
INTRODUCTION
The aorta, the largest artery in the body, serves as an elastic conduit essential for transmitting pressure throughout the arterial bed. This blood vessel, as well as those of medium and small caliber, is susceptible to the development of atherosclerosis due to a combination of acquired, hereditary, sex- and age-related factors. In addition to mechanically obstructing blood flow, the atheromatous plaque poses risks of rupture leading to obstructive or embolic vascular thrombosis. Shaggy aorta (SA) represents an extreme manifestation of aortic atherosclerosis, characterized by extensive and severe atheromatous disease featuring scattered ulcers, soft, loosely held debris, weakened medial arterial layer and tendency towards thrombus formation. (1) While the precise etiology behind the heightened vulnerability of the aorta remains elusive, it is believed to involve complex interactions between hydrodynamic patterns affecting the aorta and genetic predispositions to atherogenesis. (2) The clinical importance of this pathology relies on the various syndromes that can develop from its etiopathogenesis, which generate great morbidity and mortality in affected individuals, and its utility as a risk factor of operative mortality. Furthermore, the advancement of diagnostic tools underscores the importance of multimodality of images in achieving timely and accurate diagnoses, thereby facilitating appropriate decision regarding patient management. Within this context, we present three clinical cases exemplifying the nature of this disease and the spectrum of different syndromes associated with SA. We also highlight the various imaging tools that allowed us to make the diagnosis and its management.
Clinical Cases
Case 1: An 80-year-old female patient was admitted to the emergency room due to 3 days of oppressive, severe, self-limited retrosternal chest pain, associated with palpitations and neurovegetative symptoms, after moderate physical exertion. Medical history included hypertension and dyslipidemia.
On physical examination, the patient was tachycardic with all other vital signs preserved. Cardiac auscultation revealed rhythmic heart sounds of good intensity without murmurs or aggregate sounds. Additionally, no jugular ingurgitation or hepatojugular reflux was found. The electrocardiogram showed sinus rhythm with ST-segment elevation >1 mm and biphasic T waves in leads V1-V4. Laboratory tests revealed troponin I elevation (3.113 ng/mL, normal value <0.028 ng/mL). The patient was admitted with a diagnosis of 3-day evolving anterior Q infarction. During her hospitalization the patient developed chest pain recurrence associated with T-wave inversion in precordial leads V1-V6 and new troponin mobilization; therefore, invasive angiography was performed. During the attempt to cannulate the left coronary artery, with a JL 3. 5 5F catheter, contrast retention was detected in the ascending aorta. CT angiogram showed double lumen at the ascending aorta with presence of dissection flap at the sinotubular junction (without compromising the ostia of the coronary arteries) with ascending trajectory to the proximal aortic arch (Figure 1), and extending through the brachiocephalic trunk to the proximal segment of the subclavian artery (at the level of the humeral head). Diffuse atheromatosis was also observed at the aortic arch with an image suggestive of intraluminal thrombus. A diagnosis of SA, Stanford “A” aortic dissection, brachiocephalic trunk and right subclavian artery dissection was made. Emergency surgical treatment was indicated but unfortunately the patient died during the intervention. Histopathological study of the affected ascending aorta was performed (Figure 2), showing circumferential atheromatosis and the entrance flap of the aortic dissection.
Figure 1
CT angiogram. A, B. Dissection flap is seen at the sinotubular junction (red arrow), with ascending trajectory to the proximal aortic arch (orange arrow) and extending through the brachiocephalic trunk to the proximal segment of the right subclavian artery (white arrows). C, D. Complicated plaques in the aortic arch and descending aorta (green arrows). Diffuse atheromatosis is observed at the aortic arch with an image suggestive of intraluminal thrombus.
