ORIGINAL ARTICLE
Endovascular Treatment of Aneurysms with Complex
Aortic Anatomy
Tratamiento
endovascular de aneurismas con anatomía aórtica
compleja
L. Mariano Ferreira1,
MTSAC, Miguel Ferrer1,
Leonela Aloy1, A. Ricardo La Mura1
1
Division of Vascular Surgery.
Clinica La Sagrada Familia. Autonomous City of Buenos Aires.
Address for correspondence: L. Mariano Ferreira. Av.
del Libertador 5878 4ª. CABA C1428ACQ
Rev Argent Cardiol 2023;91:267-272. http://dx.doi.org/10.7775/rac.v91.i4.20561
ABSTRACT
Background: Arterial anatomy is the main limiting factor for
standard endovascular aortic (EVAR) approach. We present our experience for
endovascular repair of complex aortic aneurysms.
Methods: This is a retrospective observational study in patients with complex
aneurysms (juxta/pararenal
and thoracoabdominal) treated consecutively with:
fenestrated (FEVAR), branched (BEVAR), EndoAnchors
(ESAR), or chimney (ChEVAR) stents. The decision of
the technique was determined based on the arterial anatomy.
Results: The last 50 procedures were evaluated (6 women; mean age 71.3 years;
diameter 69.6 mm; and 3 patients with complicated aneurysms), among whom 22
received FEVAR (2.8 fenestrated stents/patient), 11 BEVAR, 11 ESAR and 6 ChEVAR (1.8 chimney stents/patient). Technical success rate
was 100% (absence of type I or III endoleak with
adequate patency of the visceral vessels). Three patients died within the first
30 days (6%). During follow-up, 5 patients presented with renal artery
occlusion, treated successfully in 4 cases. Four patients developed type IA endoleak (3 secondary ESAR and one ChEVAR),
one patient IC endoleak and almost a quarter of cases
type IIIB endoleak (22%, 3 out of 11 patients
receiving ESAR, none of the industrial FEVAR group). Overall survival was 88.6%
at one year, and 86.5% of cases were free from reoperation.
Conclusions: This is the first publication in our setting that
shows a global approach to the patient with complex aortic aneurysm, according
to the anatomical characteristics. These technologies already play a primary
role in the treatment of these patients.
Keywords: Abdominal Aortic Aneurysm - Endovascular repair - Device modification
- Durability Long-term follow-up - Thoracoabdominal
aneurysms - Juxtarenal aneurysms - Complex Aorta
RESUMEN
Introducción:
la anatomía arterial es la principal limitante para el abordaje aórtico endovascular estándar. Presentamos nuestra experiencia para
la reparación endovascular de aneurismas aórticos
complejos.
Material
y métodos: estudio observacional retrospectivo en
pacientes con aneurismas complejos (yuxta/pararrenales y toracoabdominales)
tratados en forma consecutiva mediante: endoprótesis fenestradas (FEVAR), ramificadas (BEVAR), con EndoAnchors (ESAR), o en chimenea (ChEVAR).
La decisión de la técnica fue determinada con base en la anatomía arterial.
Resultados:
se evaluaron los últimos 50 procedimientos (6 mujeres; edad promedio 71,3 años;
diámetro 69,6mm; 3 pacientes con aneurismas complicados), de los cuales 22 recibieron
FEVAR (2,8 fenestraciones / paciente), 11 BEVAR, 11
ESAR y 6 ChEVAR (1,8 chimeneas /paciente). La tasa de
éxito técnico fue del 100% (ausencia de endoleak I o
III con permeabilidad adecuada de los vasos viscerales). A 30 días 3 pacientes
fallecieron (6%). Durante el seguimiento, 5 pacientes presentaron oclusión de
la arteria renal, repermeabilizada en 4. Cuatro
pacientes desarrollaron un endoleak tipo IA (3 ESAR
secundarios y un ChEVAR), un paciente un endoleak IC y un cuarto uno IIIB (22%, 3 de los 11 ESAR,
ninguno de los FEVAR industriales). En el análisis de supervivencia, la
supervivencia global fue del 88,6% al año, y libre de reoperación
del 86,5%.
