (from the Greek δόλιχος, dolichos, "abnormally long") have recently attracted the attention of specialists and are included within non-atheromatous carotid artery diseases. Carotid dolichoarteriopathies (CDA) have been associated with a wide range of CVD, including stroke and transient ischemic attack (TIA). 1 However, their clinical significance remains unclear. 1 This article reviews the main aspects of CDA, focusing on its pathophysiology, diagnosis, prognosis, and treatment.
METHODS
We conducted a non-systematic review and selected the most relevant papers on this topic. PubMed, Scielo, and Scholar Google electronic databases were searched using the terms "dolichoartheriopathies," "carotid dolichoartheriopathies," "arterial tortuosity," "dolichoectasia," and their equivalents in Spanish.
RESULTS
Definition, classification and epidemiology
CDA are anatomical anomalies that result in a change in the geometric arrangement of the carotid vessels along their course, that causes coiling, kinking, and tortuosity. 1,5 Some authors include them within the group of dolichoectasias (vessel elongation, tortuosity and/or dilatation). 6 First described by Kelly in 1925, 7 CDA were classified by Weibel and Fields, 8 in three groups (Figure 1):

-
Type I or tortuosity: any S-shaped or C-shaped elongation or undulation of the course of the artery with an angulation >90°.
-
Type II or coiling: the internal carotid artery forms an exaggerated, redundant S-shaped curve or its longitudinal axis makes a complete circle (360°).
-
Type III or kinking: Angulation of one or more segments of the artery, with an angle < 90°.
-
Metz et al. sub-classified kinking based on the value of the acute angle between the two segments forming the kink in group I (between 90° and 60°, Figure 2, Panel A), group II (between 60° and 30°, Figure 2, Panel B) and group III (>30°, Figure 2, Panel C). 9

CDA are common, with a reported prevalence of 10-45%. 10 Beigelman et al. 1, and Ghilardi et al. 11 made the diagnosis of CDA in 13.3-31% of the cases, while in studies conducted in hospitalized patients, the prevalence ranged between 13.5% and 58%. 6 They are more prevalent in women and elderly patients, especially those > 60 years, and can be unilateral or bilateral, affecting the common carotid artery (CCA), internal carotid artery (ICA) and external carotid artery (ECA), but more commonly the ICA, especially on the left side. 12,13 Tortuosity and kinking are more common than coiling. 1,12
Pathophysiology
The development of CDAs has been linked to several mechanisms, although there is still some debate about the exact causes. A key question is whether they are congenital or acquired and whether they are related to atherosclerosis or other cardiovascular risk factors. Some studies shed light on the subject.
A. Embryology
The cerebral vasculature begins to develop early in the embryo, during the third week of intrauterine life, with the formation of the aortic arches (AA). 13,14 There are six pairs of AA connecting the ventral aorta (VA) to the dorsal aorta (DA). 14,15 Each AA arises from the bulbus arteriosus, and courses in its corresponding pharyngeal arch to end in the DA. 14 The first and second arches regress, and their remnants from the VA and DA persist as incipient ICA and ECA. The ICA merges bilaterally with the third AA, while the ventral aortic root between the third and fourth arches persists as the CCA. 15 There is considerable variability in the course and position of the CCA and carotid bifurcations. Elongation of the CCA and ICA results in tortuosity and kinking. 16 The position of the carotid bifurcation reflects the degree of embryologic migration of the ECA and is variable. 16 Huber et al. reported the position of the carotid bifurcation at C4 to C5 in 48% and at C3 to C4 in 34% of 658 bifurcations. 17 There are cases described of bifurcations from T3 to C2. 18 In children, bifurcation position from C2 to C3 was observed in 40% of cases and from C3 to C4 in 40% of cases. 19 Carney et al. found tortuosity in 5 of 20 fetuses of ages ranging from 5 months to full term. 20 Harrison et al. suggested that the development of carotid arteries and skeletal system might be asynchronous, causing changes and tortuosity in the course of the artery. 