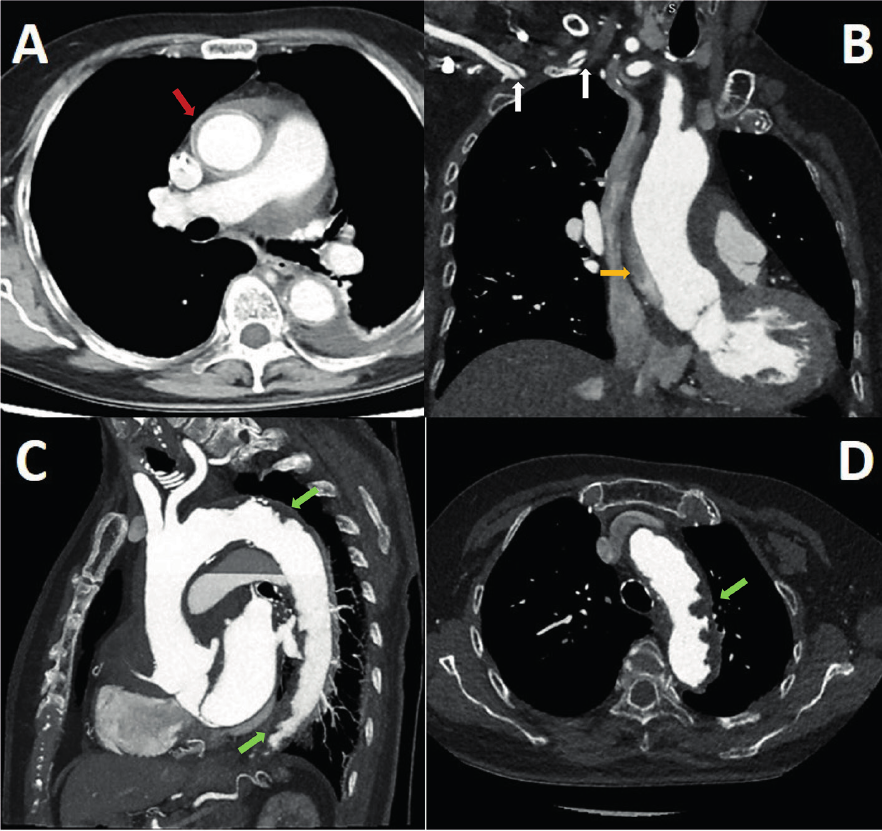
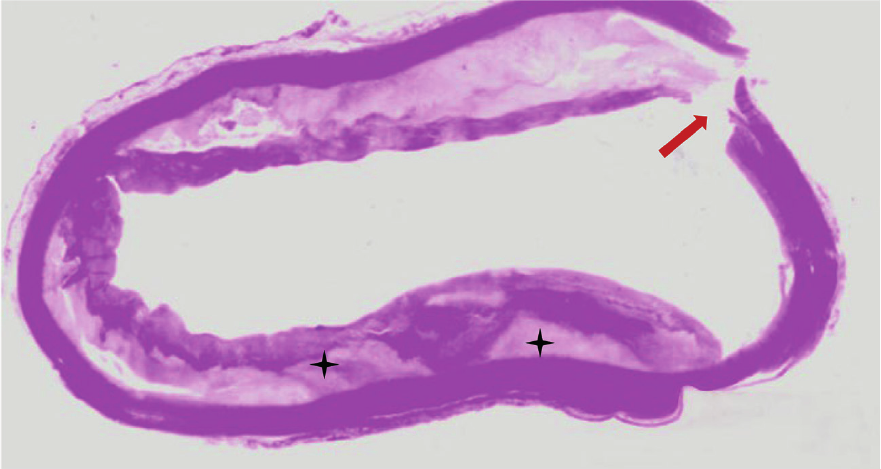
Figure 2
Microscopic view of atheromatous ascending aorta. The patient underwent emergency Bentall de Bono surgery for acute aortic dissection Stanford A; however, she died during the intervention. Circumferential atheromatous plaque in ascending aorta with cholesterol deposits in the subintimal layer (black asterisks). The aortic dissection entry flap can be seen (reddish arrow).