Conclusiones:
se trata de la primera publicación en nuestro medio que muestra un enfoque
global del paciente con un aneurisma de aorta complejo, de acuerdo con sus
características anatómicas. Estas tecnologías ya desempeñan un papel primario
en el tratamiento de estos pacientes.
Palabras
clave: Aneurisma de Aorta Abdominal -
Tratamiento Endovascular - Modificar dispositivo -
Durabilidad Seguimiento a largo plazo - Aneurismas toracoabdominales
- Aneurismas Yuxtarrenales - Aorta Compleja
Received: 05/12/2023
Accepted: 06/15/2023
INTRODUCTION
More than 80% of infrarenal
abdominal aortic aneurysms with an indication for treatment are currently
excluded using an endovascular approach. (1) For this purpose, two technical alternatives have
been developed: standard and complex techniques. The arterial anatomy,
especially that corresponding to the visceral segment of the aorta, is the
decisive factor. Endovascular repair must be sealed in a healthy aorta to
provide a durable repair. Therefore, when the aneurysm has a healthy segment
for infrarenal sealing, a standard approach is used,
which is accompanied by a low complication rate. (2-3)
On the contrary, the development of endovascular
methods for patients with visceral aortic involvement has brought about a
radical change. The complex approach, indicated when
the sealing zone compromises or is in contact with the segment of the aorta
from which the mesenteric or renal arteries emerge, implies the use of devices
that make it possible to respect the origin of these arteries. It is especially
in these procedures where the results are specifically related to an advanced
diagnostic and therapeutic algorithm. We present our experience with a global
technical approach (therapeutic algorithm) in endovascular repair of patients
with complex aortic aneurysms.
METHODS
Patient Selection
This is a retrospective observational study that
evaluated the 30-day and 3-year outcome in patients with complex aneurysms
treated using an endovascular approach to place fenestrated (Fenestrated
Endovascular Aneurysm Repair, FEVAR) or branched (Branched Endovascular
Aneurysm Repair, BEVAR) endografts, standard endografts reinforced with EndoAnchors
(EndoSuture Aneurysm Repair, ESAR), or standard endografts with parallel or chimney stents to preserve the
visceral arteries (Chimney Endovascular Aneurysm Repair, ChE-VAR).
The decision of the technique was determined based fundamentally on arterial
anatomy. Emergency patients were excluded.
Definitions and End Points
Aortic aneurysm with complex anatomy is a juxtarenal, pararenal, paravisceral, or thoracoabdominal
aortic aneurysm (TAAA), which, per instructions for use of a standard
endovascular graft, is not a candidate for exclusion by placement of only a
standard infrarenal bifurcated endograft
(EVAR).
Three fundamental algorithms have been used for the
diagnosis and treatment of these patients.
Patients were evaluated by CT angiography with
intravenous injection of contrast, except in those with creatinine
clearance less than 30 ml/min, in whom the intra-arterial route with an aortic
catheter was preferred to reduce the amount of contrast injected (less than 60
ml for thoracoabdominal studies).Various imaging
tools were also used during surgery to reduce the amount of contrast and radiation:
image fusion (Vessel Navigator, Azurion/Allura Xper FD20, Philips
Healthcare), intraoperative cone beam tomography (Xpert-CT,
Philips) and intravascular ultrasound (IVUS Vulcano,
Philips).
Patients were evaluated with CT angiography before
discharge to verify aneurysm exclusion, device integrity, and aortic collateral
vessel patency. Doppler and CT scan without contrast were performed only in
those with renal failure. In the absence of endoleak,
follow-up controls were performed by CT angiography and Doppler at 6 and 12
months and then annually, whereas in the presence of endoleak,
follow-up was carried out according to the type of endoleak,
characteristics of the patient and behavior of the aneurysmal sac.
Therapeutic algorithm
FEVAR includes a series of aortic devices that can be
custom-made by a technology manufacturer (Custom Made Devices, CMD, Cook
Medical, Bloomington, Ind)
or by a physician in the operating room (Physician Modified Stent Graft, PMSG).