21 Beigelman et al. studied a population of 885 individuals ranging from newborns (4 hours 30 minutes) to 90 years. The study population was divided into two groups: a control group of 245 individuals (children and adolescents up to 15 years old) and another group of 640 individuals (16-90 years old) in whom diagnostic color Doppler ultrasonography of the neck vessels had been requested because of clinical suspicion of atherosclerotic vascular disease. The incidence of coiling and kinking was similar in both groups. The presence of atheromatous plaques in tortuous arteries was only observed in 3 group 2 patients. The authors found a lack of correlation with other cardiovascular risk factors, and of the site of carotid artery plaques with CDA. 1
B. Genetic and molecular disorders
Voevoda et al. examined 61 families of children with previously diagnosed ICA dolichoarteriopathy using color Duplex ultrasound. The group comprised 100 individuals with ICA dolichoarteriopathy. Control group (n=245) was formed from DNA bank based on a population approach. The authors found an association between A80807T polymorphism of the transcriptional factor Sp4 gene and CDA. 22 Zaidi et al. reported the case of a consanguineous Kurdish family whose child had severe elongation and tortuosity of the aorta, carotid and other arteries, along with other changes (loose skin, joint hypermobility, hernias, and facial features resembling Ehler-Danlos syndrome [EDS]). By homozygosity mapping, they found evidence of the involvement of the locus at chromosome 20q13 in the affected child. 23 Arslan et al. observed significantly higher matrix metalloproteinase-2 (MMP-2) levels in patients with CDA compared to the control group. The expression of MMP-12 was higher in those with atheromatous plaques than in those without atherosclerosis. 24
C. Connective tissue diseases (CTD)
Foiadelli et al. reported the case of 7 children with EDS between 3 and 13 years of age, with CDA and variable clinical manifestations. 25 Welby et al. evaluated 286 patients divided into control group and CTD group. The presence of CDA was 44% in the second group, and 16% in controls (p < 0.001). Coiling was more prevalent. The prevalence of CDA was 88% in Marfan syndrome, 63% in Loeys-Dietz syndrome, 42% in neurofibromatosis type 1, and 19% in patients with both vascular and nonvascular types of EDS. 26
D. Association with other congenital diseases
According to Paltseva et al., CDA have higher elastin levels but with fiber fragmentation, higher MMP-9 expression, and lower smooth muscle actin expression. 27 Ballotta et al. analyzed 78 carotid arteries with dolichoarteriopathy and found typical and atypical patterns of fibromuscular dysplasia (FMD). 28 Sethi et al. found a significantly higher prevalence of CDA with S-shaped curve in patients with FMD. 29
Ballota et al. analyzed 43 patients with asymptomatic abdominal aortic aneurysm (AAA) and CDA and found degenerative dysplastic changes in the tunica media in all carotid specimens; in a few cases, nonobstructive atherosclerotic intimal lesions were superimposed. The histologic features of classic AAA (thinning of the media underlying the atherosclerotic plaque) were observed in almost all aortic wall specimens, suggesting underlying connective tissue disorders in both conditions. 30
E. Acquired mechanisms
Harrison et al. suggest that CDAs may be due to kyphosis or lordosis, which would deviate the carotid axis. 21 For Etheredge et al., inflammation of the pericarotid tissues would cause retraction of the carotid arteries and deviate them from their path, resulting in tortuosity. 31
Ghilardi et al. and Del Corso et al. describe a high prevalence of hypertension (HTN) and atherosclerosis in patients with CDA. 11,32 However, both studies lacked a control group of normal subjects and addressed only a population selected because of vascular disease, in which these cardiovascular risk factors are expected to predominate. For Khasiyev et al., because CDA also show dilatation, compensatory external remodeling in response to atherosclerosis may play a role in this phenotype. 6 Dilatation of the carotid arteries may also be a sign of connective tissue weakness of a non-atherosclerotic nature. Pancera et al. found a statistically significant association between kinking and HTN, and also between HTN and kinking with a greater degree of bending. 33 Oliviero et al. analyzed the prevalence of CDA in patients with HTN and diabetes. The prevalence of CDA was significantly higher in the group of hypertensive patients than in diabetics and controls and was also associated with the duration of hypertension. 34 The eccentric forces related to HTN and possibly artery aging with stiffness may play a role in ICA dilatation and, thus, in the development of CDA. 6