Case 2: A 76-year-old man with a history of arterial hypertension, cigarette smoking, atrial flutter, abdominal aortic aneurysm corrected by bilateral aortofemoral bypass, referred intermittent claudication of the lower limbs, predominantly on the left, when walking less than 100 meters (stage IV according to the Fontaine classification). He was admitted on an outpatient basis for peripheral revascularization.
On physical examination he had preserved vital signs, and thinned, cold, pale lower extremities with trophic changes. On cardiac auscultation heart sounds were arrhythmic, of good intensity, associated with a III/VI holosystolic murmur located in mitral focus, radiating to the axilla. On vascular examination both femoral pulses were preserved; however, popliteal, posterior tibial and pedal arterial pulses were absent bilaterally. The rest of the physical examination was unremarkable. The electrocardiogram showed atrial flutter rhythm, complete left bundle branch block and ventricular premature complexes. The presurgical evaluation was complemented with transesophageal echocardiography (TEE) due to poor acoustic window in the transthoracic approach. The relevant findings were biventricular systolic dysfunction with left ventricular ejection fraction (LVEF) 38%, and right ventricular fractional area change (FAC) 29% due to diffuse global hypokinesia; dilatation of both atria: left atrial volume index (LAVI) 54 ml/m2 and right atrial (RA) area 20 cm2; and severe mitral insufficiency: effective regurgitant orifice area (EROA) 0.4 cm2, regurgitant volume (RV) 65 ml and regurgitant fraction (RF) 68%. Likewise, evaluation of the aorta showed multiple complex atheromatous plaques distributed circumferentially and extending from the aortic arch to the descending aorta (Figure 3). Computed tomography aortic angiogram showed multiple ulcerated atheroma plaques arranged in tandem along the entire course of the aortic arch and descending aorta, associated with low-attenuation images suggestive of thrombi (Figure 4). The common iliac arteries presented multiple internal and external calcified plaques that conditioned severe stenosis predominantly on the left and permeable aortofemoral bypass.
Figure. 3
A. After rupture of the fibrous cap, coagulation molecules from the bloodstream come into contact with foam cells, tissue factor, and microparticles derived from apoptotic atheroma cells, triggering thrombus formation in the ruptured plaque. The thrombotic equilibrium will determine whether plaque rupture will culminate in the formation of a persistent, distant-migrating thrombus or in its dissolution. B. TEE - Proximal third of the descending aorta. Orthogonal images showing extensive mural thrombotic formation of irregular border that occupies up to one third of the arterial lumen, with small movable elements on its surface in the long axis. C. TEE - Middle third of the descending aorta. Orthogonal images showing crescent-shaped thrombus in the short-axis view. D. TEE - Distal third of the descending aorta. Orthogonal images of wedge-shaped thrombus. Secondary thrombotic elements in opposite position to the initial one.
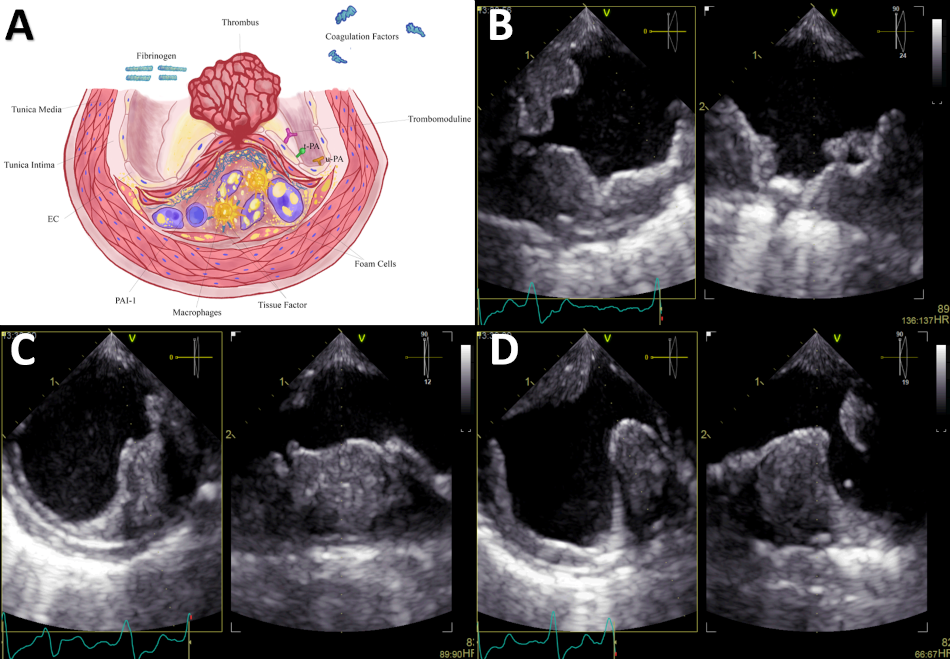
EC: endothelial cell; PAI-1: type 1 plasminogen activator inhibitor; TEE: transesophageal echocardiography; t-PA: tissue-type plasminogen activator; u-PA: urokinase-type plasminogen activator.