Fenestrations are holes in the prosthetic material of the device that
correspond to a visceral aortic branch (celiac trunk, superior mesenteric, or
renal arteries), thus allowing the graft to lie more proximally than a standard
configuration would admit. The orifice/fenestration of the endograft
is then made to coincide with the origin of the artery to be preserved. To seal
and specifically anchor the fenestration, stents are placed inside it towards
the preserved artery. FEVAR was indicated in patients with a short infrarenal neck, less than 5mm in length, and visceral
aortic diameter less than 36 mm. (Fig.
1)
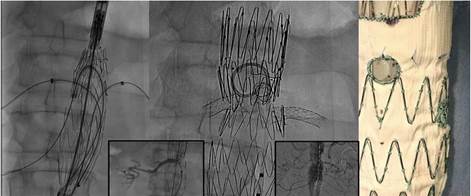
Fig.
1. From left to right.
Angiographic image showing fenestrated endograft in
position with introducers and guidewires placed in
the renal and superior mesenteric arteries. Bottom left: Cannulation
of the right renal artery. Middle: Fenestrated endograft
(FEVAR) with deployed stents in the renal and mesenteric arteries. Bottom
right: Final angiography. Right: Photograph of fenestrated endograft
manufactured in the operation room with a central fenestration for the superior
mesenteric artery.
BEVAR. Standard branched graft (Zenith t-BRANCH, Cook
Medical, Denmark) consists of a tubular endograft
with four caudal branches, located in the standard longitudinal and axial axes,
based on CT files of patients with thoracoabdominal
aneurysms. It also requires an additional stent, a bridge, to connect and seal
the stent branch with the visceral vessel. It was indicated in patients with
type IV thoracoabdominal aneurysms (Fig. 2).
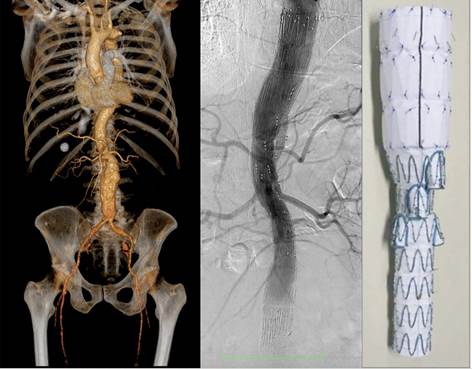
Fig.
2. Left: Computed tomography angiography of a patient
with juxta-visceral aneurysm. Center: Final
angiography with branched endograft towards the
celiac trunk, the superior mesenteric artery and both renal arteries. Right: Protograph of the branched endograft.
ESAR. EndoAnchors (Heli-FX™ EndoAnchor™ system,
Medtronic Inc, Minneapolis, USA), are endosutures that reinforce the contact between the endograft and the arterial wall at the neck level. The
procedure involves the endovascular screwing of small helical clips, simulating
the force of a hand-sewn surgical anastomosis. This approach was used in
patients with the possibility of a correct apposition (contact) between the endograft and the infrarenal
aorta of at least 10 mm, but with a neck over 30 mm in diameter, and conical, teardropor hourglass-shaped necks, all tomographic
characteristics that are associated with an increased risk of mid-term dilation
of the proximal neck. It was also used in previously operated patients, with
growth of the aneurysmal sac due to type II endoleak
and neck dilation of more than 10% or more than 32 mm in diameter.
CHEVAR. Chimney stents ensure inflow through a covered stent
placed in the visceral branch parallel to the endograft.
It was indicated in patients with a short neck, 5 to 10 mm but less than 28 mm
in diameter, especially in high-risk patients not only for aneurysm rupture
(pain or more than 70 mm) but also at high surgical risk (ASA IV).
Statistical analysis
Continuous data are presented as mean and standard
deviation (SD) and categorical data as percentages. Continuous data were
compared using Student’s t-test or Wilcoxon’s test according to their
distribution. Paired data tests were used to compare the dimensions before and
after the intervention. Categorical data were compared with the chi-square test
or Fisher's exact test, as appropriate. Event-free survival was defined by
survival analysis, with the creation of Kaplan Meier curves. Statistical
analysis was performed using SPSS 25.0 software for Windows. (SPSS, Inc.,
Chicago, IL).