Wang et al. evaluated the association between body mass index (BMI) and CDA. They analyzed 513 patients without CTD using the tortuosity index (TI) expressed as a percentage, calculated as the ratio between the actual length of the ICA (AL) and the length measured from the carotid bifurcation to the base of the skull, called the cord length (CL):
Male sex and BMI were significantly correlated with the TI. For each increase in BMI of 1 kg/m2, there was a 1.59-fold increase in the risk of developing CDA. 35 Dilba et al. used the same index in a population of the Plaque At RISK study and concluded that age, obesity and hypercholesterolemia were associated with higher TI. They also found higher prevalence and severity of CDA in the left ICA. Higher BMI and CDA could be due to high intra-abdominal pressure which may result in an upward shift of the diaphragm and a rise of the mediastinum. This would push up the carotid arteries, which, surrounded by lax connective tissue, can slip and become tortuous. Because the brachiocephalic artery "absorbs" part of the lifting force, the right ICA develops less severe tortuosity than the left. Thus, repeated and prolonged exposure to periods of high and low flow results in stress that affects arterial remodeling and causes tortuosity. 36
Derubertis et al. observed a higher prevalence of CDA in previously irradiated patients. Radiation can cause retraction and alteration of the connective tissue, resulting in tortuosity of the artery. 37 Saba et al. analyzed a population of 124 patients with ICA dissection diagnosed by computed tomography (CT) or magnetic resonance imaging (MRI) and found a statistically significant association between dissection and kinking and coiling. 38 Barbour et al. found a significant association between spontaneous ICA dissection and tortuosity, particularly if tortuosity is present bilaterally. 39 Some authors propose that changes in hemodynamics might lead to the local disruption of the endothelial integrity which trigger inflammation that can modify the structure of the vessel, and the release of inflammatory agents might predispose to carotid dissection. 6
Diagnosis
A diagnosis of CDA can be made by many imaging tests. Ultrasound seems to be the gold standard. 1,2,6 The turbulent blood flow inside the tortuous vessels can be evaluated with Doppler scanning. 40 Di Pino et al. studied the prevalence of dolichoarteriopathies of the ICA using color Doppler ultrasound in 2856 subjects (0-96 years) and demonstrated peaks of prevalence distributed in a bimodal fashion (< 21 years and > 60 years). CDA were detected in 9.9% of participants. This study was one of the first to use ultrasound in a large cohort. 41 Uchino et al. reported a case of CDA diagnosed by computed tomography (CT) angiography and single photon emission computed tomography (SPECT). Both tests better defined the morphology of ICA tortuosity and secondary perfusion abnormalities. 42 In other studies, CT allowed the evaluation of subtle abnormalities, such as microaneurysms, and 3D reconstructions of
CT appear to be more effective in classifying morphological variations of the ICA and detecting
these anomalies. (43-45) Balevi et al. found a prevalence of CDA of 40.3% in the general population using contrast-enhanced magnetic resonance angiography (MRA). 12 Tomiya et al. performed MRA in 13 patients and obtained very clear images of CDA. 46 Yu et al. believe that MRA is a good option for the diagnosis of CDAs. Digital subtraction angiography (DSA) remains the gold standard for the diagnosis of cervical and intracranial vascular disease, could provide hemodynamic data and show the morphology of CDAs in detail, but cannot determine the pathological changes of the arterial wall of the ICA. 40 It would serve as a complementary imaging test in the study of CDAs rather than a useful imaging test for diagnosis. All these techniques are valid and not mutually exclusive and should be chosen in order of increasing complexity and invasiveness to make a correct diagnosis.