Figure 4
A. CT angiogram - Sagittal section of the aorta. Multiple atheromatous plaques, in tandem, along the entire course of the aortic arch and thoracoabdominal aorta (red arrows), predominantly in the supradiaphragmatic portion. B. Longitudinal reconstruction of the aorta. The cross section shows plaques with low attenuation coefficient (35 HU), irregular borders (lower central box), ulcerated and associated with images suggestive of thrombus (lower right box).
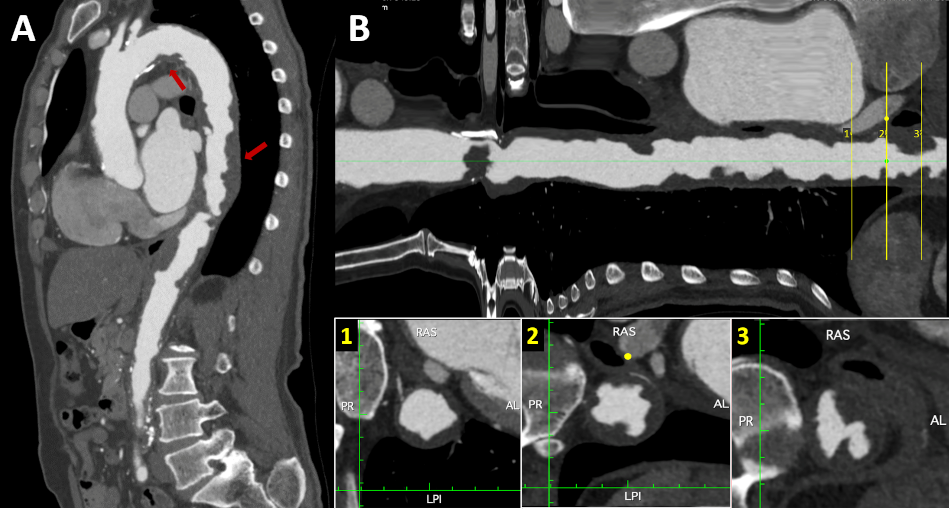
AL: anterior and left; CT: computed tomography; HU: Hounsfield units;; LPI: left posterior and inferior; PR: posterior and right; RAS: right anterior and superior.
Because of these findings, coronary revascularization and mitral valve replacement with subsequent peripheral revascularization was decided. However, the patient did not tolerate the cardiac surgery and died during the procedure.
Case 3: An 84-year-old male patient was admitted at the emergency room with acute diarrhea associated with severe diffuse abdominal pain. Medical history included hypertension, diabetes mellitus, chronic kidney disease and senile dementia.
Physical examination revealed tachycardia, pale, earthy skin, sweating and capillary refill time >2 sec. Cardiac sounds were rhythmic and tachycardic; no murmurs were identified. On pulmonary auscultation, the vesicular murmur was preserved in both lung fields. Laboratory tests showed severe anemia (Hb: 6.9 mg/dL), leukocytosis with left shift, elevated azotemia (creatinine 3.11 mg/dL, urea 134 mg/dL) and hyperlactacidemia. A thoracoabdominal computed tomography (CT) angiography was requested, revealing a SA with severe parietal calcification associated with an abdominal aortic aneurysm of up to 85 mm, with presence of mural thrombosis (Figure 5). Mesenteric ischemia was suspected, with emboligenic source coming from complex atheromatous aortic plaques or abdominal aortic aneurysm. The patient was admitted to the operating room for an exploratory laparotomy. However, he died during the operative procedure.