RESULTS
The last 50 patients who underwent endovascular
procedures for complex aortic disease, were consecutively evaluated; 44 were
men (88%) and 3 (6%) had complications at the time of presentation (symptomatic
or ruptured and contained aneurysm).
Mean age was 71.3 ± 11.6 years, and mean aneurysmal diameter was 69.6 ±
16.6 mm (FEVAR 68.5 mm, BEVAR 66.4 mm, ESAR 72.3 mm, and ChEVAR
79, 8 mm p=0.418). Twelve patients (24%) presented with a previous EVAR. In
this subgroup, the indication for treatment was due to type IA endoleak (n=4, 33.3%), migration (n=2, 16.7%), and proximal
neck dilation (n=6, 50%).
Procedures performed included: 22 FEVAR (17 PMSG and 5
CMD), 11 BEVAR, 6 ChEVAR, and 11 ESAR.
Technical success rate was 100% without the presence
of type I or III endoleak, with adequate branch
patency. Three patients died during the first 30 perioperative days, one in the
immediate postoperative period due to mesenteric atheroembolism
(BEVAR), a second patient on day 22 due to pneumonia (patient with ruptured and
contained aneurysm) and another due to ventricular tachycardia on day 8, the
last two deaths secondary to ChEVAR.
Complications during follow-up
During an average follow-up of 17 months (range 1-48
months), four patients presented with type IA endoleak,
three of whom received a FEVAR (all with a prior secondary ESAR, treated during
follow-up for proximal neck dilation), and a fourth, with a previous ChEVAR, which was corrected by gutter embolization and EndoAnchors placement.
Renal artery occlusion occurred in five patients (3
BEVAR and 2 PMSG). Three were corrected, a fourth high-risk patient remained
asymptomatic without treatment and the fifth patient presented renal artery
occlusion in an already atrophic kidney, so he also received no treatment.
In the Kaplan-Meier analysis, overall survival was
88.6% at 1 year and 77.3% at 3 years; 86.5% of cases were free of reoperation
at 1 year and 61.3% at 3 years, while primary vessel patency was 91.3% at one
year and 79.9% at three years.
Behavior of the aneurysmal sac
Overall, the aneurysmal sac underwent a
non-significant reduction from 68.3 mm±15.6 mm to 66.9 mm±17.6 mm (p=0.69).
However, knowing the small number of patients in the series, the tomographic
information was disaggregated by procedure. Patients with BEVAR developed sac
narrowing from 64.9 mm±8.12mm to 59 mm±8.2mm (p=0.14) and those with FEVAR from
60.17 mm±11.1 mm to 54.17 mm±9.9 mm (p= 0.31). Specifically, aneurysmal sac
enlargements developed in type IA endoleak patients
who were repaired and three in type II endoleak
patients currently under observation.
DISCUSSION
This series shows the experience of a center
specialized in the treatment of patients with aortic aneurysms. Supported by a
selection based on anatomical and clinical-surgical criteria, it is the first
publication in our setting that shows a global approach to the patient with
complex aortic aneurysm. The application of a well-established protocol made it
possible to treat this group of patients at high surgical risk, even during the
pandemic, with a perioperative morbidity and mortality rate similar to
international standards.
It is estimated that 50% of patients with abdominal
aortic aneurysms are not candidates for endovascular repair with the devices
currently available on the market due to their unfavorable anatomy. (4) This includes patients with short or angled necks,
aneurysmal extension to the internal iliac artery, or aneurysmatic
involvement of the juxtarenal, paravisceral,
and thoracoabdominal aorta (complex aorta). Good
surgical candidates can tolerate conventional open surgery.(5,6) However, in a recent presentation at the Charing Cross International Symposium in London on April
27, 2023, the surgical team from the University of Brescia, after matching
covariates from 204 patients with thoracoabdominal
aneurysms, determined that 30-day mortality after open surgery was 13% vs. 5%
for complex endovascular treatment; paraplegia was 10% vs. 3%, severe
respiratory complications 18% vs. 7%, cardiac complications 42% vs. 26% and
severe renal 27% vs. 6% for endovascular treatment. This shows a real world
with current statistics, advanced technology and a surgical team with
experience in both approaches.