Clinical implication
The clinical implication of CDA is controversial. There is limited evidence to support the association between CDA and CVD. 6 Yin et al. observed a higher incidence of white matter lesions in patients with CDA compared to controls. The severity of these lesions was directly related to the number of kinks. 47 Other authors argue that ischemic disease is more common in people with CDA and other cardiovascular risk factors. Pancera et al. found a significant association between kinking and TIA. Hypertension and CDA could be additive risk factors in the pathophysiology of TIA. 33 Oliviero et al. demonstrated that the presence of carotid kinking in hypertensive subjects may not be considered a further risk factor for ischemic events. 48 But, as Pancera et al. state, the addition of risk factors to the presence of CDA may increase the risk of vascular events. 33 Iwai-Takano et al. observed an association between CDA and aging, HTN and sex, but not with dyslipidemias, diabetes or smoking. 49
Those who consider that CDA are harmful believe that kinking in the ICA, in addition to causing luminal narrowing and endothelial lesions, can create turbulent blood flow that can lead to a prothrombotic state. For others, as Balevi et al., CDA are more a curiosity than a real predictor of ischemic events. 12 Valvano et al. believe that there is no association between CDA and CVD. 50 CDA can cause cerebral hypoperfusion that produces encephalopathy, vertigo, diplopia, TIA or infarction. 40 The prevalence of cerebrovascular symptoms in patients with CDA varies between 15 and 23%. 51 Coiling is not considered a risk factor for ischemic events due to its weak association with symptoms, as opposed to kinking which might be associated with symptoms which most commonly appear due to transitory hypotension during sleep or sudden and extreme movement of the head and neck. 40 Other symptoms observed are visual impairment as amaurosis fugax, uveitis, retinitis and macular dystrophy. 52 Severe cases of CDA can produce mass effect, resulting in dysphagia, dyspnea, upper airway obstruction and obstructive apnea, and, more rarely, pulsatile tinnitus and hemilingual spasm. 40,53,54
In the Northern Manhattan Study (NOMAS), Khasiyev et al. analyzed the relationship between CDA and biomarkers of atherosclerosis in 558 participants and found an association between CDA and diastolic blood pressure and larger aortic root diameter, but not with other markers of atherosclerosis. Determining the risks of vascular events associated with this non-atherosclerotic phenotype may help for a better risk stratification for individuals with CDA. 55
Beigelman et al. investigated the genesis of neurological complications associated with CDA. Sixty patients with CDA without atherosclerosis underwent head rotation tests and color Doppler ultrasound of the ICAs and ophthalmic arteries with evaluation of flow velocities. The results suggested that CDA do not cause neurological abnormalities or symptoms, as no events were recorded during the test, and a significant reduction in the velocities in the ophthalmic artery was observed in only 3 of 60 cases. 56
Wang et al. analyzed the blood pressure changes caused by CDA in 12 patients using DSA. They measured the angle of kinking by rotational angiography and calculated the blood pressure at the proximal, kinking and distal sites of the ICA using a microcatheter. These results were compared with two simulation models. A numerical simulation model was constructed with a software based on a geometric model of a tortuous ICA. An in vitro fluid simulation model was built using a silicone tube with different kinking angles. Water flowed through the silicon tube via a peristaltic pump. The software simulation showed a linear drop in blood flow pressure with decreases in the kinking angle. The pressure drop was the smallest at the kinking angle of 180° and was the largest at 30°. However, a reversal occurred between the kinking angles of 30° and 20°; the increasing kinking degree led to a smaller pressure drop. This was confirmed in the in vitro experimental system. When the flow rate was constant, the pressure drop decreased with increasing kinking angle, but the pressure drop increased when the kinking angle increased from 20° to 30°. However, these findings did not correlate with clinical observations: the clinical tests performed on patients showed greater pressure drops when the kinking angle was < 30°, and severe kinking induced an average decrease of 15.5% in blood pressure. The development of the reversal of greater pressure drops with increased kinking angles from 20° to 30° was not observed in the clinical measurements. This was attributed to excessive elongation and stenosis of the ICA in cases of severe kinking. And although the pressure drop changed gradually in the simulation models, it decreased rapidly in clinical measurements when the angle was < 45º but was more gradual with higher angles. This behavior could be caused by the characteristics of the medium (blood is a non-Newtonian fluid), and the elastic walls of the ICA. Both factors can contribute to the self-regulatory mechanism of blood flow. 57 This was one of the first studies to evaluate these aspects of CDA by comparing clinical and artificial observations with direct measurements of ICA pressures. These results show that blood pressure and blood flow abnormalities may be responsible for the interruption of cerebral perfusion, resulting in ischemia and thus cerebrovascular events.