Figure 5
A. Non-contrast thoracoabdominal CT - Coronal section. Severe calcification of the aorta is observed, predominantly in the aortic arch and abdominal aorta. Also, there is an aneurysmal dilatation of the infrarenal aorta with a maximum diameter of up to 8.5 cm. B. Longitudinal reconstruction of the aorta. The transverse sections at the level of the abdominal aortic aneurysm demonstrate the calcification of the abdominal aneurysm wall along with the presence of extensive mural thrombus (red arrows) and a reduced luminal diameter (orange star).
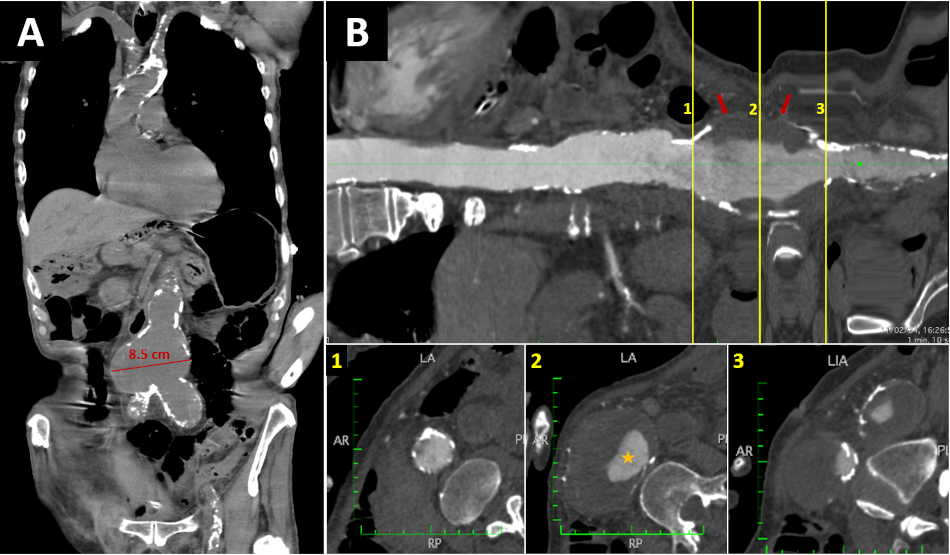
AR: anterior and right; CT: computed tomography; LA: left and anterior; PI: posterior and inferior; RP: right and posterior.