Complex endovascular aortic techniques were designed
to extend the proximal sealing zone from the infrarenal
segment to the juxta or suprarenal aorta, thus
avoiding the limitation of the absence or short length of the infrarenal aortic segment. From the moment we started in
2011 the first option for these patients has been and remains the placement of
a fenestrated endograft (FEVAR). Since then,
evolution has meant better patient selection, innovative changes in endograft design, significant developments in imaging
technology, and the application of standardized protocols for perioperative
care. It is clear that care for these patients does not begin or end in the
operating room; hence the importance of multidisciplinary care, on which the
overall success of the procedure depends. Fenestrated grafts specifically need
to be custom assembled. Arterial anatomy is unique for each patient, and
precise contact between graft orifice and the origin of the artery to be
preserved is required. That information is obtained from the CT scan and must
be transferred to a design to build the endograft.
The industrial production of these devices (Cook Medical in our case) implies a
certain delay in their availability (authorization time, production, and
transfer) that may be too long for patients with urgent needs (aneurysms of
more than 7 cm, symptomatic or ruptured). The way to respond to this problem
was to train in endograft manufacturing, but
fenestrated in the operating room, which has the enormous advantage of the
almost immediate availability of a custommade endograft. (7) For
this purpose, two members of the team were trained at the Mayo Clinic
(Rochester, Minnesota). This allowed us to design these endografts
with variables such as number, location, and fenestration size or to design
them to be cannulated for a femoral or subclavian approach. Thus, we can access from the cranium
to caudally oriented vessels, and also avoid placing a bulky introducer in a
femoral artery, which could cause limb ischemia. (8) However, published evidence and our own experience
determine that this type of endografts modified in
the operating room should be indicated in exceptional cases. The study
presented by Dr. Oderich of the Mayo Clinic
determined that the current approach has evolved from devices built in the
operating room to almost exclusively company manufactured devices (CMD). These
have been manufactured with greater technical success, with no mortality and
with fewer serious adverse events. (9) In our series, none of the patients who received a
CMD developed complications.
It is also important to emphasize the strict followup that these patients require. As shown in the
results section, this approach is accompanied by a not negligible rate of
reoperations: almost 10% of patients received a second procedure due to branch
instability (occlusion or endoleak). But, most were
minor surgeries and did not affect survival. (10-13)
A goal of the division was also to try to decrease the
need for FEVAR in a specific group of patients.
Patients with proximal necks excluded from the
instructions for use, but in whom the CT scan analysis allowed us to predict
that we had a contact zone of 10 mm, were not treated with FEVAR as the first
option. (14) The experience obtained with EndoAnchors
allowed us an adequate seal, with no mid-term mortality or type IA endoleak, when EndoAnchors were
implanted in the primary procedure. Same as in the ANCHOR registry, these
results remain promising.
(15) On the other hand, when they were placed before a proximal neck dilation, in some cases, the consequent
dilation ended in a proximal endoleak, which had to
be repaired by FEVAR.
ChEVAR was relegated to a strict anatomical and clinical
indication. We are aware of the higher incidence of type IA endoleak
associated with this technique, and for this reason we are very selective in
its use. (16)
Finally, BEVAR was not performed in the context of
dilated necks but in those evidently aneurysmal, juxta/pararenal aneurysms, where the dilated visceral aorta
implied more than 5 mm of distance between the endograft
and the origin of the visceral artery. (17) Spinal cord ischemia is a devastating complication,
with a known association between its incidence and mortality. (18) In 2019, we published our protocol for its
prevention, analyzing 29 patients. (19) Since then, we have had no
cases of early or late paraplegia.
Although current international guidelines do not
directly translate into recommendations for complex treatment, it is logical
and reasonable to assume that the benefits of an endovascular approach will be
even greater when applied to patients with juxta, pararenal, or thoracoabdominal
aneurysms. (20,21) It is well known that, due to their age and
comorbidities, especially these patients have a limited life expectancy beyond
surgery. It could be argued, then, that quality of life is a better metric for
evaluating outcomes than survival.
Ethical considerations
The protocol was approved by the Ethics Institutional
Board.
Limitations
As limitations, this was a mid-term follow-up study
and in the context of a pandemic, which partially hindered patient follow-up.