Some authors observed an association between CDA and aneurysms in the context of CTD. 26 The positive predictive value of the combination of aortic aneurysm and CDA associated with CTD was 95.4% with a specificity of 98.6%. Increased tortuosity index in the aorta and vertebral artery is an independent predictor of aortic dissection in patients with Marfan syndrome. Thus, in patients with CTD, CDA can indicate the presence of clinically significant aneurysms. 6,26,40
Dolichoarteriopathies have been associated with increased morbidity and mortality in head and neck surgery. This risk was recognized in the studies by Weibel and Fields 8 and Metz. 9 Nayak et al. emphasize the importance of evaluating the morphology of the carotid arteries prior to pharyngeal procedures, as they can be complicated by vascular injury, bleeding, and in severe cases, death due to massive hemorrhage. 58 For this reason, it is essential to thoroughly examine the carotid arteries before performing any procedure in the neck.
Treatment
Despite the controversy about the clinical implications of CDAs, some indications have been developed to manage them according to the degree of hemodynamic involvement of the tortuosity, among other parameters. Gavrilenko et al. 59 proposed treating CDAs under the following conditions:
-
ICA stenosis ≥ 60% with atherosclerotic plaques and any degree of cerebrovascular insufficiency; or
-
ICA stenosis < 60% with atherosclerotic plaques, a moderate to severe degree of cerebrovascular insufficiency in combination with tortuosity, a linear blood flow rate ≥ 110 cm/s and a turbulent blood flow.
Grego et al. 60 proposed specific indications for surgery:
-
TIA (hemispheric symptoms);
-
Asymptomatic patients with kink angle < 30°, with contralateral carotid artery occlusion;
-
Patients with non-hemispheric symptoms after a screening to exclude all other possible neurological or non-neurological causes with: 1) Doppler ultrasound positive for significant increase of flow velocity, 2) positive cerebral CT scan or MRA for ischemic lesions in the ipsilateral hemisphere, and 3) reversal of circulatory flow in the anterior cerebral artery and its reduction in the middle cerebral artery, in relation to rotation and cephalic flexion-extension maneuvers.
Other authors have suggested initiating treatment in cases with an ICA-to-common carotid ratio > 2 or a blood flow velocity greater than 180 cm/s. 61,62 However, the actual indication for treating CDA remains controversial. Most authors agree that symptomatic CDA should be treated after excluding other causes.
Invasive techniques have been proposed to correct CDA with successful results (fixation of the ICA to the digastric muscle, end-to-end anastomosis, end-to-side reimplantation, carotid endarterectomy with patch, bypass grafting, and carotid angioplasty with stenting). 40 However, despite the success of these techniques, the appropriate treatment remains controversial. Further studies are needed to determine the real effectiveness of the surgical approach to CDAs.
CONCLUSION
CDA are a common condition with multifactorial etiology and limited, but not negligible, evidence of cerebrovascular involvement. Further studies are needed to determine the usefulness of the therapeutic strategies to improve its prognosis. Strict monitoring and closer follow-up of patients with global assessment of thromboembolic risk are reasonable measures to prevent future events.