DISCUSSION
Definition
A uniform definition of SA has not been clearly established due to the different diagnostic methods used. However, some definitions have been postulated. SA is a descriptive term that has been used for atherosclerotic aortic segments, which show localized or diffuse irregularity and typical obstructive and spiculated images that are visualized with different diagnostic tools. The shagginess is imparted by complications in the form of multifocal ulcerations, calcification, and/or overlying thrombi. (3) Another definition used for the SA is the appearance of a hemp-like fluff on the inner surface of the aorta due to severe diffuse atherosclerotic lesions in the aorta. Clinically, it is often referred to an imaging finding of contrast-enhanced CT or echography. (1)
Epidemiology and pathophysiology
The prevalence and incidence of SA in the general population is unknown. However, there are some reports on the prevalence and incidence of SA in certain risk groups. Thus, in one study it was found that 48/447 patients (11%) having elective aortic abdominal aneurysm repair had SA. Also, the incidence of major complications and mortality was 4.1 times higher in patients with SA than in patients without severe atherosclerotic aorta. (4) In another study, it was reported that the prevalence of SA in patients undergoing total aortic arch replacement was 19 %. (5) Likewise, it has been seen that most of the patients with SA are elderly, predominantly males with comorbid conditions like hypertension, diabetes mellitus, chronic obstructive pulmonary disease, coronary and peripheral artery disease, and stroke. (3)
Severe atherosclerotic degeneration of the aorta is a multifactorial process in which various modifiable and of the organism itself (non-modifiable) risk factors intervene. The initial event that gives rise to atheroma formation is unknown; however, the "response to injury" hypothesis considers atherosclerosis as a chronic response of inflammation and scarring in the arterial wall after endothelial injury with subsequent evolution of the atheroma due to the interaction of modified lipoproteins, the immune system and the smooth muscle cells of the arterial wall. (6)
After accumulation of lipoprotein particles in the subintimal space and their binding to proteoglycans, these particles are affected by oxidative stress (oxidation and glycation). These modified lipoproteins induce the synthesis of cytokines that promote chemotaxis of inflammatory cells (monocytes, T lymphocytes), phagocytizing this material. These macrophages (foam cells) are a source of new mediators that favor the migration of smooth muscle cells toward the intima, which are responsible for the elaboration of the extracellular matrix that accumulates within the atherosclerotic plaque (allowing its growth). (2)
The spatial heterogeneity of atherosclerotic lesions in patients with SA has been difficult to explain. It is believed that this is not only the result of a response to the different hydrodynamic patterns that affect the aorta (normal pulsatile lamellar flow generates greater shear force that is associated with lower atherogenicity), but also of a genetic predisposition specific to the individual. Thus, those with higher expression of genes encoding for the enzymes superoxide dismutase, nitric oxide synthase and Kruppel-type factor 2 are less predisposed to severe atherosclerotic degeneration, by reducing the formation of oxygen free radicals, inhibiting proinflammatory nuclear factor-kappa B (NF-kB) and favoring vasodilatation. (2)
Diagnostic implications
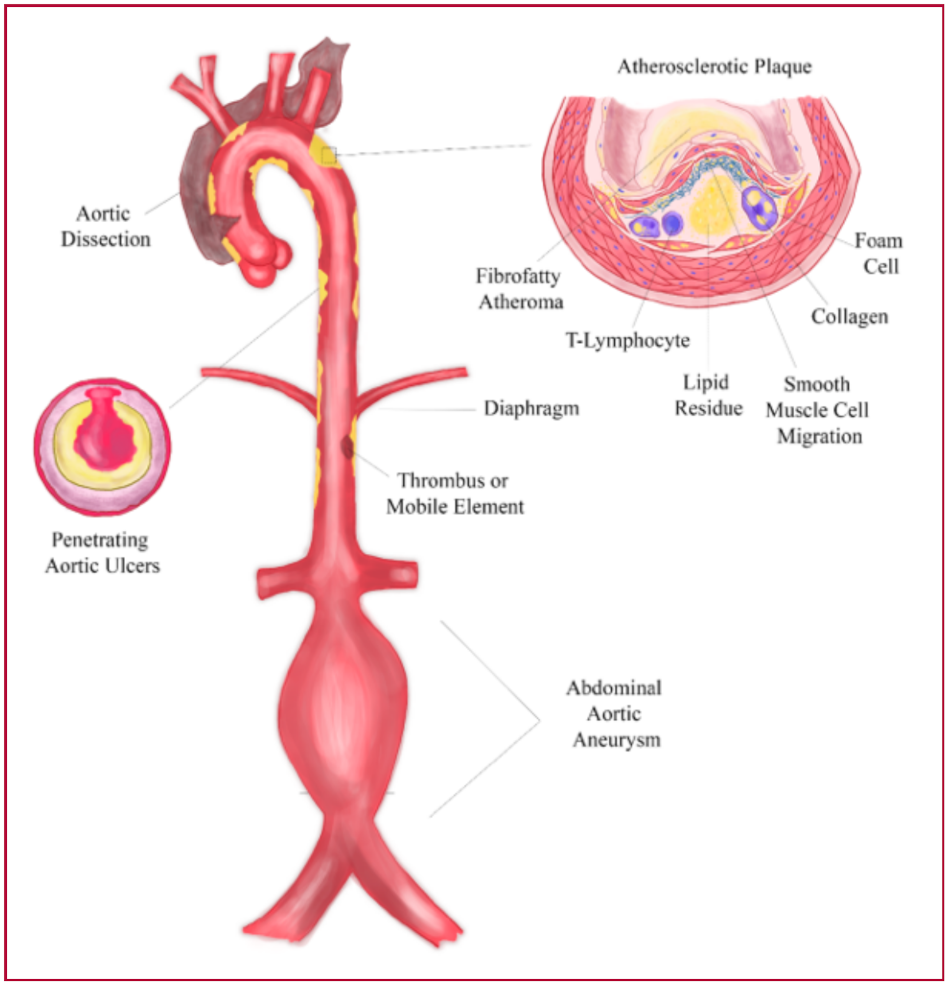