It is also worth highlighting the number of patients
analyzed (50 patients) which, while being a representative value for our
country, does not allow us to arrive to robust recommendations, but to
demonstrate the possible advantages of centralizing pathologies based on
experience and applied technology.
CONCLUSIONS
In conclusion, this presentation shows a global
approach in which different techniques do not oppose but rather complement each
other to achieve mid-term effective and long-lasting treatment in patients with
complex aortic aneurysms. The goal is not to compare the techniques, since they
have different indications, but rather to seek a final result, which is the
minimally invasive treatment of patients with great technical complexity.
Conflicts of interest
None declared.
(See authors’ conflict of interests
forms on the web).
Financing
None.
![]() https://creativecommons.org/licenses/by-nc-sa/4.0/
https://creativecommons.org/licenses/by-nc-sa/4.0/
©Revista
Argentina de Cardiología
1. Lederle
FA, Freischlag JA, Kyriakides
TC, Padberg FT Jr, Matsumura JS, Kohler TR, et al. Outcomes following endovascular vs
open repair of abdominal aortic aneurysm: a randomized trial. JAMA 2009;302:1535-42. https://doi.org/10.1001/jama.2009.1426
2. Huang Y,
Glovinsky P, Oderich GS,
Duncan AA, Kalra M, Fleming MD y col. Outcome after
open and endovascular repairs of abdominal aortic aneurysm in mathed cohorts using propensity score modeling. J Vasc Surg 2015;62:304-311.
https://doi.org/10.106/j.jvs.2015.02.039.
3. Lai BK,
Zhou W, Li Z, Kyriakides T, Matsumura J, Lederle FA, et al; OVER Veterans Affairs Cooperative Study
Group. J
Vasc Surg 2015;62:1394-404. https://doi.org/10.1016/j.jvs.2015.02.003.
4. Escobar
GA, Oderich GS, Farber MA, de Souza LR, Quinones- Baldrich WJ, Patel HJ, et al; NACAAD Investigators. Results of the North American Complex Abdominal Aortic Debranching (NACAAD) Registry. Circulation. 2022;146:1149-58. https://doi.org/10.1161/CIRCULATIONAHA.120.045894.
5. Locham S, Dakour-Aridi H, Nejim B, Dhaliwal J, Alshwaily W, Malas M. Outcomes
and cost of open versus endovascular repair of intact thoracoabdominal
aortic aneurysm. J
Vasc Surg 2018;68:948-55.e1. https://doi.org/10.1016/j.jvs.2018.06.211
6. Locham S, Dakour-Aridi H, Bhela J, Nejim B, Havana Challa A, Malas M. Thirty-Day
Outcomes of Fenestrated and Chimney Endovascular Repair and Open Repair of Juxtarenal, Pararenal, and
Suprarenal Abdominal Aortic Aneurysms Using National Surgical Quality
Initiative Program Database (2012-2016). Vasc Endovasc Surg 2019;53:189-98. https://doi.org/10.1177/1538574418819284.
7. Zettervall SL, Tenorio ER, Schanzer A, Oderich GS, Timaran CH, Sweet MP. Secondary interventions after
fenestrated/branched aneurysm repairs are common and non
detrimental to long-term survival. J Vasc Surg 2022;75:1530-8.
https://doi.org/10.1016/j.jvs.2021.11.074
8. Timaran CH, Oderich GS, Tenorio ER, Farber MA, Schneider DB, Schanzer
A, et al; Aortic Research Consortium. Expanded Use of Preloaded Branched and
Fenestrated Endografts for Endovascular Repair of
Complex Aortic Aneurysms. Eur J Vasc Endovasc Surg.
2021;61:219-26. https://doi.org/10.1016/j.ejvs.2020.11.001.
9. Oderich
GS, Ribeiro MS, Sandri GA, Tenorio ER, Hofer JM, Mendes BC, et al. Evolution from physician modified to
company-manufactured fenestrated-branched endografs
to treat pararenal and thoracoabdominal
aortic aneurysms. J Vasc Surg
2019;70:31-42.e7. https://doi.org/10.1016/j.jvs.2018.09.063.
