Pioderma gangrenoso como diagnóstico diferencial de isquemia crónica crítica de miembros inferiores
Rev Argent Cardiol 2024;92:288-290. http://dx.doi.org/10.7775/rac.v92.i4.20808
Correspondence: Carlos F. Manganiello. Email: cfmanganiello@hotmail.com
MTSAC Miembro Titular de la Sociedad Argentina de Cardiología

Pyoderma gangrenosum is an uncommon ulcerative skin disease, first described 80 years ago, and is classified as neutrophilic dermatosis. (1) Ulcers can occur anywhere on the body, the most common region being the pretibial region. It has no specific serology or histology, and diagnosis is primarily clinical. The ethology is inflammatory and autoimmune (non-infectious). It may occur secondarily to a minor cutaneous (accidental or post-surgical) trauma due to a phenomenon known as pathergy or in association with systemic diseases: inflammatory bowel disease (particularly, ulcerative colitis), and also rheumatoid arthritis, monoclonal gammopathies, or as part of a paraneoplastic syndrome. (2,3)
We present the case of an 87-year-old male patient with a history of arterial hypertension, with a good functional class so far. His disease began 2 months before hospitalization, with low-impact trauma in the anterior region of the right leg. He received antibiotic and analgesic treatment on an outpatient basis, but evolved unfavorably, experiencing painful ulcerative lesions with a necrotic background on the ipsilateral lateral internal and external infrapatellar surface (Figure 1A).
As a result, the patient was hospitalized. Upon admission, he was conscious, and his blood pressure was 130/70 mmHg, his heart rate was irregular reaching 98 beats per minute, temperature was 37.8 °C, and oxygen saturation at room air was 95%. Examination of the right lower limb showed weak positive femoral and popliteal pulse (notably different from contralateral pulse) with good distal foot temperature. Electrocardiogram: atrial fibrillation with moderate ventricular response, and good R wave progression on precordial leads.
Laboratory test: hematocrit 35%, leukocytes: 6300/mm3, platelets: 450,000/mm3, erythrocyte sedimentation rate 100 mm/h, with normal hepatic and renal function, as well as acid-base status. Blood cultures: negative.
Arterial Doppler ultrasound evidenced mild calcific irregularities, triphasic flow in deep and superficial femoral, popliteal monophasic flow, tibial-peroneal, anterior and posterior, and foot trunk, with preserved intima-media thickness.
Surgical toilette and a skin biopsy were performed. Antibiotic treatment, intravenous glucocorticoids and opioids were administered for pain, together with low molecular weight heparin anticoagulation. The patient improved and had no fever. Pain was successfully managed. Analgesia was reduced to non-steroidal anti-inflammatory drugs (NSAIDs), and glucocorticoids and oral anticoagulation were rotated: meprednisone 40 mg and rivaroxaban 20 mg per day.
Laboratory immunology tests: antinuclear factor (ANF), anti-DNA, complement, anti-neutrophil cytoplasmic antibodies (ANCA), and anticardiolipin antibodies were all negative. Skin biopsy: marked polymorphonuclear inflammatory infiltrate, with areas arranged as aseptic abscess. Leukocytoclastic reaction was also evident. Please note that skin biopsy in pyoderma gangrenosum is non-specific and indication aims at excluding other causes of ulceration: infectious (bacterial, fungal) or neoplastic processes. (2,3)
Diagnosis of pyoderma gangrenosum led to continued immunosuppressive (first-line) treatment with meprednisone 1 mg/kg, resulting in very good response, progressive healing of the ulcerative lesion and absence of pain (4) (Figure 1B).
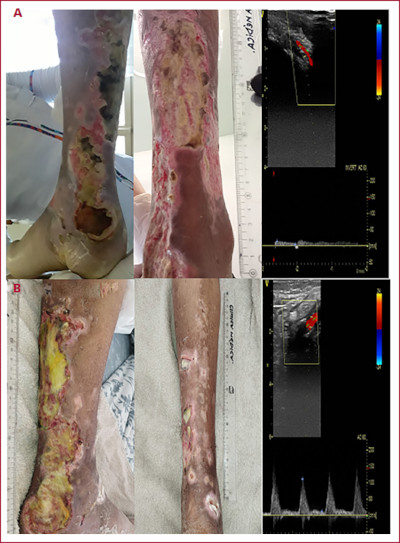
Figure 1.
A. ADMISSION: from left to right: ulcerative lesion upon hospitalization, before and after surgical toilet. Right: Doppler ultrasound with monophasic flow of the anterior tibial artery.
B. POST-TREATMENT: from left to right: granulated and scar tissue after one month of treatment with meprednisone 40 mg/day. Right: Doppler ultrasound with recovered triphasic flow of the anterior tibial artery.
Doppler ultrasound is a non-invasive first-line technique used to evaluate the arterial tree and characterize vascular lesions with an accuracy comparable to angiography. The normal (triphasic) flow pattern may be replaced by a monophasic spectral pattern in various physiological and pathological conditions. The presence of monophasic flow in arteries without any parietal alterations may be due to the presence of distal vasodilation, which can be physiological due to a hyperdynamic state (exercise), or the presence of vascular lesions in soft tissues leading to distal hyperflow. Arteries that appear normal in ultrasonography, but with an impaired vasomotor tone causing monophasic flow, may be undergoing inflammatory-infectious processes, such as erysipelas or cellulitis. In any case, the most common artery condition is parietal atherosclerosis, with significant sites of stenosis creating distal monophasic flow due to reduced distal artery resistance in response to ischemia. (5,6)
In conclusion, the origin of painful lower limb ulcers along arteries is obstructive and vascular, but we need pyoderma gangrenosum as a differential diagnosis, especially in patients with a history of previous trauma or concurrent autoimmune diseases or neoplasms, since treatment for both pathologies is completely different: revascularization is used for arterial stenotic disease, while immunosuppressive treatment is selected for pyoderma gangrenosum (Table 1).
Table 1
Differential diagnosis: arterial ulcer versus pyoderma gangrenosum
BIBLIOGRAFÍA
1. Brunsting LA, Goeckerman WH, O'Leary PA. Pyoderma (Echthyma) Gangrenosum: Clinical and experimental observations in five cases occurring in adults. Arch Derm Syphilol. 1930;22:655-80. https://doi.org/10.1001/archderm.1930.01440160053009
2. Maverakis E, Marzano AV, Le ST, Callen JP, Brüggen MC, Guenova E, et al. Pyoderma gangrenosum. Nat Rev Dis Primers 2020;6:81. https://doi.org/10.1038/s41572-020-0213-x
3. Ferrándiz-Pulido C, García-Patos Briones V. Pioderma gangrenoso. Diagnóstico y tratamiento. Piel. 2008;23:24-9. https://doi.org/10.1016/S0213-9251(08)70969-9
4. Teagle A, Hargest R. Management of pyoderma gangrenosum. J R Soc Med 2014;107:228-36. https://doi.org/10.1177/0141076814534407