The clinical importance of this pathology lies in the various syndromes that can develop from its etiopathogenesis, which generate great morbidity and mortality in affected individuals. The presence of severe atherosclerotic degeneration in the aorta will be associated with an increased risk of developing aortic aneurysms, aortic dissection, thromboembolism or peripheral atheromatous embolization (to the digestive system, renal, spinal cord or peripheral limbs manifested as SA syndrome), ischemic stroke and penetrating atherosclerotic ulcer (CENTRAL ILLUSTRATION). (7) Similarly, SA is an independent and significant risk factor for operative mortality.
CENTRAL ILLUSTRATION
Shaggy aorta is characterized by severe atherosclerotic degeneration, resulting from a multifactorial pathophysiological process (with chronic inflammation, ischemia, aortic wall shear stress, and individual genetic susceptibility being fundamental to parietal remodeling and increased vulnerability). The clinical importance of this disease lies in the different clinical conditions to which it predisposes (aortic dissection, penetrating aortic ulcer, aneurysmal dilatation and systemic embolization) and in its role as an independent and significant risk factor for operative mortality.
The predisposition for the development of aneurysms and aortic dissection has a multifactorial basis involving chronic inflammation and ischemia of the aortic wall, which generates remodeling and increased susceptibility. The presence of severe atherosclerosis is associated with increased local expression of proteinases that contribute to tissue destruction, cell necrosis and apoptosis. (8, 9) On the other hand, the blood supply of the aorta is provided by simple diffusion (2/3 internal) and through the vasa vasorum (1/3 external), except for the infrarenal aorta, which lacks an independent vascular supply; (10) therefore, the presence of atheromas favors ischemia of the media with subsequent apoptosis of smooth muscle cells and weakening of the wall. (11) This phenomenon, together with a simultaneous stressful stimulus, which exceeds the strength of the aortic wall, increases susceptibility to the development of aneurysms and/or aortic dissection.
Another of the syndromes associated with SA is embolism, central or peripheral, of thrombi or cholesterol crystals. Plaque stability will be the result of the balance between mechanical resistance and the forces that affect the coating. Thus, unstable plaques will be characterized by the presence of a thin fibrous plaque, with few smooth muscle cells, covering a large lipid core with abundant foam cells and tissue factor. (12) Fracture of the sheath will expose the atheroma tissue factor to blood clotting proteins, thus initiating the coagulation cascade and the formation of fibrin-rich thrombi (Figure 4), which embolize to the brain or peripheral organs. Likewise, the exposure of cholesterol crystals, contained within the lipid core, can be embolized to the peripheral organs or extremities giving rise to a SA syndrome (diffuse atheromatous embolization). (13)
Penetrating atherosclerotic ulcers (PAU) are caused by ulceration of the atherosclerotic plaque with extension into the media producing a mushroom-shaped excrescence. They occur as unifocal or multifocal lesions in diffusely atherosclerotic aortas, particularly in the mid-portion and distal third of the descending aorta. Its timely diagnosis is essential as large PAU (>20 mm), with a depth greater than 10 mm, are responsible for 2-7% of cases of acute aortic syndrome. (3, 14)
Diagnosis and multimodality
When evaluating aortic pathology, the method of choice will depend on the diagnostic suspicion, the patient's comorbidities and the availability of the method. These include transthoracic echocardiography (TTE), TEE, CT and magnetic resonance imaging (MRI). Generally, more than one diagnostic tool will be used, emphasizing the importance of multimodality for proper diagnosis, and its choice will depend on the individualization of each case.