10. Schanzer A, Greenberg RK, Messina L. Predictors of
abdominal aortic aneurysm sac enlargement after endovascular repair. Circulation
2011;123:2848-55. https://doi.org/10.1161/CIRCULATIONAHA.110.014902
11. Chait J, Tenorio ER, Mendes BC,
Barbosa Lima GB, Marcones GB, Oderich
GS. Impact of gap distance between fenestration and aortic
wall on target artery instability following fenestrated-branched endovascular
aortic repair. J Vasc Surg
2022 Jul;76(1):79-87. https://doi.org/10.1016/j.jvs.2022.01.135
12. Ferreira LM ,
Ferrer M, Zambrano A, Cohen Arazi H, La Mura R.
Marcadores a largo plazo para la endofuga tipo I
proximal. https://doi.org/10.20960/angiologia.00040.
13. Konstantinou
N, Kölbel T, Dias NV, Verhoeven E, Wanhainen A, Gargiulo M, et al. Revascularization of occluded renal artery stent grafts after complex
endovascular aortic repair and its impact on renal function. J Vasc Surg. 2021;73:1566-72.
https://doi.org/10.1016/j.jvs.2020.09.036.
14. Jordan WD, Mehta
M, Varnagy D, Moore WM, Arko
FR, De Vries JP. Results of the ANCHOR prospective, multicenter registry of EndoAnchors for type Ia endoleaks and endograft migration
in patients with challenging anatomy. J Vasc Surg 2014;60:885-92. https://doi.org/10.1016/j.jvs.2014.04.063
15. Wu WW, Swerdlow NJ, Dansey K, Shuja F, Wyers MC, Schermerhorn ML. Surgical Treatment patterns and clinical
outcomes of patients treated for expanding aneurysm sacs with type II endoleaks after endovascular. J Vasc
Surg 2021;73:484-93. https://doi.org/10.1016/j.jvs.2020.05.062
16. Fazzini S, Martinelli O, Torsello G, Austermann M, Pipitone MD, Torsello GF, et al. Eur the PROTAGORAS 2.0 study to identify sizing and
planning predictors for optimal outcomes in abdominal chimney endovascular J Vasc Endovasc Surg
2021; 61:591-602. https://doi.org/10.1016/j.ejvs.2020.11.019.
17. Tsilimparis N, Bosiers M, Resch T, Torsello G, Austermann M, Rohlffs F, et al. Two-year
target vessel-related outcomes following use of off-the-shelf branched endografts for the treatment of thoracoabdominal
aortic aneurysms. J Vasc Surg.
2023:S0741-5214(23)01017-0. https://doi.org/10.1016/j.jvs.2023.03.498.
18. Aucoin VJ, Eagleton MJ, Farber MA, Oderich
GS, Schanzer A, Timaran CH,
et al. Spinal cord protection practices used during endovascular repair of
complex aortic aneurysms by the U.S. Aortic Research Consortium. J Vasc Surg. 2021;73:323-30. https://doi.org/10.1016/j.jvs.2020.07.107
19.
Ferreira LM, Ferrer M, La Mura R. Staging Procedures,
Cerebrospinal Fluid Drainage, Selective Neuromonitoring,
and Use of Conduits During Complex Endovascular Aortic Repair in Patients With
High Risk of Spinal Cord Injury. J Vasc Surg 2019;70:149. https://doi.org/10.1016/j.jvs.2019.08.098
20. Chaikof EL, Dalman RL, Eskandari MK, Jackson BM, Lee WA, Mansour MA, et al. The
Society for Vascular Surgery practice guidelines on the care of patients with
an abdominal aortic aneurysm. J Vasc Surg. 2018;67:2-77.e2. https://doi.org/10.1016/j.jvs.2017.10.044.
21. Wanhainen A, Verzini F, Van Herzeele I, Allaire E, Bown M, Cohnert T, et al.
Editor’s Choice - European Society for Vascular Surgery (ESVS) 2019 Clinical Practice
Guidelines on the Management of Abdominal Aorto-iliac
Artery Aneurysms. Eur J Vasc
Endovasc Surg. 2019;57:8-93.
https://doi.org/10.1016/j.ejvs.2018.09.020.