TTE allows visualization of the aortic root, sinotubular junction (STJ), ascending aorta (AAo), distal portion of the aortic arch and proximal portion of the descending aorta (DAo). However, it is limited by the acoustic window of each patient. On the other hand, TEE allows visualization, with higher spatial resolution, of the AAo, the arch and the thoracic DAo, with the exception of a "blind spot" located at the junction of the AAo and the aortic arch. (15) The higher spatial resolution is due to the proximity of the esophageal transducer to the aorta and the higher wave frequency. For this reason, TEE is the imaging modality of choice to diagnose plaques in the thoracic aorta and to specify its morpho-structural characteristics. (15) Thus, the aortic plaque is defined as an irregular thickening of at least 2 mm with increased echogenicity with respect to the adjacent intimal surface. A complex aortic plaque, defined by a thickness ≥4 mm, ulcerated or with associated mobile component, is associated with increased risk of cardiovascular and cerebrovascular events and mortality. (16)
CT makes it possible to visualize the aorta in its entirety, detect calcified plaques, tortuosity, aneurysm and evaluate adjacent organs. The visualization of the lumen requires the use of contrast media, which can accurately define the aortic wall, perform precise measurements, identify and characterize aortic plaques, as well as their complications (endoluminal thrombi and the different forms of acute aortic syndrome). (16) Therefore, when acute aortic syndrome is suspected, it is considered the first diagnostic study, as long as it is contrasted and triggered. Its main limitations lie in the use of radiation and iodinated contrast.
MRI perfectly characterizes the composition of the aortic plaque (fibrous cap and lipid core) and identifies thrombi attached to the plaque. (17) Its diagnostic capability is superior to TEE, particularly in the AAo and aortic arch; nonetheless, TEE has a better image quality regarding the DAo. (18) In addition, it allows assessment of cardiac and valvular function, information that is of interest in aortic pathology. Despite these advantages, its high cost, limited availability, longer acquisition time and occasional use of contrast, make it an ineligible method for diagnosis and follow-up.
Management
Although there is no clear indication for endovascular aortic treatment of the abdominal or thoracic aorta in patients with SA, we know that these patients are at increased risk for embolization and development of acute and chronic aortic complications. Evidence suggests that ''prophylactic'' endarterectomy of a severely atherosclerotic aorta for protruding atheroma as an adjunct to a cardiac procedure is not recommended because of the high incidence of intraoperative stroke. (19) Nevertheless, patients with recurrent peripheral or visceral embolization and presence of SA with favorable anatomical features for endovascular reperfusion may undergo such treatment (Recommendation Class IIb, Level of Evidence C). (20) On the other hand, the management of complications associated with SA are beyond the scope of this review.
CONCLUSIONS
SA refers to severe atherosclerotic degeneration of the aortic surface, which is extremely friable and predisposes to various complications such as aneurysms, acute aortic syndromes, and peripheral embolization. The incidence and prevalence of SA in the world population is unknown but is estimated at 10-20%. The fundamental bases for the development of SA and its complications are chronic inflammation, ischemia, aortic wall shear stress and individual genetic susceptibility. On the other hand, multimodality imaging is essential for the timely and correct identification and characterization of aortic atherosclerotic plaques, especially complex ones, which are typical of SA. Each of these diagnostic tools has certain characteristics that favor or limit their usefulness. Finally, there is no consensus regarding the interventional or surgical management of SA, but its finding constitutes an important risk factor for operative and long-term mortality.
Conflicts of interest
None declared. (See authors' conflict of interests forms on the web).
Financing
None